
Abstract
Background:
Drug pharmacokinetics (PK) are altered in neurocritically ill patients, and optimal levetiracetam dosing for seizure prophylaxis is unknown.
Objective:
This study evaluates levetiracetam PK in critically ill patients with severe traumatic brain injury (sTBI) receiving intravenous levetiracetam 1000 mg every 8 (LEV8) to 12 (LEV12) hours for seizure prophylaxis.
Methods:
This prospective, open-label study was conducted at a level 1 trauma, academic, quaternary care center. Patients with sTBI receiving seizure prophylaxis with LEV8 or LEV12 were eligible for enrollment. Five sequential, steady-state, postdose serum levetiracetam concentrations were obtained. Non-compartmental analysis (NCA) and compartmental approaches were employed for estimating pharmacokinetic parameters and projecting steady-state trough concentrations. Pharmacokinetic parameters were compared between LEV8 and LEV12 patients. Monte Carlo simulations (MCS) were performed to determine probability of target trough attainment (PTA) of 6 to 20 mg/L. A secondary analysis evaluated PTA for weight-tiered levetiracetam dosing.
Results:
Ten male patients (5 LEV8; 5 LEV12) were included. The NCA-based systemic clearance and elimination half-life were 5.3 ± 1.2 L/h and 4.8 ± 0.64 hours. A one-compartment model provided a higher steady-state trough concentration for the LEV8 group compared with the LEV12 group (13.7 ± 4.3 mg/L vs 6.3 ± 1.7 mg/L; P = 0.008). Monte Carlo simulations predicted regimens of 500 mg every 6 hours, 1000 mg every 8 hours, and 2000 mg every 12 hours achieved therapeutic target attainment. Weight-tiered dosing regimens achieved therapeutic target attainment using a 75 kg breakpoint.
Conclusion and Relevance:
Neurocritically ill patients exhibit rapid levetiracetam clearance resulting in a short elimination half-life. Findings of this study suggest regimens of levetiracetam 500 mg every 6 hours, 1000 mg every 8 hours, or 2000 mg every 12 hours may be required for optimal therapeutic target attainment. Patient weight of 75 kg may serve as a breakpoint for weight-guided dosing to optimize levetiracetam therapeutic target attainment for seizure prophylaxis.
Background
Levetiracetam is an antiseizure drug widely used for the prevention and treatment of seizures. While the specific mechanism is unknown, levetiracetam binds to synaptic vesicle protein 2A in the brain and inhibits presynaptic calcium channels, reducing neurotransmitter release and acting as a neuromodulator. Levetiracetam demonstrates linear pharmacokinetics (PK) with peak serum concentrations within 30 minutes of intravenous administration, and an elimination half-life of 6 to 8 hours in healthy populations. 1 Critically ill patients often demonstrate pharmacokinetic changes necessitating dose adjustments to pharmacotherapeutic regimens. Augmented renal clearance (ARC), defined as enhanced renal elimination of solutes, has been described in critically ill populations including patients with trauma, burns, and acute brain injury. Renally eliminated medications, including levetiracetam (60%-70% elimination via glomerular filtration), may require higher doses or more frequent administration to achieve the desired pharmacodynamic impact in these populations.2-4
Early posttraumatic seizures (PTS) have an incidence of 0.4% to 10.5% and are associated with increased morbidity and mortality. Prevention of PTS may reduce the risk of developing posttraumatic epilepsy, which accounts for 5% of all epilepsies. 5 The most recent guidelines for severe traumatic brain injury (sTBI) recommend phenytoin for prophylaxis of early PTS. 6 Despite this, levetiracetam is used for seizure prophylaxis given its favorable pharmacokinetic properties, infrequent adverse events, wide therapeutic index, and limited drug interaction profile.6-15 Phenytoin has a narrow therapeutic index, exposure-related toxicity, and is heavily affected by changing pharmacokinetic parameters making it a less desirable option in critically ill populations. 16 Levetiracetam dosing for PTS prophylaxis varies, but a dose of 1000 mg every 12 hours is generally used in patients with normal renal function. 9 A strong correlation between levetiracetam concentrations and clinical efficacy has yet to be established, but a trough concentration of 6 to 20 mg/L has been suggested for prophylaxis.17-19
Evidence to guide dosing for target levetiracetam trough attainment in critically ill patients is limited. A previous study evaluated 12 adult neurocritical care patients receiving seizure prophylaxis with intravenous levetiracetam 500 mg every 12 hours. Pharmacokinetic modeling predictions found levetiracetam 1000 mg every 8 hours had a 57.1% probability of achieving goal trough concentrations of 6 to 20 mg/L, but this predicted dosing regimen has not been directly measured. 18 The primary purpose of this study is to evaluate levetiracetam PK in critically ill patients with sTBI receiving intravenous levetiracetam 1000 mg every 8 to 12 hours for PTS prophylaxis.
