
Abstract
Keywords
Introduction
Substantial morbidity and mortality is attributed to acute respiratory infections (ARIs). 1 These infections range in severity from self-limited sinusitis to pneumonia, the latter of which is the fourth most common cause of death worldwide. With the advent of sensitive molecular assays, paramyxoviruses such as respiratory syncytial virus (RSV), human metapneumovirus (hMPV), and parainfluenza virus (PIV) are increasingly being recognized as significant primary causes of and contributors to ARIs.2-4 Middle East respiratory syndrome coronavirus (MERS-CoV) is also of significant concern, given the high mortality rate and ongoing outbreaks, primarily affecting individuals who travel within the Arabian Peninsula.5,6
The severity of noninfluenza respiratory viral infections (NIRVIs) is dependent on patient factors such as immune function, the presence of preexisting cardiopulmonary disease or other comorbidities, and the intrinsic virulence of the infecting viral species. 7 In profoundly immunocompromised populations such as hematopoietic stem cell transplant (HSCT) recipients, the mortality rate for RSV lower respiratory tract infection (LRTI) ranges between 7% and 83%. 8 Similarly, in lung transplant recipients, the mortality rate for paramyxovirus ARIs has been estimated to be between 10% and 20%. 9
With the recognition of the burden of NIRVIs and a paucity of active treatment options, ribavirin has been increasingly used, specifically in immunocompromised or severely ill patients.10-13 Ribavirin, a guanosine analogue with activity against a broad spectrum of RNA and DNA viruses, is available in oral and aerosolized formulations in the United States.14,15 Ribavirin inhalation is Food and Drug Administration (FDA) approved for the treatment of RSV in pediatric patients, whereas oral ribavirin is only FDA approved for the treatment of hepatitis C. Because aerosolized ribavirin is associated with bronchospasm, requires special isolation procedures because of teratogenicity risk to pregnant health care workers/visitors, and is very expensive, oral ribavirin has been used as a therapeutic option in the treatment of NIRVIs.11-13 Unfortunately, published data on the use of oral ribavirin for the treatment of NIRVIs are limited to case reports, retrospective reviews, prospective observational studies, small nonrandomized comparative studies, and primarily immunocompromised patients with HSCT/malignancy or lung-transplant recipients.10-13,16-25 A clinical guideline from a working group of the Fourth European Conference on Infections in Leukaemia (ECIL-4) lacks a strong recommendation but suggests that intravenous immune globulin (IVIG) and aerosolized or systemic (oral or intravenous) ribavirin may be used in patients with hematological malignancy presenting with RSV or hMPV ARIs. 26 This systematic review aims to summarize the available clinical outcomes data, so that treating clinicians can make evidence-based decisions regarding the use of oral ribavirin for NIRVIs.
Methods
Literature Search
MEDLINE, EMBASE, and PubMed Central (1972 to June 1, 2015) were queried with the following search term combinations: “Oral” AND “ribavirin” AND (“respiratory syncytial virus” OR “metapneumovirus” OR “parainfluenza” OR “coronavirus” OR “rhinovirus” OR “enterovirus” OR “adenovirus”). References within each included article were evaluated for possible inclusion in the systematic review. The literature search was performed and described according to PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines. 27
Study Selection
Included studies must have characterized the clinical outcomes of a cohort of patients treated with oral ribavirin for symptomatic NIRVIs. Case reports and series with <5 cases, conference abstracts, articles evaluating severe acute respiratory syndrome coronavirus (SARS-CoV), and articles written in languages other than English were excluded. SARS-CoV studies were excluded because of ribavirin’s lack of activity against SARS-CoV. 28 The titles and abstracts of all search results were first screened for possible inclusion. The full texts of these reports were then reviewed to determine final eligibility for inclusion in the systematic review. Both authors (MLB and AEG) independently performed the literature search and study selection. Any disagreement was resolved by consensus.
