
Abstract
Occlusion of enteral feeding tubes is a relatively common occurrence that both disrupts nutrient delivery and eliminates a route for medication administration.1-4 Clogs may result from inadequate flushing procedures, highly viscous enteral feeding formulations, denaturization of the protein of the enteral formulation, and administration of crushed or interacting medications.3,4 In one report, small-bore enteral feeding tube (eg, Dobhoff) patency was lost in 32 of 90 (35%) patients over an 8-month period. 1 Other reports cite rates of 10% to 23%,2,5 with medications being the cause of occlusion in approximately 15% of patients.6,7 Prompt restoration of tube patency reduces the clinical impact and may save health care resources devoted to tube replacement.
Various methods of clearing enteral feeding tube occlusions have been proposed in the literature; however, results have been inconsistent.1,3,8-11 Flushing the occluded tube with water is an easy and often effective initial step. In addition, cranberry juice, carbonated colas, papain, bromelain, chymotrypsin, and pancreatic enzymes have been administered in attempts to clear occluded enteral feeding tubes, using instillation dwell times ranging from 5 minutes to 4 hours. Yet the acidity of cranberry juice and carbonated colas may actually worsen occlusions, denaturing the caseinate proteins in enteral nutrition formulas.8-10
The efficacy of 9 substances in clearing 8-French enteral feeding tubes clogged with Osmolite enteral nutrition formula was evaluated in an in vitro trial. 9 Substances tested included 1 mL volumes of distilled water, cola, and cranberry juice and solutions of crushed single tablets or capsules of Viokase, Pancrease pancrelipase, pancreatin, papain, bromelain, or chymotrypsin/trypsin dissolved in 1 to 3 mL distilled water. Clearance of each solution in 3 clogged enteral feeding tubes was assessed every 30 minutes for up to 4 hours. Although the clogs moved within at least 1 of the 3 occluded feeding tubes following instillation of solutions of Viokase, Pancrease, papain, or chymotrypsin/trypsin, none of the substances cleared the tubes before 4 hours. Only tubes instilled with chymotrypsin/trypsin or papain were able to be irrigated at 4 hours.
Chymotrypsin is currently available only as an expensive pharmaceutical grade powder ($867/1 g) or as a component of multi-ingredient dietary supplements. 12 Papain, extracted from the papaya and commonly used as a meat tenderizer, is inexpensive, but in vitro trials have also not consistently documented superiority to water or other agents.8,9 The efficacy of relatively expensive commercially available products (eg, Clog Zapper) containing pancreatic enzymes and papain have not been documented in published trials. 3
In 1989, Marcuard et al 8 compared the efficacy of several substances for clearing occluded enteral feeding tubes, including an alkalinized pancreatic enzyme solution compounded by mixing 1 crushed Viokase (lipase 8000 units, amylase 30 000 units, and protease 30 000 units) tablet with 5 mL water and increasing the pH to 7.9 with sodium hydroxide solution. In a blinded assessment, the alkalinized Viokase solution was more effective (P < .01) at clearing Dobhoff (8-French) tube obstructions in vitro than pH-adjusted distilled water (pH = 7.9), carbonated colas, papain, or plain Viokase (ie, not pH adjusted). Following failure of a water flush, alkalinized Viokase solution (pH = 7.9) successfully restored patency to occluded enteral feeding tubes in 7 of 10 patients.
In a subsequent prospective clinical trial, a solution of 1 Viokase tablet crushed with 1 sodium bicarbonate 324 mg tablet dissolved in 5 mL warm water was instilled into 32 occluded 8-French Dobhoff tubes not cleared by water alone. 1 After clamping for 5 minutes, the tube was flushed with water. This protocol was effective at clearing 23 of the 32 (71.9%, P < .01 compared to water) occluded tubes. When 8 tubes obstructed as a result of factors unrelated to the feeding formula (eg, kinked tubes and impacted tablet powder) were excluded, the efficacy rate increased to 95.8%.
