
Abstract
Introduction
Staphylococcus aureus is a prevalent pathogen in many infections, including acute bacterial skin and skin structure infections (ABSSSIs), pneumonia, meningitis, and deep-seated infections such as osteomyelitis, bacteremia, and endocarditis. S. aureus expresses several virulence factors, such as toxins and adhesins, that facilitate its pathogenesis and has developed resistance to many commonly used antibiotics.1-3 Approximately 95% of S. aureus isolates produce a narrow-spectrum β-lactamase, which confers resistance to penicillin. About half of S. aureus isolates are resistant to methicillin (MRSA) and most other β-lactams via the overproduction of penicillin-binding proteins (PBPs), specifically PBP2a, as a result of the presence of the mecA gene. 4 More recently, increasing incidences of vancomycin-intermediate S. aureus (VISA), heteroresistant VISA (hVISA), and isolated cases of vancomycin-resistant S. aureus (VRSA) have been observed. 5 Because there are limited therapeutic options for serious MRSA infections, these resistant strains pose a significant threat.
Historically, MRSA infections were seen primarily in hospitalized patients or those with health care exposure. Between 1992 and 2003, the prevalence of MRSA isolates in intensive care units doubled. 6 However, the overall incidence of MRSA decreased 31% from 2005 to 2011, with the largest decrease in hospitalized patients at 54%. 7 Although the overall incidence of MRSA is decreasing, the 2013 Threat Report from the Centers for Disease Control and Prevention classifies MRSA as a serious-level threat, meaning that it remains a serious concern and requires prompt and sustained action to ensure that the problem does not escalate. 8 They estimated that 80, 461 invasive MRSA infections and 11, 285 related deaths occurred in 2011, underscoring the fact that while the overall incidence of MRSA is on the decline, these infections require prompt medical attention, especially bacteremia and endocarditis, which are among some of the most serious MRSA infections. 8
Blood stream infections are a leading cause of death in the United States, and S. aureus is responsible for approximately 20% of nosocomial bacteremia cases, half of which are MRSA. 9 MRSA bacteremia (MRSAB) is associated with high morbidity and mortality rates, increased hospital length of stay and health care costs.3,7,9-11 In comparison to methicillin-sensitive S. aureus (MSSA), MRSA is associated with longer median time to clearance of bacteremia of 8 to 9 days versus 3 days.11-13 Persistent bacteremia is associated with increased incidence of a metastatic site of infection, and ultimately, poorer outcomes. 10 MRSAB mortality rates range anywhere from 20% to 60%. Specifically looking at those patients with MRSA endocarditis, a common sequelae of bacteremia, mortality ranges from 30% to 37%.10-16 The 2011 MRSA treatment guidelines from the Infectious Diseases Society of America (IDSA) categorizes MRSAB as complicated or uncomplicated. 16 The distinction is important because it determines duration of antibiotic therapy. Uncomplicated bacteremia requires the exclusion of endocarditis, absence of implanted prosthetics, clearance of bacteremia within 2 to 4 days after initiation of antibiotics, defervescence within 72 hours of therapy, and absence of evidence of a metastatic infection. The presence of any of the above factors indicates complicated bacteremia. 16