Data Extraction
MLB and AEG independently extracted the following from each included study using a standardized data extraction form: authors; publication date; study location; patient demographics, including underlying immunocompromising condition(s); attributed virus; classification of NIRVI as upper-respiratory-tract infection (URTI) or LRTI; use of IVIG or corticosteroids; ribavirin treatment regimen; and clinical outcomes, including disease progression, mortality, length of stay (LOS), and ribavirin-related adverse effects. Disease progression included progression from URTI to LRTI and development of bronchiolitis obliterans syndrome (BOS). The heterogeneity of study populations and study designs, combined with the lack of randomized studies, precluded meta-analysis, and thus, a narrative synthesis of study data was created.
Results
Study Selection
Figure 1 describes the literature search. Initially, 1421 articles were identified. After screening titles/abstracts and removing duplicates, the full texts of 196 articles were reviewed to determine final eligibility.
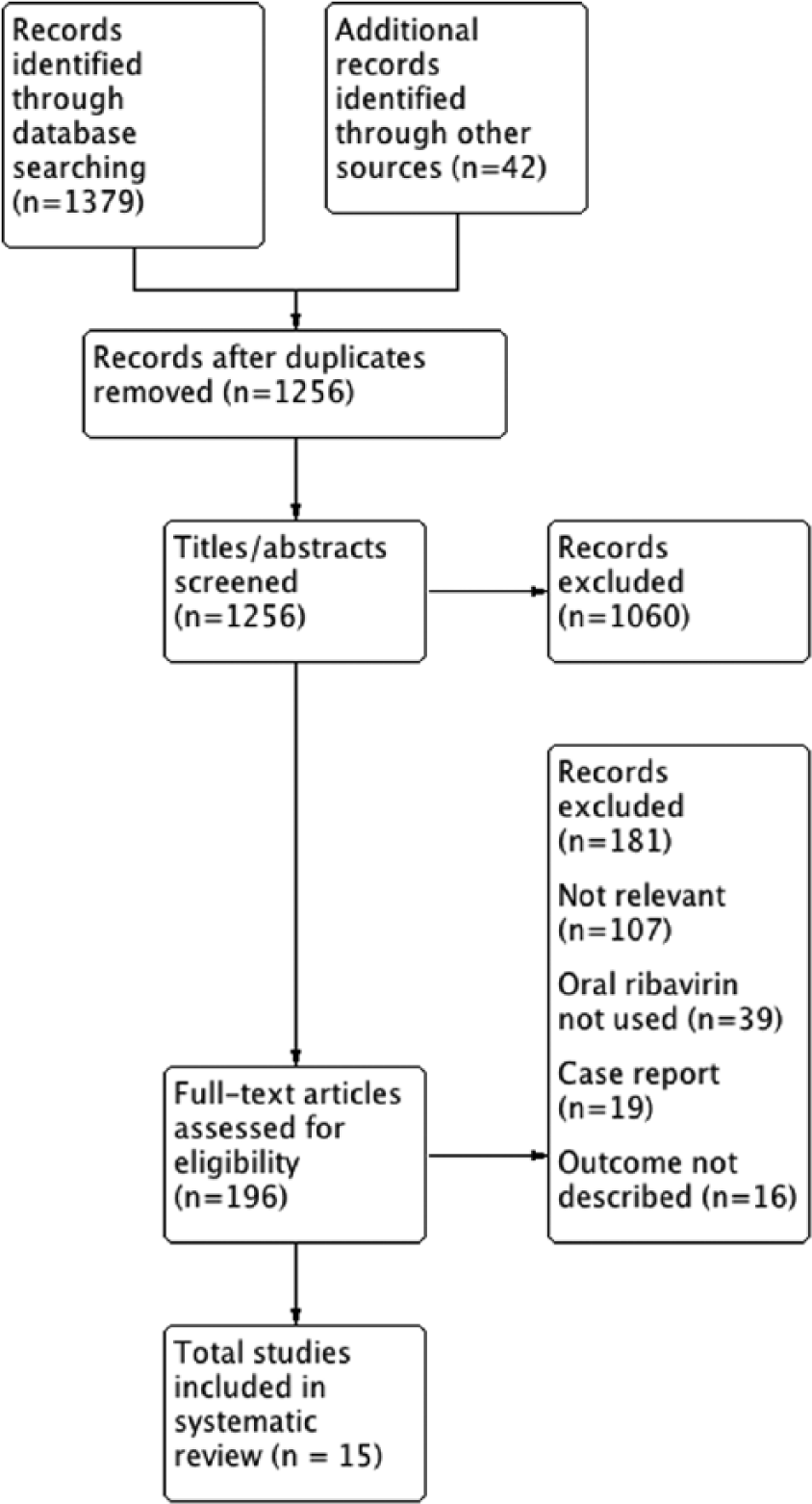
Study identification, inclusion, and exclusion.