Methods
This prospective, open-label, single-center, pilot PK/PD study was conducted at an American College of Surgeons–verified level 1 trauma center. Institutional review board (IRB) approval was obtained (University of Cincinnati IRB 2020-0744) and informed consent was obtained from each patient’s legally authorized representative. Patients aged 18 to 80 years admitted to the neurosurgical intensive care unit (NSICU) or surgical intensive care unit (SICU) and diagnosed with sTBI were screened for inclusion. Severe TBI was defined as a postresuscitation Glasgow Coma Score (GCS) ≤8 with or without head computed tomography scan abnormalities. Patients receiving intravenous levetiracetam 1000 mg every 8 or 12 hours for PTS prophylaxis were eligible for inclusion. Patients were excluded for known history of seizure disorder, prescribed antiseizure drugs prior to admission, taking medications with known effect on levetiracetam PK (carbamazepine, phenytoin, oxcarbazepine, mefloquine, methotrexate, or orlistat), weight <50 kg, anticipated survival <72 hours from injury determined by the primary neurosurgeon’s clinical discretion, acute kidney injury or creatinine clearance (CrCl) <50 mL/min at the time of enrollment, incarceration, and pregnancy. Acute kidney injury was defined as an increase in serum creatinine (Scr) ≥ 0.3 mg/dL within 48 hours or increase in Scr to ≥1.5 time baseline or urine volume <0.5 mL/kg/h for 6 hours. 20
Prior to enrollment, intravenous levetiracetam was initiated in accordance with current institutional practice and was not influenced by study eligibility. Patients with sTBI qualifying for advanced neuromonitoring (Appendix 1) could receive more aggressive dosing (ie, levetiracetam 1000 mg every 8 hours) while all other sTBI patients receive levetiracetam 1000 mg every 12 hours. Levetiracetam dosing regimens were initiated and adjusted at the discretion of the primary treatment team. Patients were grouped based on primary dosing regimen: levetiracetam 1000 mg every 8 hours (LEV8) or 1000 mg every 12 hours (LEV12). Target enrollment was a minimum of 10 patients up to 20 patients equally divided between groups (10 LEV8, 10 LEV12).
Data Collection
Baseline characteristics were collected as follows: intensive care unit (ICU) location, sex, race, weight, age, admission CrCl, collection day CrCl, collection day Augmented Renal Clearance in Trauma Intensive Care (ARCTIC) score, mechanism of injury, baseline GCS, highest GCS at 24-hour postresuscitation, collection day GCS, presence of multimodal monitoring (MMM), first levetiracetam dose administered, and neurosurgical intervention during the study period. Clinical and/or electrographic seizures from admission to discontinuation of levetiracetam seizure prophylaxis were collected. Collection day was defined as the day of assay collection. Baseline GCS was defined as first documented GCS and 24-hour GCS was defined as postresuscitation GCS at 24 hours after hospital arrival. Creatinine clearance was calculated using the Cockcroft-Gault method. 21 The predicted presence of ARC was defined as an ARCTIC score ≥6 and CrCl ≥ 130 mL/min.2,3,22
One set of 5 post dose timed serum levetiracetam concentrations were collected by trained nursing staff after a minimum 6 consecutive doses to optimize probability of steady-state PK. Intravenous levetiracetam 1000 mg doses were administered over 30 minutes. Timing of sample collection was guided by previous evaluations and dependent on dosing regimen received. 18 Patients receiving LEV12 had samples collected at 0.5, 1, 4, 8, and 12 hours after infusion initiation. Patients receiving LEV8 had samples collected at 0.5, 1, 4, 6, and 8 hours after infusion initiation. Approximately 5 mL whole blood samples were collected in red top tubes from either peripheral or central venous catheters and delivered to the clinical laboratory for processing. Samples were allowed to clot for 20 to 30 minutes prior to sera harvesting into labeled tubes and transferred to Labcorp Specialty Labs (Dublin, Ohio) for analysis. Levetiracetam serum concentrations (Test: 716936, CPT: 80177) were assessed using a validated method of liquid chromatography tandem mass spectrometry (LQ/MS/MS) according to standard lab procedure. Results were marked as research and collected by the research team.