The 2011 IDSA MRSA guidelines recommend vancomycin or daptomycin as first-line options for treatment of complicated and uncomplicated MRSAB, based on efficacy demonstrated in clinical trials.13,16 Recommended treatment duration for uncomplicated MRSAB is 14 days from the first negative blood culture, but because of difficulties in treating deep-seated infections, complicated MRSAB generally requires 4 to 6 weeks of treatment. 16 Despite appropriate antimicrobial therapy, clinical and microbiological failures are common in patients with MRSA endocarditis and bacteremia. Persistent bacteremia is often an issue of source control; however, there are instances where source control may not be achievable, and treatment failures have been observed even in those patients on optimal antibiotic therapy. 16
Vancomycin, although often considered the gold standard for treatment of MRSAB and endocarditis, has been associated with treatment failures and poor outcomes. Factors linked with vancomycin treatment failures include the drug’s slow bactericidal activity, minimum inhibitory concentrations (MICs) ≥2 µg/mL, emergence of hVISA, and difficulty in attaining optimal vancomycin serum concentrations.9-11,16,17 As with vancomycin, treatment failures have also been observed with daptomycin. In clinical trials, the emergence of reduced susceptibilities to daptomycin while on therapy has been associated with treatment failure. 13 In addition, there is a correlation between daptomycin nonsusceptible strains and increased vancomycin MICs.18-20 Given daptomycin’s concentration-dependent pharmacodynamics, higher doses may be needed to overcome the burden of infection.9-11,16-18
The definition of treatment failure and appropriate indications for change in therapy remain unclear. The average time to clearance of blood cultures in MRSAB is 7 to 9 days, and as previously stated, persistent bacteremia is associated with worse clinical outcomes, increased health care costs, and potential for antimicrobial resistance.9-11,13,16,21 Because no agents have been proven to be superior to vancomycin or daptomycin, a dilemma presents itself when a patient, on appropriate anti-MRSA therapy, remains bacteremic. The IDSA MRSA guidelines recommend that on or around day 7 of continued bacteremia, patients should be assessed to determine if a change in therapy is appropriate; taking into account the overall clinical response, vancomycin trough serum concentrations, susceptibility testing results, and the ability to achieve source control. 16 If a change in therapy is deemed appropriate, no clear alternative or salvage regimen is recommended in the guidelines. Guideline-suggested alternatives for salvage therapy are listed in Table 1. 16 Data for these regimens are largely based on case reports or small subgroups from clinical trials.16,19,22,23 Because there is no clear-cut answer, the question remains: What alternate agent should be utilized in persistent MRSAB and antibiotic treatment failure?
Alternate Agents for Persistent Methicillin-Resistant Staphylococcus aureus Bacteremia With Reduced Susceptibilities to Vancomycin and Daptomycin. a
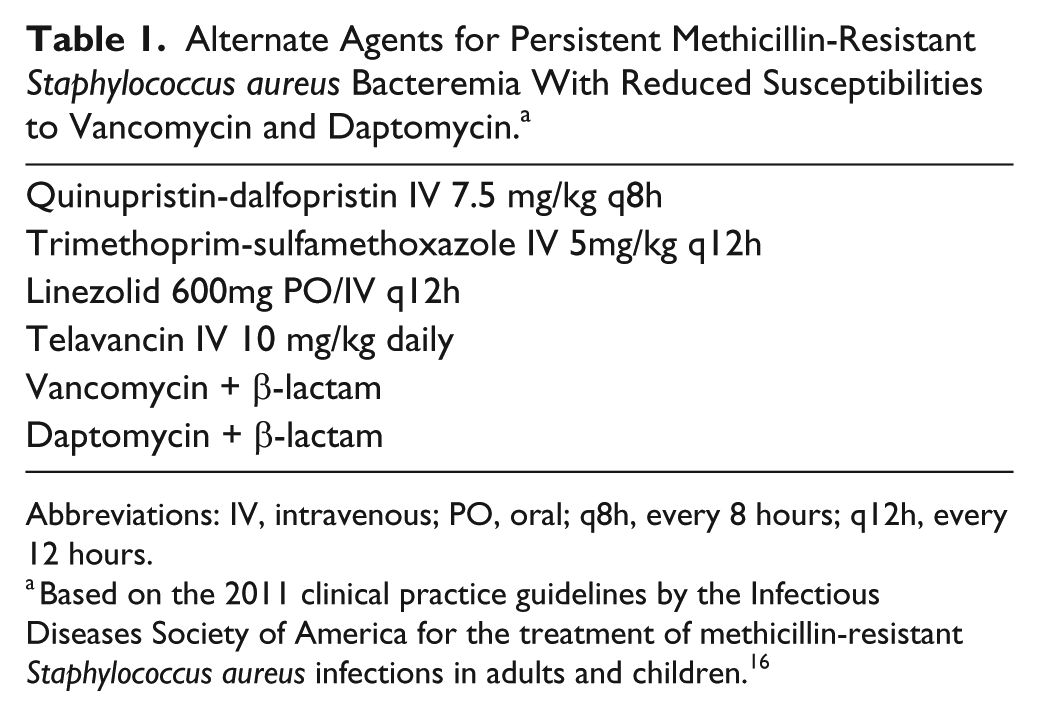
Abbreviations: IV, intravenous; PO, oral; q8h, every 8 hours; q12h, every 12 hours.