Study and Patient Characteristics
Table 1 presents the abstracted data from the 15 included studies. In all, 12 retrospective and 3 prospective studies met eligibility criteria. Three studies were comparative and included control groups that did not receive ribavirin.11,13,23 One case series included pediatric patients. 16 A total of 516 cases of NIRVIs were reported in the 15 studies,10-13,16-25,29 and 31% (159/516) and 69% (357/516) of patients presented with URTIs and LRTIs, respectively. The causes of NIRVI were RSV (n = 343),10-13,16,17,19-22,24,29 PIV (n = 90),10,11,17,19,20 MERS-CoV (n = 49),23,25 and hMPV (n = 34).11,13,18 No studies with adenovirus, enterovirus, or rhinovirus met inclusion criteria. With the exception of the 2 MERS-CoV studies, all studies were in immunocompromised patient populations—primarily, studies with hematological malignancy/HSCT recipients (n = 9)10,12,13,16-21 or lung/heart-lung recipients (n = 4).11,22,24,29 Of the 516 NIRVI cases, 380 were treated with oral ribavirin. Corticosteroids and IVIG were given in 54% (281/516) and 25% (128/516) of cases, respectively.
Summary of Publications of Oral Ribavirin for Noninfluenza Respiratory Viral Infections.

Abbreviations: ADR, adverse drug reaction; AML, acute myeloid leukemia; BOS, bronchiolitis obliterans syndrome; GVHD, graft-versus-host disease; Hgb, hemoglobin; hMPV, human metapneumovirus; HSCT, hematopoietic stem cell transplant; IV, intravenous; IVIG, intravenous immunoglobulin; LD, loading dose; LOS, length of stay; LRTI, lower-respiratory-tract infection; MERS-CoV, Middle East respiratory syndrome coronavirus; NG, nasogastric; non-RBV, ribavirin untreated; NR, not reported; OR, odds ratio; PIV, parainfluenza virus; PIV3, parainfluenza virus type 3; RBV, ribavirin; RSV, respiratory syncytial virus; URTI, upper-respiratory-tract infection.
Denominator is all patients in study, unless otherwise indicated.
Denominator is patients who received oral ribavirin.
Only patients who received oral ribavirin as initial primary therapy; number of IV switched to oral not reported.
Moderate immunodeficiency: HSCT >6 months from RSV diagnosis, GVHD (<2), receiving maintenance immunosuppression, T or B cell depletion >3 months from RSV diagnosis.
Severe immunodeficiency: HSCT ≤6 months from RSV diagnosis, GVHD (grade ≥2), T or B cell depletion ≤3 months from RSV diagnosis, leukopenia, lymphopenia, or hypogammaglobulinemia.
10 Cases in 7 patients.
Clinical Outcomes: Immunocompromised Patients
Oncology/HSCT Patients or Other Immunosuppression
Park et al 13 conducted a single-center, retrospective study evaluating clinical outcomes of 145 patients with hematological disease with RSV, hMPV, or PIV ARI. Oral ribavirin treatment was initiated in 114 patients at the discretion of the attending physician. A nested propensity-matched case-control analysis was performed in 21 pairs of ribavirin-treated and untreated patients with similar baseline age (median 55 and 50 years, respectively), immunosuppressant and methylprednisolone use, transplant type (predominantly sibling allogeneic HSCT), and underlying diagnoses. More than half presented with LRTI, had ultimately fatal disease according to McCabe score, and were on methylprednisolone therapy. In both the unadjusted and propensity score–matched analyses, no difference in mortality was found at any time point (7, 14, or 30 days) or specifically for underlying respiratory death between oral ribavirin and untreated control groups. However, the matched analysis was underpowered, with only 21 patients in each arm. Corticosteroid use was an independent predictor of mortality (adjusted odds ratio [OR] = 5.67; 95% CI = 1.97-16.33).