Viokase tablets were previously stocked by the University of Michigan Health System (UMHS) Department of Pharmacy Services for clearing occluded feeding tubes according to the procedures described by Marcuard et al. 1 However, in 2010, Viokase and several other pancreatic enzyme products were removed from the US market as unapproved drugs.13,14 After April 2010, just 3 pancreatic enzymes remained on the market: Creon, Pancreaze, and Zenpep. These products consist of encapsulated enteric-coated beads formulated for delayed release in the duodenum for their FDA-approved indications—the treatment of exocrine pancreatic insufficiency caused by conditions such as cystic fibrosis, chronic pancreatitis, and pancreatectomy.15-17
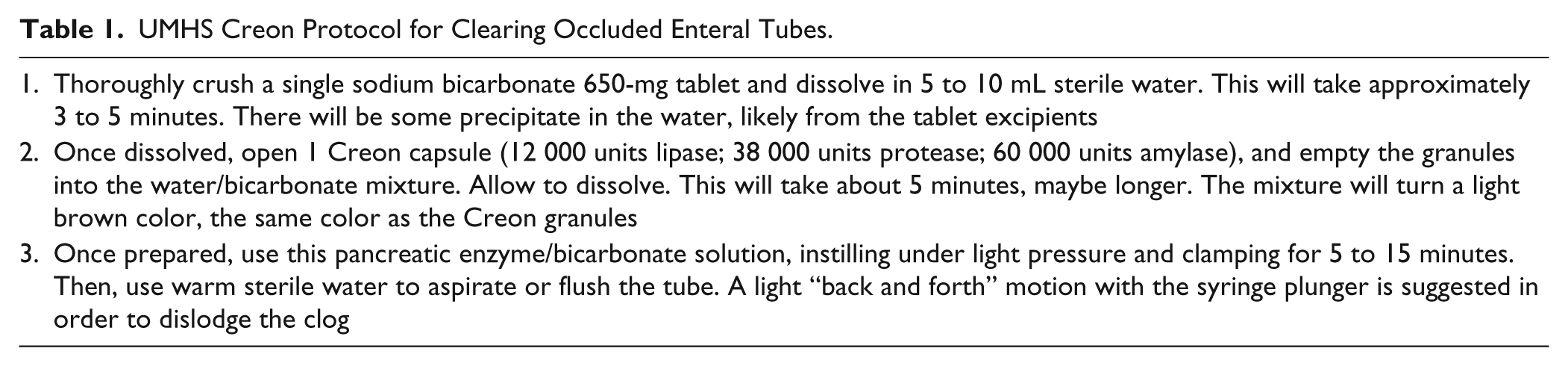
Despite the lack of published efficacy data, Creon delayed-release capsules containing lipase 12 000 units, protease 38 000 units, and amylase 60 000 units replaced Viokase tablets in the protocol for clearing occluded enteral feeding tubes, with the dose of sodium bicarbonate increased in consideration of the enteric coating of Creon (Table 1). The objective of this retrospective, quality assurance study was to evaluate the efficacy of this adjusted protocol.
UMHS Creon Protocol for Clearing Occluded Enteral Tubes.
Methods
Adult and pediatric patients admitted to UMHS or seen in the emergency department between May 1 and November 30, 2010, who were prescribed Creon delayed-release capsules for an occluded enteral feeding tube were identified through the Department of Pharmacy Services dispensing database and included in this retrospective study. Patients who did not receive the prescribed dose of Creon delayed-release capsules (ie, either the standard 12 000 units lipase or another dose) or received Creon for another indication were excluded. Data were collected from electronic medical records by 3 investigators (KD, RMK, and JV) and subsequently reviewed by 1 investigator (KD) to ensure consistency and completeness of recorded data. Data collected included the following: (1) patient demographics (age, sex, weight, medical service, type of enteral feeding tube, and enteral formula administered); (2) cause of clog; (3) number of clearance attempts with the Creon protocol; (4) whether or not Creon was effective in clearing the occlusion; (5) other documented tube-clearing procedures attempted; (6) subsequent intervention if the Creon protocol failed (eg, tube removed, tube replaced); and (7) any adverse effects attributed to the Creon protocol as recorded in the medical record. All data collection was conducted in compliance with the Health Insurance Portability and Accountability Act (HIPAA) of 1996. This study was approved by the University of Michigan Institutional Review Board.