Based on the 2011 clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. 16
Since the publication of these guidelines, several new Gram-positive antibiotics have been approved, including ceftaroline, dalbavancin, oritavancin, and tedizolid. All have MRSA activity, however, with the exception of ceftaroline, there is little to no data available for their use in bacteremia. This article will describe the use of ceftaroline as a potential option for salvage monotherapy in MRSAB and endocarditis.
Data Sources
A PubMed search was conducted to identify articles relevant to the use of ceftaroline as salvage monotherapy for persistent MRSAB. The search was limited to articles published between January 1980 and June 2016. The search used a combination of the following terms: methicillin-resistant Staphylococcus aureus, MRSA, bacteremia, ceftaroline, refractory, and persistent. Supplemental references were generated through a review of identified literature citations. Available English-language full-text articles pertaining to the use of ceftaroline for persistent MRSAB were included. There are no published randomized controlled trials to date. Four of the largest case series were chosen for inclusion in this review. The literature was summarized pertaining to the clinical setting in the context of this search. Results of the literature search were independently reviewed by the authors for relevance.
Literature Review
Ceftaroline
Ceftaroline is a bactericidal extended-spectrum cephalosporin approved in 2010 and the first β-lactam antibiotic available with MRSA activity. As with other β-lactams, ceftaroline binds to essential PBPs, thereby preventing cell-wall synthesis. However, unlike its predecessors, it possesses the ability to bind to PBP2a, conferring MRSA activity. Currently, ceftaroline is FDA approved for the treatment of community-acquired bacterial pneumonia (CABP) and ABSSSI dosed 600 mg every 12 hours.24-27 In September 2015, ceftaroline gained FDA approval for the treatment of concurrent S. aureus bacteremia (SAB) in patients with ABSSSI. 26 Reported adverse effects are generally mild and include neutropenia, diarrhea, nausea, rash, increase in liver function tests, hypokalemia and Clostridium difficile infection (CDI).26-28 The half-life of ceftaroline is approximately 2.7 hours with normal renal function, however dose adjustment is required in patients with decreased creatinine clearance, as this is the primary mode of elimination. 26 Based on the pharmacokinetics, ceftaroline was dosed twice daily in the ABSSSI and pneumonia clinical trials. Although ceftaroline has been utilized clinically for only a few years, resistant S. aureus strains have been reported. The Clinical Laboratory and Standards Institute (CLSI) has determined that MRSA isolates with a MIC ≤1 mg/L are susceptible to ceftaroline (Table 2). 26 It is worth noting the MIC50/90, or the concentrations at which 50% or 90% of isolates are inhibited, for MRSA are higher than those for MSSA (0.5/1 vs 0.25/0.25 mg/L, respectively). 29 Based on data provided from the Assessing Worldwide Antimicrobial Resistance and Evaluation (AWARE) surveillance program, between 2008 and 2015, 97.6% of MRSA isolates in the United States tested susceptible to ceftaroline. 29 However, it should be noted that susceptibility rates may not be the same worldwide. AWARE data from 7 countries in the Asia-Pacific region and Australia state that 78.8% and 83.1%, respectively, of MRSA isolates collected in 2012 tested susceptible to ceftaroline.30,31 Although resistance rates may appear low in the United States, it is important to recognize and monitor regional differences in resistance trends.
MIC Breakpoints.