Lehners et al 21 conducted a retrospective study to identify factors that influenced outcomes in 56 patients with RSV ARI in an oncology/HSCT unit. The cohort was severely ill, with 71% of patients eventually developing LRTI and 35% of those experiencing mortality. In multivariate analysis, oral ribavirin was protective for mortality (OR = 0.14; 95% CI = 0.02-0.92). Most patients who died (79%) were coinfected with other viral, bacterial, or fungal infections, thus, limiting conclusions about the influence of RSV on their death.
Marcelin et al 12 reported a cohort of 34 immunosuppressed patients primarily with hematological malignancy (74%) and lung transplant (9%) treated with oral ribavirin for RSV ARI. Of these patients, 71% presented with LRTI; 38% were managed in the intensive care unit (ICU), and 18% required mechanical ventilation. Despite the cohort having moderate/severe illness, no mortality was attributed to RSV per the study authors. However, 2 patients likely died from respiratory failure, one with concomitant disseminated Elizabethkingia infection and a second with respiratory failure who transitioned to palliative care.
Khanna et al 20 retrospectively evaluated the outcomes of RSV ARI in 34 patients with hematological malignancy, 79% of whom were HSCT recipients. One-third of patients presented with URTIs, 15% were admitted to the ICU, and 12% required mechanical ventilation. Oral ribavirin was used in 25 (74%) patients; all of these patients received IVIG cotherapy, and 13 received palivizumab. Diagnosis of LRTI at presentation, pre-engraftment status, and classification as severely immunocompromised were predictive of RSV-related mortality, which occurred in 18% of patients. Progression to LRTI occurred in 2 patients, both of whom were classified as severely immunocompromised and received oral ribavirin. A surrogate for ribavirin effectiveness, RSV viral load, was measured from serial nasal secretions in 19 patients who received oral ribavirin, and a >2 log10 copies/mL decrease was appreciated in 58% and 90% of patients at 7 and 14 days, respectively.
Multiple small case series of patients with HSCT/malignancy were identified; the abstracted data are included in Table 1.10,16-19 Briefly, Egli et al 18 summarized the clinical presentation and course of 8 HSCT recipients with hMPV LRTI. Seven patients (87.5%) were hospitalized, 6 patients received oral ribavirin, and 1 ribavirin-treated patient required ventilatory support and died. Casey et al 10 reviewed the outcomes related to RSV and PIV ARI in 15 patients post-HSCT treated with oral ribavirin and IVIG. Three patients died, all with RSV. All 7 patients who presented with a URTI progressed to a LRTI, and the authors attributed this to an inadequate initial oral ribavirin dose of 10 mg/kg/d. Chakrabarti et al 17 presented the outcomes related to RSV and PIV URTI in 10 allogeneic HSCT patients who received oral ribavirin. Three patients, all with PIV, escalated therapy from oral to IV ribavirin (2 patients) or oral to aerosolized and then IV ribavirin (1 patient) because of nonresponse. The only death was in a patient who received oral then IV ribavirin for PIV. Guellar et al presented a case series that included 5 patients who received oral ribavirin for RSV URI. 19 No progression to LRTI or mortality occurred. Unlike patients with URTI, all 5 patients with LRTI received IV ribavirin for 10 days with or without subsequent oral ribavirin.
Pediatric patients were evaluated in the case series by Anak et al. 16 Five of the 6 included patients in an oncology ward received oral ribavirin and IVIG for the treatment of RSV LRTI. Three patients were receiving consolidation chemotherapy for acute myeloid leukemia or acute lymphocytic leukemia; 1 patient post–bone marrow transplant for hyper-IgM syndrome had chronic graft versus host disease; and 1 patient was receiving chemotherapy for neuroblastoma. All patients survived; however, 2 patients required retreatment with oral ribavirin because of a return of respiratory symptoms after 2 weeks.