Descriptive statistics were applied to the demographic characteristics of the patients and to outcomes. The primary outcome parameter, the efficacy of the Creon protocol, was based on documentation in the medical record of tube clearance or resumption of enteral feedings with no note regarding tube replacement. Efficacy was reported as the percentage of occluded tubes successfully cleared. The Creon protocol was deemed a failure if the occluded tube was removed and/or replaced following administration of the pancreatic enzyme solution. The effect of the dose of Creon administered on outcome was analyzed using the Fisher’s exact test.
Results
A total of 104 patients with 155 obstructed enteral feeding tubes met the inclusion criteria within the 7-month study period. Of these, 21 patients with 37 clogged tubes were excluded because administration of the prescribed Creon was not documented. The remaining 83 patients collectively experienced 118 cases of tube occlusion; however, 3 patients were subsequently excluded from the efficacy analysis because of inadequate documentation of treatment outcome.
The patient population was 54.2% male and 45.8% female. The median age was 55 years (range = 2 months to 93 years). The Creon protocol was administered in the emergency department to 6 of the 83 patients (7.2%). Another 33 (39.8%) and 44 (53.0%) patients received Creon while admitted to medical and surgical services, respectively. Osmolite was the most frequently administered enteral feeding solution in the study population. A variety of enteral feeding tubes were represented in this study. The most frequently occluded were Dobhoff (43 of 83, 51.8%), jejunostomy (15 of 83, 18.1%), and percutaneous endoscopic gastrostomy (PEG; 11 of 83, 13.3%) tubes.
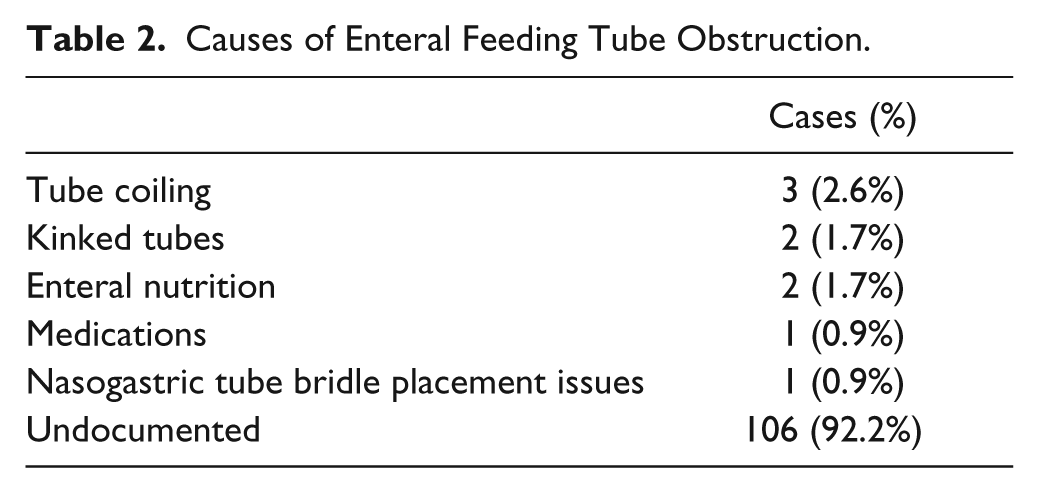
Overall, the Creon protocol successfully cleared the occluded feeding tube in 53 of the 115 evaluable cases (46.1%). Causes of obstruction were infrequently documented but included tube coiling in the esophagus or stomach and kinked tubes (Table 2). When 5 tube occlusions caused by mechanical problems not cleared by pancreatic enzyme treatment were excluded, the Creon protocol demonstrated success in clearing 53 of 110 tubes, a clearance rate of 48.2%.