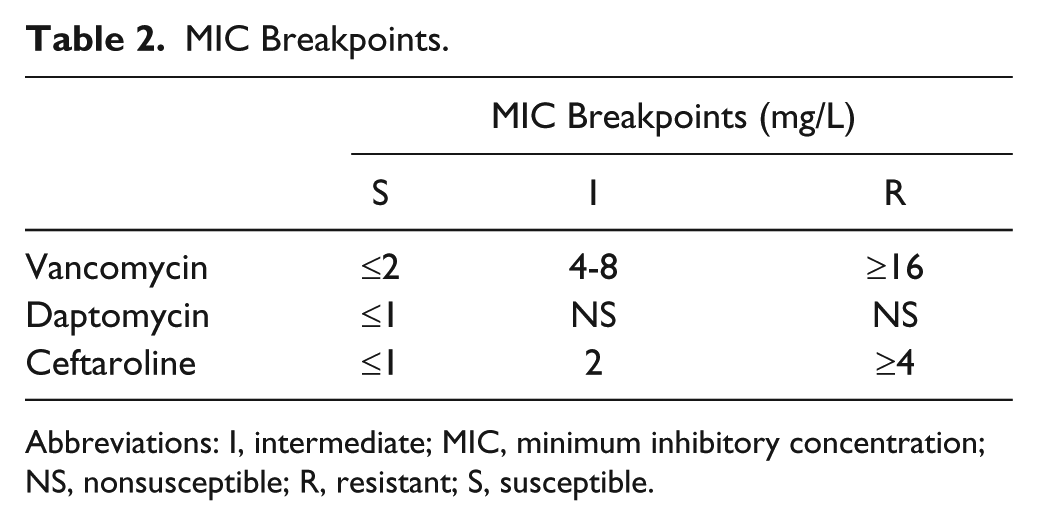
Abbreviations: I, intermediate; MIC, minimum inhibitory concentration; NS, nonsusceptible; R, resistant; S, susceptible.
As with other β-lactams, ceftaroline exhibits time-dependent killing and correlates with the percentage of time during the dosing interval that the free drug concentration remains above the MIC (f%T>MIC). A Monte Carlo pharmacokinetic-pharmacodynamics (PK-PD) attainment analysis evaluated ceftaroline dosed at 600 mg every 12 hours in normal renal function to predict the probability that ceftaroline at the above dose would attain the appropriate f%T>MIC (defined as 51% of the dosing interval). 32 In MRSA isolates with an MIC of 1 mg/L, the CLSI breakpoint, ceftaroline attained the PK-PD target 97% of the time at 600 mg every 12 hours. Similar results were seen at the approved renal dose adjustments, thereby validating the FDA-approved dose of ceftaroline for CABP and ABSSSI. 32 Nonetheless, questions remain regarding optimal dosing of ceftaroline if used for more serious infections such as MRSAB and endocarditis. An in vitro hollow-fiber PK-PD analysis evaluated the activity of ceftaroline 600 mg every 12 versus every 8 hours. 33 For MRSA strains with an MIC of 0.5 mg/L, ceftaroline dosed every 8 hours produced a f%T>MIC of 100%, whereas dosing every 12 hours achieved a f%T>MIC for 83% of the dosing interval. At the current CLSI breakpoint of 1 mg/L, ceftaroline dosed every 8 hours produced f%T>MIC of 94% versus 62.5% when dosed every 12 hours. Although the more-frequent dosing schedule attained free drug concentrations above the MIC for a greater part of the dosing interval, it was noted that there was no difference in killing activity between the 2 regimens. Because this is an in vitro study, it is unknown if there will be greater efficacy seen with higher doses of ceftaroline used in vivo, but it suggests that higher doses may be necessary to attain appropriate PK-PD targets in deep-seated infections; this will be discussed later when reviewing clinical studies of ceftaroline for MRSAB.
Ceftaroline is not FDA indicated for treatment of bacteremia or endocarditis caused by S. aureus, with the exception of concomitant bacteremia and ABSSSIs. 26 However, other antistaphylococcal β-lactams have demonstrated superior outcomes in the treatment of MSSA bacteremia compared with vancomycin, suggesting that ceftaroline may be a viable option in this setting.34-37 Within the FDA registry trials for ceftaroline for ABSSSI, 7 patients also had concomitant MRSAB, and 6/7 attained clinical cure (86%). 25 Based on these data, as well as ceftaroline’s favorable PK-PD profile, excellent bactericidal MRSA activity, low baseline resistance, and ease of dosing, some clinicians have utilized it for salvage therapy in MRSAB and endocarditis. In addition, a phenomenon described as the “seesaw effect” has been observed in cases of decreased glycopeptide or lipopeptide susceptibility, where susceptibility to β-lactam antibiotics is enhanced.38,39 This allows for older β-lactam antibiotics to be used in combination with glycopeptide or lipopeptide antibiotics, such as vancomycin or daptomycin. In vitro studies have demonstrated a marked “seesaw effect,” where ceftaroline susceptibilities were increased in the setting of increased vancomycin, daptomycin, and teicoplanin MICs. 38 With the addition of ceftaroline to the armamentarium of antibiotics active against MRSA, there may be a place in therapy for ceftaroline in patients with preexposure to vancomycin or daptomycin.