Lung/Heart-Lung Transplant Recipients
The study by Li et al 22 was the only study comparing oral with aerosolized ribavirin for RSV ARI. This retrospective study of lung/heart-lung transplant recipients compared survival in 15 patients who received aerosolized ribavirin with that in 6 patients given oral ribavirin. There were no significant baseline differences between the treatment groups. Most patients presented with LRTI (67% and 53% in oral and aerosolized groups, respectively); 67% and 100% of patients receiving oral and aerosolized ribavirin were hospitalized, respectively (P = 0.07). There was no mortality at 30 days, and survival between treatment groups at the end of follow-up was not different (P = 0.42). Two patients (13%) in the aerosolized group and no patients in the oral ribavirin group had BOS progression at 6 months postinfection (P > 0.99). Notably, median follow-up time was 1.5 and 2.9 years in the oral and aerosolized ribavirin groups, respectively (P < 0.01). Given the different at-risk observation periods, there is a risk of differential misclassification bias and type 2 error if patients who received oral therapy experienced BOS or mortality between 1.5 and 2.9 years.
Fuehner et al 11 conducted a prospective, observational study evaluating clinical outcomes of RSV, hMPV, and PIV ARI in lung/heart-lung recipients who received oral ribavirin (n = 38) versus those who did not because of contraindications (n = 29). 11 There were no baseline differences in age, time since transplantation, transplantation type, or immunosuppressive regimen among treatment groups. Most patients were not severely ill; 85% were treated in the outpatient setting. One patient infected with hMPV who received oral ribavirin died. Graft function recovery at 30 days was higher in the oral ribavirin group (84% vs 59%, P = 0.02), and new onset BOS occurred less frequently (5% vs 24%, P = 0.02).
The retrospective study by Burrows et al 29 reported the outcomes of 56 cases of RSV LRTI in lung/heart-lung recipients. The mean age was 47 years, and the mean time to RSV LRTI onset was about 5.5 years posttransplant. Seven patients were managed as outpatients. No patients died, and 1 patient experienced BOS 3 months postinfection. Full lung function recovery occurred in 83% of cases at 3 months. The authors suggested that the use of oral ribavirin instead of IV ribavirin avoided a mean LOS of 6.7 days in this cohort. Compared with IV ribavirin, the authors calculated a cost savings of $11 696 per RSV LRTI episode treated with oral ribavirin.
Pelaez et al 24 reported 5 lung transplant recipients treated with oral ribavirin for RSV LRTI who experienced a >10% decline in FEV1 (forced expiratory volume in 1 s); all patients survived with return to baseline of FEV1, and none developed BOS during the 1.5-year follow-up period. Finally, 3 patients in the study by Marcelin et al 12 were lung transplant recipients, and all survived RSV ARI after treatment with oral ribavirin.
Clinical Outcomes: Immunocompetent Patients
MERS-CoV Pneumonia
Omrani et al 23 conducted a retrospective cohort study in ventilated immunocompetent adults with MERS-CoV pneumonia comparing clinical outcomes in patients who received oral ribavirin plus interferon-α2a (n = 20) with a control group that received supportive care (n = 24). Patients received supportive care if treated prior to September 16, 2013, or consent was declined. Patients were critically ill with a mean Acute Physiology and Chronic Health Evaluation II (APACHE II) score of 27, and groups were generally well matched. Median time to ribavirin and interferon initiation in the treatment group was 3 days after MERS-CoV diagnosis. Survival rates after MERS-CoV diagnosis for treated versus untreated patients were 70% versus 29% at 14 days (P = 0.004) and 30% versus 17% at 28 days (P = 0.054), respectively. Selection bias was minimized through outcomes blinding at the time of matching assessments. This study suggests that decreased mortality may be associated with the use of oral ribavirin; however, the nonrandomized design limits any definitive conclusion about the effectiveness of ribavirin for MERS-CoV.