Causes of Enteral Feeding Tube Obstruction.
The dose of Creon administered as part of the protocol was most commonly 12 000 lipase units (112 of 121 doses, 92.6%) but ranged from 6000 lipase units (6 of 121 doses, 5.0%) to 24 000 lipase units (3 of 121 doses, 2.5%). In 5 cases, Creon administration was repeated after the initial dose was ineffective. The second attempt successfully cleared 3 tubes but was unsuccessful in 2 cases. In one of these patients, the procedure was repeated a third time but was again unsuccessful, with subsequent tube replacement. There was no significant difference in outcome based on the initial dose of Creon administered.
Flushing of the occluded tubes with water was often documented. In addition, several other methods to clear the clogs were attempted prior to or following administration of Creon solution, including instillation of coffee, cola drinks, or normal saline. Following Creon failure, the alternative method was also not effective in clearing the obstruction in 10 of 13 (76.9%) cases, and the tube was subsequently removed or replaced. Enteral feeding tube removal or replacement was documented in 11 (17.7%) and 36 (58.1%) of 62 cases, respectively. Documentation regarding the remaining 15 of 62 (24.2%) occluded tubes not cleared with the Creon protocol was not available. No adverse effects were attributed to Creon administration.
Discussion
Enteral feeding tubes are generally described according to their insertion sites and the location of their distal tips (eg, nasogastric and PEG).4,7 Small-bore enteral tubes (5-12 French lumen diameter) are frequently used in hospital settings to provide a means for short-term delivery of enteral nutrition and medications. The Dobhoff tube is a commonly used small-bore enteral feeding tube that may be inserted nasally, with the end of the tube lodged in either the stomach or the small bowel. Although more comfortable for the patient, the narrow lumens of small-bore enteral feeding tubes are more likely to become occluded by viscous enteral nutrition formulas or crushed medications than larger-bore, stiffer enteral feeding tubes (eg, PEG tubes).
Many substances have been advocated anecdotally for instillation into clogged enteral feeding tubes, although clinical support is generally sparse.1,3,8-11 In light of the results of an in vitro direct comparison and a subsequent clinical trial reporting a high degree of efficacy, use of alkalinized solutions of Viokase tablets have largely been recommended over other agents for clearing enteral feeding tubes in clinical practice.1,3,4,8
Following the market withdrawal of Viokase pancreatic enzyme tablets, UMHS procedures for clearance of enteral feeding tube occlusions were adapted to incorporate Creon delayed-release capsules. A standard solution of Creon delayed-release capsules crushed with sodium bicarbonate was implemented in our hospital as a result of the proven superiority of alkalinized pancreatic enzymes for this indication. 8 To prevent enzyme inactivation in the low pH of the stomach, Creon consists of encapsulated enteric-coated spheres designed to release enzymes at a pH of 5.5 or higher. 17 The pH of the protocol solution was not measured; however, the calculated pH of a solution of 650 mg of sodium bicarbonate in 5 to 10 mL of water exceeds 10. Another encapsulated formulation, Zenpep, dissolved in 5 mL of sodium bicarbonate solution and warm water was similar in efficacy, in vitro, to water in disrupting clogs made by mixing calcium caseinate with hydrochloric acid. 11 However, to our knowledge, the present study is the first clinical assessment of delayed-release pancreatic enzymes for clearing occluded enteral feeding tubes.