Summary of the Literature
At the time of this publication, no randomized controlled trials have evaluated ceftaroline for the treatment of MRSAB. Results from a completed cohort study evaluating the safety and efficacy of ceftaroline in individuals with S. aureus bacteremia or persistent MRSAB have yet to be published. 40 Currently available data are limited to case reports and case series of its use in salvage treatment of MRSAB.41-47 Four of the largest case series will be discussed (Table 3).44-47 The first 2 case series have small numbers, but were the first to document use of ceftaroline for MRSAB. The final 2 case series contain the most comprehensive evidence available supporting ceftaroline for the treatment of MRSAB.
Ceftaroline Use in MRSAB.
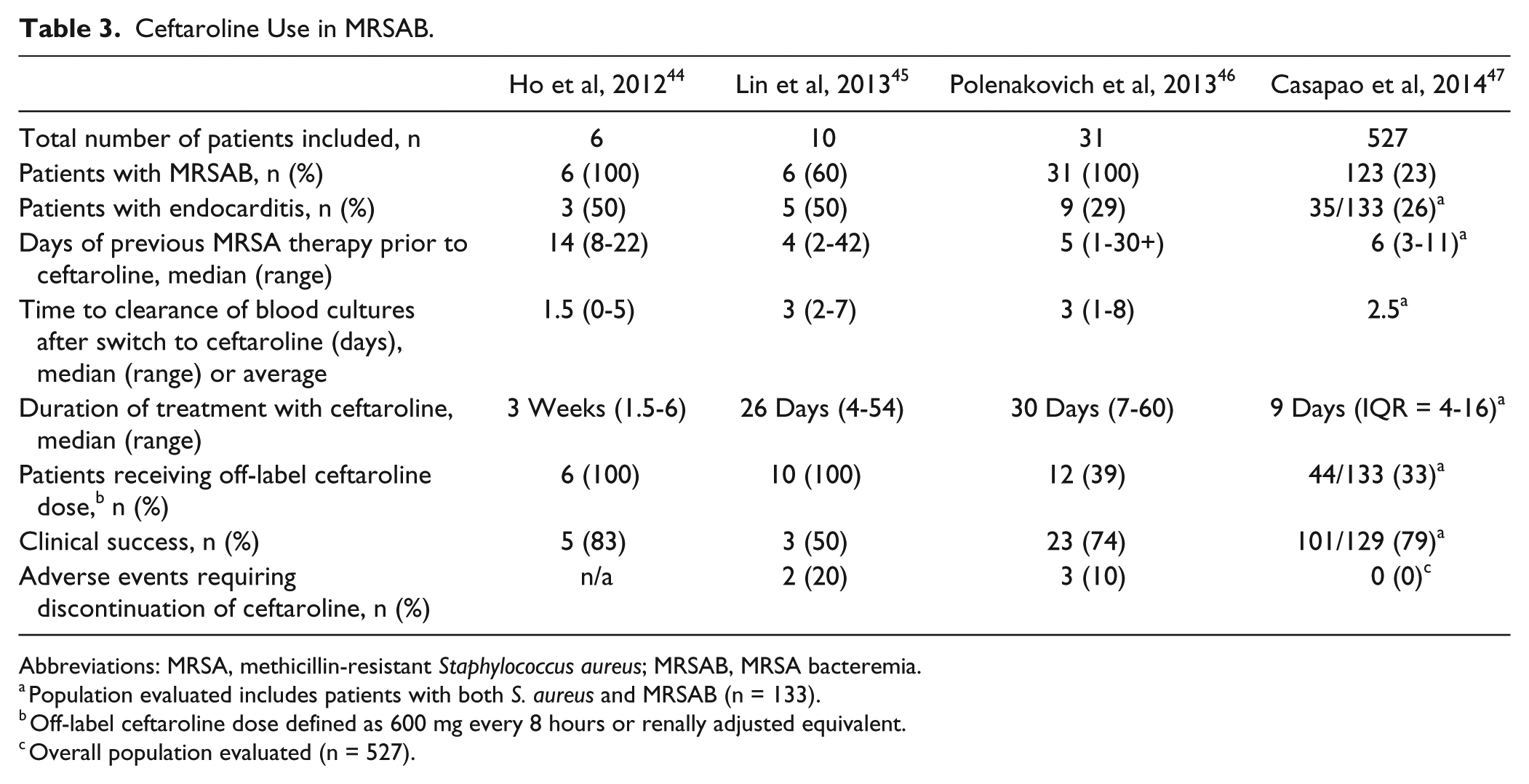
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MRSAB, MRSA bacteremia.