Al-Tawfiq et al 25 reported a case series of 5 critically ill adults who received oral ribavirin, interferon-α2b, oseltamivir, and corticosteroids for MERS-CoV pneumonia. Median time to initiation of ribavirin was 19 days after hospital admission, and all patients died from respiratory and multiorgan failure, reflecting the often delayed identification of the virus and severity of MERS-CoV infection.
Ribavirin Adverse Effects
All studies except that of Anak et al 16 reported on adverse effects associated with ribavirin. Ribavirin therapy was discontinued in 4% (15/375) of patients because of adverse effects; 11 studies reported hemolysis caused by ribavirin (14%; 54/375 patients), ranging in severity from mild anemia to severe hemolytic anemia and lactic acidosis, requiring blood transfusions and ribavirin discontinuation.11-13,17,18,20,22-25,29 Omrani et al 23 noted a mean decrease in hemoglobin of 4.3 g/L and 2.1 g/L in ribavirin-treated and untreated patients, respectively (P = 0.002). Despite the difference in mean hemoglobin decrease, there was no difference in the need for blood transfusions. Chakrabarti et al 17 noted that all patients receiving at least 2 weeks of ribavirin experienced anemia. Adverse effects occurring in <2% of patients included the following: nephrotoxicity (n = 6), nausea (n = 3), pancreatitis (n = 2), drug rash (n = 1), altered mental status (n = 1), and liver injury (n = 1).
Oral Ribavirin Dosing
The FDA-approved oral ribavirin dosing for the treatment of hepatitis C does not exceed about 15 mg/kg/d divided twice daily. In this review, dosing differed among the studies and was dependent on local hospital protocols and/or physician preference. Also, 9 studies specified that weight-based maintenance dosing was used.10-13,16,17,20,21,24,29 Assuming an 80-kg patient, maintenance dosing typically ranged from 10 to 30 mg/kg/d, and doses were most commonly divided every 8 or 12 hours. Loading doses of ribavirin were used in 5 studies.18,20,23,25,29 Strategies for fixed escalating dosing over time and/or based on clinical response were used in 4 studies.10,17,18,20 Casey et al 10 used the lowest starting dose of 10 mg/kg/d; with this low dose, the authors observed poor response in these HSCT patients and, therefore, recommended initiating treatment at 20 mg/kg/d. In patients with MERS-CoV, the study by Omrani et al 23 used a high-dose tapering regimen with a 2-g loading dose followed by 1200 mg every 8 hours for 4 days, then 600 mg every 8 hours for 4 to 6 days. Adjustments for renal dysfunction were reported in 3 studies.12,23,29
Discussion
The treatment of NIRVIs is problematic given the dearth of treatment options. In this systematic review of 15 studies evaluating the use of oral ribavirin for the treatment of NIRVIs, we found that there were no randomized or controlled prospective studies. The primary pathogens identified were RSV and PIV, and there is very limited reported experience with the use of oral ribavirin for hMPV. We found that mortality rates related to NIRVIs were highly variable and often dependent on the underlying severity of illness. Given the lack of high-quality controlled studies and variability in NIRVI severity, the use of oral ribavirin should be based on a patient-specific risk and benefit assessment. Pediatric data are extremely limited, and we are unable to provide pediatric recommendations.
For adults with malignancy/HSCT treated with oral ribavirin for NIRVIs, the mortality ranged from 0% to 31% in the included studies. The largest study did not identify a clinical outcome benefit of oral ribavirin in unadjusted or propensity score–adjusted analyses. 13 Conversely, another study found that oral ribavirin was independently associated with survival in multivariate analysis. 21 The included reports illustrate the importance of the underlying degree of immunodeficiency and severity of illness on patient outcomes. Two studies found that more severely immunocompromised patients had a higher mortality rate.20,21 Risk factors for progression to LRTI and mortality should be assessed when deciding whether or not to treat NIRVIs. In HSCT recipients, risk factors for RSV progression to LRTI include absolute neutrophil count <500 cells/µL or lymphocytes <0.2 × 10 9 /L, mismatched/unrelated donor, allogeneic HSCT within the previous month, and older age.26,30 Similarly, mortality risk factors in this population include lymphocytes <0.2 × 10 9 /L, allogeneic HSCT within the previous month, pre-engraftment, severe immunodeficiency, and age >65 years. 26 In patients with the aforementioned risk factors, oral ribavirin should be considered in the treatment of NIRVIs.