In this 7-month, retrospective study, the UMHS Creon-based protocol cleared 48.2% of 110 enteral feeding tubes occluded by nonmechanical causes. In contrast, the published efficacy of a Viokase protocol was nearly twice as high—95.8%—when mechanical occlusions were excluded. 1 Differences in study population and design may have contributed to these disparate results. The study by Marcuard et al 8 included only patients with Dobhoff tubes, whereas a wide variety of enteral feeding tubes were included in the present assessment. Yet just 40% of the subset of 55 Dobhoff tubes were cleared with the UMHS Creon protocol. Although the content of Viokase tablets (8000 lipase units, 30 000 protease units, and 30 000 amylase units) differed from that of Creon delayed-release capsules (12 000 lipase units, 38 000 protease units, 60 000 amylase units), the higher enzyme content per dose, especially the protease component, would be anticipated to favor the efficacy of Creon. Efficacy appeared to be dose-related, with those receiving initial Creon doses of 6000, 12 000, and 24 000 lipase units achieving tube clearance rates of 20%, 46%, and 67%, respectively. However, these differences in outcome between doses did not achieve statistical significance.
The design of the present study confers both advantages and limitations with respect to interpretation and application of the results. The retrospective design differs from the prospective methodology of the clinical study by Marcuard and Stegall 1 and likely accounts for some of the differences in documented effectiveness. Our retrospective evaluation allowed a more real-world assessment of the efficacy of the protocol. Whereas a variety of nursing staff prepared and administered the enzyme solution in UMHS during the study period, members of a nutrition support team were involved in these aspects of the Marcuard study. Having fewer staff who are potentially better trained regarding the tube clearance study procedures would be expected to improve consistency of the administration of enzyme doses. In fact, the lack of consistency in the present assessment is apparent in the variability of the doses of Creon ordered. This is despite the standard UMHS tube clearance guidelines specifying use of the Creon 12 000 lipase unit dosage strength. Concern regarding the lack of consistency also extends to preparation procedures. Whereas Viokase tablets were readily solubilized after crushing, more than 5 minutes might be required for complete dissolution of the enteric-coated beads of Creon capsules. Incomplete dissolution of the Creon delayed-release capsules for some doses could have resulted in insufficient amounts of enzymes available to act on the clog. In addition, although the optimal dwell time remains unclear, the 5- to 15-minute time frame advocated in the UMHS protocol may not have been consistently adhered to.
In March 2012, the FDA approved Viokace, a pancreatic enzyme tablet that differs in content from the discontinued Viokase tablets despite the similar name. 18 The availability again on the market of a tablet formulation of pancreatic enzymes that is not enteric coated or delayed release is compelling, in that concerns regarding inadequate dissolution and inherent stickiness of the enteric coating of Creon beads are eliminated. However, further research is needed to determine if efficacy may be improved with use of crushed Viokace over that documented with the Creon-based tube clearance protocol.
The retrospective nature of the study may have affected the results because of potential lack of standardization of enzyme preparation and administration techniques. This evaluation was also limited by the completeness of information available in the electronic medical record. For example, the causes of the occlusions (eg, enteral tube feedings, medications, and kinked tube) were not always recorded. Because pancreatic enzymes would not be expected to resolve mechanical occlusions, inadequate documentation and subsequent inclusion of these cases in the efficacy analysis would decrease the calculated clearance rate. In addition, assumptions were made regarding the success or failure of the Creon protocol when not explicitly noted in the medical record. Tube replacement was regarded as an indication of failure of the Creon protocol; resumption of enteral tube feedings was assumed to indicate successful clearance of the clog. Both assumptions, if incorrect, would affect the study results.
Conclusion
This 7-month retrospective, quality assurance study of a protocol using alkalinized Creon delayed-release capsules documented clearance of 53 of 110 (48.2%) evaluable occluded enteral feeding tubes, excluding those occluded as a result of mechanical causes. This clearance rate is much less than that documented in a published prospective study using a pH-adjusted solution compounded from Viokase pancreatic enzyme tablets, perhaps because of differences in pancreatic enzyme formulation and study design. In light of these results, a change from Creon delayed-release capsules to the newly marketed Viokace tablets in the standard protocol for occluded enteral feeding tubes is under evaluation. An assessment of the modified protocol is planned.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
Previously presented as a poster at the American Society of Health-System Pharmacists Midyear meeting; Las Vegas, NV; December 3, 2012. At the time of this study, Drs. Kurian, Vuong, and Dang were students of the University of Michigan College of Pharmacy.