Population evaluated includes patients with both S. aureus and MRSAB (n = 133).
Off-label ceftaroline dose defined as 600 mg every 8 hours or renally adjusted equivalent.
Overall population evaluated (n = 527).
The first report of ceftaroline for MRSAB was a case series of 6 patients with ceftaroline as salvage monotherapy for persistent MRSAB. 44 These complicated patients all had concomitant infections such as uveitis, osteomyelitis, and septic thrombophlebitis, and 3 were also diagnosed with endocarditis. All had received previous treatment with vancomycin, with therapeutic trough serum concentrations, and one also received daptomycin after 13 days of vancomycin. Therapy was initiated with ceftaroline 600 mg every 8 hours after a median of 14 days (range = 8-22 days) of MRSA-active therapy. After switching to ceftaroline, median time to blood culture clearance was 1.5 days (range = 0-5 days). Two patients cleared their bacteremia on day 1 of ceftaroline therapy. Patients were continued on ceftaroline for a median of 3 weeks (range = 1.5-6 weeks). One patient received 6 weeks of ceftaroline to complete therapy; 4 others were switched after 2 to 3 weeks of ceftaroline to vancomycin, linezolid, or daptomycin to complete therapy for ease of administration or consolidation therapy. Source control, mitral valve replacement, was performed in 1 patient with endocarditis after 13 days of ceftaroline. Cultures of the valve were negative for MRSA. Of the 6 patients treated, 5 had resolution of MRSAB. One death occurred in a patient with acute respiratory failure and gastrointestinal bleeding. The investigators did not attribute cause of death to the infection or ceftaroline. No adverse events were reported in this analysis, despite the use of higher doses of ceftaroline and longer treatment durations; however, follow up data available were limited. This initial case series provided some evidence that ceftaroline may be useful in deep-seated MRSAB.
The second case series included 10 patients treated with ceftaroline for MRSA endocarditis and deep-seated infections. 45 Six patients had positive blood cultures, 5 of whom were diagnosed with endocarditis. Endocarditis was diagnosed clinically and was presumed if the patients had prolonged bacteremia (>48 hours) with no other source and were suspected to have an intravascular source of infection. Other infections included pyomyositis, osteomyelitis, septic arthritis, and pneumonia. Patients were switched to ceftaroline therapy if they failed to clinically respond to vancomycin, relapsed after treatment, or experienced therapy-limiting adverse events. The median duration of prior MRSA therapy was 4 days (range = 2-42 days). The authors did not comment as to whether those patients on vancomycin prior to the switch attained therapeutic troughs. All patients were treated with ceftaroline 600 mg every 8 hours or renal dose equivalent. Of the 6 patients with bacteremia, 5 patients cleared their blood cultures in a median of 3 days after initiation of ceftaroline (range = 2-7 days). Patients received ceftaroline for a median of 26 days (range = 5-54 days). Overall, 6 of 10 patients achieved clinical cure, 3 of whom were in the MRSAB/endocarditis subpopulation. Clinical cure was defined as resolution of all signs and symptoms of infection or improvement such that no further antimicrobial therapy was necessary. Three patients were placed on comfort care and died in the hospital. Four patients experienced adverse events that included CDI (n = 3), eosinophilia (n = 3), and rash (n = 2). Ceftaroline was discontinued in 2 patients who experienced rash. Again, this series showed success in using ceftaroline for deep-seated infections caused by MRSA, but also highlighted the need for close monitoring of adverse events.