A significant minority of patients with hematological malignancy/HSCT and NIRVI received IVIG or corticosteroids with or without oral ribavirin. There are no adequate controlled studies assessing IVIG in the treatment of NIRVIs. 8 In these patients with hematological malignancy/HSCT and NIRVI, corticosteroids were used in 36% of patients with NIRVI. It is important to note that one study in patients with hematological malignancy identified steroid use to be an independent predictor of mortality. 13 Corticosteroids have also been associated with increased mortality in patients with acute respiratory distress syndrome secondary to influenza. 31 A randomized controlled trial of dexamethasone in pediatric patients with RSV LRTI suggested that corticosteroids also did not improve patient outcomes, including duration of ventilation and LOS. 32 Given these data, we do not recommend routine use of corticosteroids for NIRVI in hematological malignancy/HSCT patients.
Previously reported RSV-related mortality rates in lung transplant recipients range from 10% to 20%. 9 However, in the current review, 30-day mortality occurred in only 0.9% (1/108) of oral ribavirin-treated lung transplant recipients; no deaths occurred in the 44 remaining oral ribavirin-untreated patients. The studies evaluating oral ribavirin in lung transplant recipients generally include a less severely ill population relative to patients with hematological malignancy/HSCT or infected with MERS-CoV.11,22,24,29
Long-term graft and patient survival in lung transplant recipients are influenced by the development of BOS, and paramyxovirus infection is associated with BOS development. 9 Aerosolized ribavirin causes treatment-limiting side effects such as bronchospasm, and in individuals with BOS or at risk of developing BOS, oral administration may result in better therapy adherence. Fuehner et al 11 found that oral ribavirin was associated with less BOS development and a greater proportion of patients with full graft function recovery at 30 days. Again, most patients were not severely ill and were managed as outpatients. In addition, Burrows et al 29 suggested that LOS and cost may be decreased by using oral ribavirin instead of intravenous or aerosolized routes. Given the improved outcomes and ease of administration, oral ribavirin should be considered for lung transplant recipients with NIRVI to decrease the time to graft function recovery, risk of BOS, and need for hospitalization. Most lung transplant patients (93%) received corticosteroids (or an increase in maintenance dose) with or without ribavirin.11,22,24,29
The case fatality rate with MERS-CoV is 37%. 33 In the included studies, patients were critically ill and had LRTI; 39/49 (80%) patients died. Omrani et al 34 found a statistically significant survival benefit at 14 days in patients treated with oral ribavirin compared with supportive care; however, there was no benefit at 28 days (P = 0.054). The negative finding at 28 days may be attributed to the small sample size. Adjunctive therapy with interferon alfa was provided to all patients who received oral ribavirin for MERS-CoV, and most also received corticosteroids and/or oseltamivir. In vitro data suggest synergistic activity against MERS-CoV with combined ribavirin and interferon alfa-2b. 35 Corticosteroids are not recommended by the World Health Organization (WHO) routinely for MERS-CoV, given the association with increased mortality in patients with influenza. 36 The WHO also does not recommend oseltamivir for MERS-CoV. Given the in vitro activity of ribavirin and the association with oral ribavirin and decreased mortality for MERS-CoV, treatment with oral ribavirin and interferon should be considered.
Adverse effects led to oral ribavirin discontinuation in 4% of patients; hemolytic anemia was the most common adverse effect and occurred at a rate similar to that reported in the product labeling (10% of patients). 15 Patients receiving oral ribavirin must be monitored for anemia and renal dysfunction. Although ribavirin has serious adverse effects, if patients are monitored, the benefits of therapy will often outweigh the risk of typically reversible adverse effects.
Given the lack of high-quality efficacy data for oral ribavirin in the treatment of NIRVI, its viability as a treatment option should be considered from a pharmacokinetic/pharmacodynamic point of view. Oral ribavirin is well absorbed, but absolute bioavailability is 64% secondary to hepatic first-pass metabolism. 15 In 600 mg single- and multiple-dose (twice-daily) studies, the maximum serum concentrations of oral ribavirin were 0.78 and 3.68 µg/mL, respectively. Although the pharmacodynamics of ribavirin for paramyxoviruses in humans is not defined, in vitro studies suggest that concentrations of 3 to 10 µg/mL inhibit RSV and PIV.37,38 Correlation of these data to humans is challenging given the significant intracellular distribution of ribavirin and unknown lung epithelial lining fluid penetration. Despite lacking pharmacokinetic and pharmacodynamic data, ribavirin affects viral loads from respiratory samples in RSV ARI. One study showed a >1 log10 RSV copies/mL decrease in patients treated with aerosolized ribavirin at days 9 to 10 compared with a >1 log10 RSV copies/mL increase in untreated patients. 39 Khanna et al 20 studied RSV viral loads in 19 patients who received oral ribavirin and observed a >2 log10 RSV copies/mL decrease in 90% of patients by day 14 of treatment. These surrogate data suggest that ribavirin is active for RSV ARI.
For patients with hematological malignancy/HSCT and ARI caused by RSV or PIV, the ECIL-4 guideline suggests a loading dose of 600 mg, followed by 200 mg every 8 hours the first day, 400 mg every 8 hours the second day, and then escalating daily to a maximum of 30 mg/kg/d; this regimen was adapted from the study by Khanna et al.20,26 In this review, a larger loading dose of 2 g was used for patients with MERS-CoV infections.25,34 Loading doses were not given to lung/heart-lung recipients; a 15- to 20-mg/kg/d maintenance dose was generally required for these patients, for a median duration ranging from 5 to 14 days.11,22,24 Conversely, patients with hematological malignancies/HSCT received treatment for longer periods, with a median of 14 to 26 days.
Viral shedding persists for weeks, and cessation of viral shedding is not likely useful for dictating therapy duration; antigen positivity is present from 2 to up to 7 weeks after diagnosis and may be from nonviable virus.12,16,21 Given favorable outcomes despite persistence in viral shedding and the studied durations of therapy, it is reasonable to treat HSCT and lung transplant recipients with oral ribavirin for 5 to 10 days or until symptom resolution. For both these immunocompromised populations, we suggest a starting dose of 20 mg/kg/d divided every 8 to 12 hours and avoiding doses of ≤10 mg/kg/d because low doses may be associated with poor response. 10 Dosing for MERS-CoV may be based on the Omrani et al 34 study, with the duration based on symptom resolution; however, more data are needed to establish the optimal dosing regimen for all patients with NIRVI.
This systematic review has some limitations. Although multiple electronic databases were searched, it is possible that some reports were not identified. Data from case reports and series with <5 cases, although limited, were excluded. The nonrandomized nature of included studies disallows a causal inference regarding the efficacy of oral ribavirin for NIRVIs, and only a single study compared oral ribavirin with aerosolized ribavirin. 22 The included comparative studies were generally conducted in a single center and lacked statistical power. A minority of patients within the studies had ARI secondary to multiple pathogens, which may have influenced outcomes. Only one publication included pediatric patients, and none included immunocompetent adults with paramyxovirus ARI.
Conclusion
The currently available evidence supporting the use of oral ribavirin for NIRVI is not based on high-quality studies. Randomized controlled trials are needed to determine the efficacy of oral ribavirin for NIRVI. Unfortunately, randomized studies evaluating NIRVI have been prohibitively difficult to conduct; one multicenter study was terminated early because of futility, with a slow patient enrollment rate of 14 patients in 5 years. 40 Current evidence suggests that some benefit is derived from the use of oral ribavirin in patients with NIRVI.11,21,34 Oral ribavirin should be considered for the treatment of NIRVI in immunocompromised adults (malignancy/HSCT or lung transplant) or adults with MERS-CoV.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of our routine work.