The third study reviewed 31 patients with MRSAB who received at least 7 days of ceftaroline. 46 Of these, 9 patients also had endocarditis (29%), and the most common sources of bacteremia were central venous catheters or unknown. The median duration of prior MRSA therapy was 5 days, but ranged from 1 to more than 30 days. Of the 31 patients, 26 received vancomycin, 7 received daptomycin, 3 received linezolid, and 2 received trimethoprim-sulfamethoxazole. Six patients received 2 or 3 alternate antibiotic regimens before switching to ceftaroline. Rationale for switching to ceftaroline included vancomycin MIC ≥2 mg/L, persistent bacteremia, or poor clinical response to current MRSA therapy per the treating physician. No comment was made as to the duration of bacteremia prior to switching to ceftaroline; however, 11 patients were noted to have persistent MRSAB listed as a reason for ceftaroline use. Persistent MRSAB was defined as bacteremia persisting after 7 days of vancomycin or daptomycin treatment. The median total daily dose of ceftaroline was 1200 mg; however, approximately 40% of patients (12/31) received a daily dose of 1800 mg (equivalent to 600 mg every 8 hours). The median duration of ceftaroline therapy was 30 days (range = 7-60 days). After switching to ceftaroline, 45% of patients cleared their blood cultures within 72 hours; 74% (23/31) of patients met criteria for clinical success, defined as the resolution of signs and symptoms of infection at the end of ceftaroline therapy per the treating physician. Three patients experienced recurrent bacteremia; however, all 3 also retained prosthetic devices. Patients were followed for a median of 30 days to evaluate for adverse events. Of the 31 patients, 3 (10%) required cessation of treatment as a result of adverse events, including antibiotic-associated diarrhea, rash, and 1 case of eosinophilic pneumonia. There were 2 additional cases of peripheral eosinophilia that resolved without cessation of ceftaroline.
The largest series was a retrospective observational multicenter study that analyzed the clinical and microbiological outcomes of 527 patients who were treated with ceftaroline for ≥72 hours. 47 Patients were excluded from the analysis if ceftaroline was used for prophylactic therapy or an infection caused by an organism known to be resistant to ceftaroline (eg, Pseudomonas aeruginosa, ESBL [extended-spectrum β-lactamase]-producing Enterobacteriaceae) alone without MRSA infection. Although this review evaluated patients with a variety of infections, a large subpopulation of MRSAB was present. Overall, 62% of patients had positive cultures for S. aureus, of which 89% were MRSA. Of the total population, 148 patients had a diagnosis of bacteremia, and 133, or 25%, had SAB. Also, 80% (422/527) of all patients were previously treated with MRSA active therapy. Vancomycin, daptomycin, and linezolid were the 3 most common antimicrobials prescribed prior to initiation of ceftaroline (70% [295/422], 14% [60/422], 6% [24/422], respectively). The most common rationales for ceftaroline use included disease progression on prior therapy, a simplified regimen for multiple indications, and anticipated risk of toxicity on current therapy.
Examining specifically the bacteremia subpopulation, 93% (123/133) of the patients with SAB had MRSAB, and 97% (143/148) received MRSA treatment prior to ceftaroline for a median of 6 days (range = 3-11 days). Specific MRSA-targeted treatment prior to the switch was not defined in the bacteremia subpopulation. It was found that 26% of patients with SAB also had concomitant endocarditis (35/133). In addition to ceftaroline, 31% of patients (41/133) in the SAB subpopulation were administered another concomitant antimicrobial. These agents were not defined; however, it was stated that metronidazole was the most common antimicrobial administered in combination with ceftaroline. It is unknown whether other anti-MRSA antibiotics were also administered, which may or may not have affected the results. Approximately one-third (45/133) of patients received off-label, high-dose ceftaroline. The authors stated that the time to clearance of bacteremia after switching to ceftaroline was 2.5 days, although it was not noted how many patients had positive blood cultures at the time ceftaroline was initiated. Of the 130 evaluable patients with SAB, 117 (90%) achieved microbiological success (eradication of the infecting organism of the clinically evaluable patients). Clinical success, resolution of all signs and symptoms of infection with no need for escalation of antimicrobials while on ceftaroline, was achieved in 78% of SAB patients (101/129). The median duration of ceftaroline therapy during hospitalization was 9 days (range = 4-16 days). Among the patients, 71% were prescribed antibiotics as an outpatient, and approximately half were given ceftaroline as part of their outpatient regimen.
This study also commented on the outcomes by dosing strategy. Within the bacteremic subpopulation, there was no difference in clinical cure (79.4% vs 78.5%) using standard dosing or off-label dosing. Overall, adverse events were uncommon, with only 8% of patients experiencing any adverse event, and no patient requiring cessation of therapy. Higher rates of adverse events were seen in the bacteremic subgroup (19/133, 13%) and those who were prescribed off-label doses of ceftaroline (13/76, 17%). The most common adverse reactions reported included renal failure, diarrhea, vomiting, nausea, rash, hypokalemia, and CDI. No information was included regarding long-term patient follow-up. Because many of these patients likely received prolonged courses of antibiotics, the lack of information about adverse events leaves a large hole in the data.
Four case series provide evidence of ceftaroline monotherapy for salvage treatment of MRSAB and endocarditis. The most consistent rationale inciting a change in therapy to ceftaroline was persistent bacteremia on appropriate anti-MRSA therapy. Most showed favorable outcomes with quick clearance of bacteremia, although given the median duration of MRSAB in clinical trials, patients may have cleared their bacteremia had they continued on their previous regimen. Still, many of these patients were bacteremic significantly longer than 7 to 9 days, and ceftaroline demonstrated rapid clearance of blood cultures even in these patients. Some patients received higher, off-label dosing of ceftaroline in an effort to achieve optimal PK-PD targets in serious infections and with organisms with higher MICs. Although reported adverse events were uncommon, the follow-up data were wholly inadequate to assess this, and so, the true incidence of adverse events associated with higher doses of ceftaroline for a prolonged duration is unknown. Some concerning reports describe hematological toxicities that limit treatment duration with ceftaroline. Neutropenia and anemia have both been reported as causes for treatment discontinuation, possibly as a result of dose accumulation as most discontinuations occurred around day 22 of therapy.28,48-50 It is unknown whether other adverse effects caused by dose accumulation may appear with prolonged used of ceftaroline, such as neurotoxicity seen with cefepime. 51 It is also unclear whether ceftaroline will retain durable activity against MRSA with more frequent use because recent reports from Australia and Asia suggest higher rates of resistance than previously reported.30,31 To date, follow-up data regarding patient outcomes from these case series have not yet been published. Results from a completed cohort study evaluating the safety and efficacy of ceftaroline in those with SAB or persistent MRSAB are expected and may provide more evidence for the use of ceftaroline for these indications. 40
Combination therapy of vancomycin or daptomycin with β-lactam antibiotics is also an evolving area of interest. There have been many in vitro studies demonstrating synergy, even if the β-lactam itself is not active against MRSA.20,39,52 Furthermore, there have been in vitro analyses and case series reporting on combination therapy of vancomycin, daptomycin, or trimethoprim-sulfamethoxazole with ceftaroline for the treatment of persistent MRSAB.53-55 These results appear promising, with rapid clearance of bacteremia, but the potential for drug-drug interactions as well as increased health care costs may outweigh the benefit of combination therapy. Further studies are warranted to evaluate the utility in this complex patient population.
Conclusion
Available evidence suggests a possible role for ceftaroline in the treatment of MRSA, but 2 major questions remain: What is ceftaroline’s place in the treatment of MRSAB and endocarditis, and if used, at what dose? Based on the available data, ceftaroline may be considered for those patients failing first-line therapy with vancomycin or daptomycin, in cases of nonsusceptibility to first-line agents, or in patients with allergies or intolerances to the first-line agents. PK-PD studies have shown higher target attainment using more frequent dosing—600 mg every 8 hours versus every 12 hours in vitro. Higher doses appear to be effective, and given the severity of illness, a more aggressive dosing strategy might be appropriate in some patients. However, this may come at the price of an increased incidence of adverse effects, and it will be imperative to monitor for these, particularly with prolonged treatment courses. Although there are some reports using combination therapy of ceftaroline with another anti-MRSA agent, the benefit over monotherapy has not been established, and further studies are warranted.
Footnotes
Authors’ Note
These data have not been published elsewhere and are not under consideration for any other journal.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.