Pharmacokinetic Analysis
Pharmacokinetic analyses were conducted on an intention-to-treat basis using both non-compartmental analysis (NCA) and compartmental modeling with Phoenix WinNonlin software (version 8.2; Certara). Non-compartmental analysis was used for primary pharmacokinetic analysis that employed the trapezoidal method for determining the total (zero to infinity) area under the concentration-time curve (AUC) and regression analysis of data in the terminal part of the pharmacokinetic profile for estimating the terminal rate constant (λz). Systemic clearance (CL) was then determined as dose/AUC and the elimination half-life as (0.693/λz). The best fit compartment model was employed for projecting steady-state peak and trough levetiracetam concentrations. In addition, the compartmental modeling-based pharmacokinetic estimates were used for Monte Carlo simulations (MCS).
Pharmacokinetic parameters were compared between LEV8 and LEV12 patients. Descriptive statistical analyses were performed using SigmaPlot 15.0 (Systat, San Jose, California). Categorical and discrete variables were compared through chi-square and Fisher exact test, as appropriate. Continuous data were assessed for normality and described as mean ± standard deviation (SD) or median (interquartile range, IQR) as appropriate. Parametric data were compared using the Student t test and non-parametric data were compared using the Wilcoxon rank sum test. A P value of <0.05 was considered statistically significant.
Pharmacodynamic Analysis
Monte Carlo simulations were performed using Crystal Ball Fusion Edition release 11.1.2.0.00 (Oracle, Redwood Shores, California). Using mean and standard deviation of calculated pharmacokinetic parameters in the observed population, the volume of distribution and clearance of 10000 hypothetical patients were simulated with a lognormal distribution and uniformly distributed patient weights observed in the population. Steady-state, one-compartment serum concentration-time profiles were simulated for each of these patients for multiple intravenous levetiracetam dosing regimens, with an assumed unbound fraction of 100%. Each regimen was then assessed as a population probability of target attainment (PTA) for a therapeutic trough concentration defined as the number of patients with trough concentration ≥6 mg/L/10000 hypothetical patients. In addition, each regimen was assessed as a population PTA for supratherapeutic trough concentration >20 mg/L/10000 hypothetical patients. Therapeutic target attainment was defined as having both >90% PTA for trough concentrations ≥6 mg/L and <10% PTA for trough concentrations >20 mg/L and was assessed for each dosing regimen.
A secondary analysis explored PTA for weight-tiered levetiracetam dosing. Weight was simulated as a uniform distribution to allow for stratification of therapeutic and supratherapeutic PTA by 5 kg weight increments. The range of measured weights in the study population were utilized for analysis. Modeled dosing regimens were assessed for therapeutic target attainment at each weight increment.
Results
Study Population
Study enrollment was stopped after 10 patients (5 LEV8; 5 LEV12) were consented and enrolled. A total of 50 serum samples were collected and 49 serum samples were analyzed. One sample (study ID 1, sample 1) was inadvertently damaged during processing and was unusable. Study ID 6 received 2 doses of LEV12 before being changed to LEV8 and assays were collected after the fourth consecutive dose of the LEV8 regimen. All patients had at least 24 hours of continuous electroencephalography (cEEG) monitoring and all LEV8 patients received advanced neuromonitoring. Mean collection day creatinine clearance was 197.8 ± 56.8 mL/min. Nine patients (90%) demonstrated predicted ARC. No patients experienced clinical or electrographic seizure activity during the study period. Two patients (study ID 1 and 7) experienced clinical seizures prior to levetiracetam initiation. No patients received antiseizure drugs other than levetiracetam during resuscitation prior to study enrollment. Full study demographics are outlined in Table 1.
Baseline Demographics.
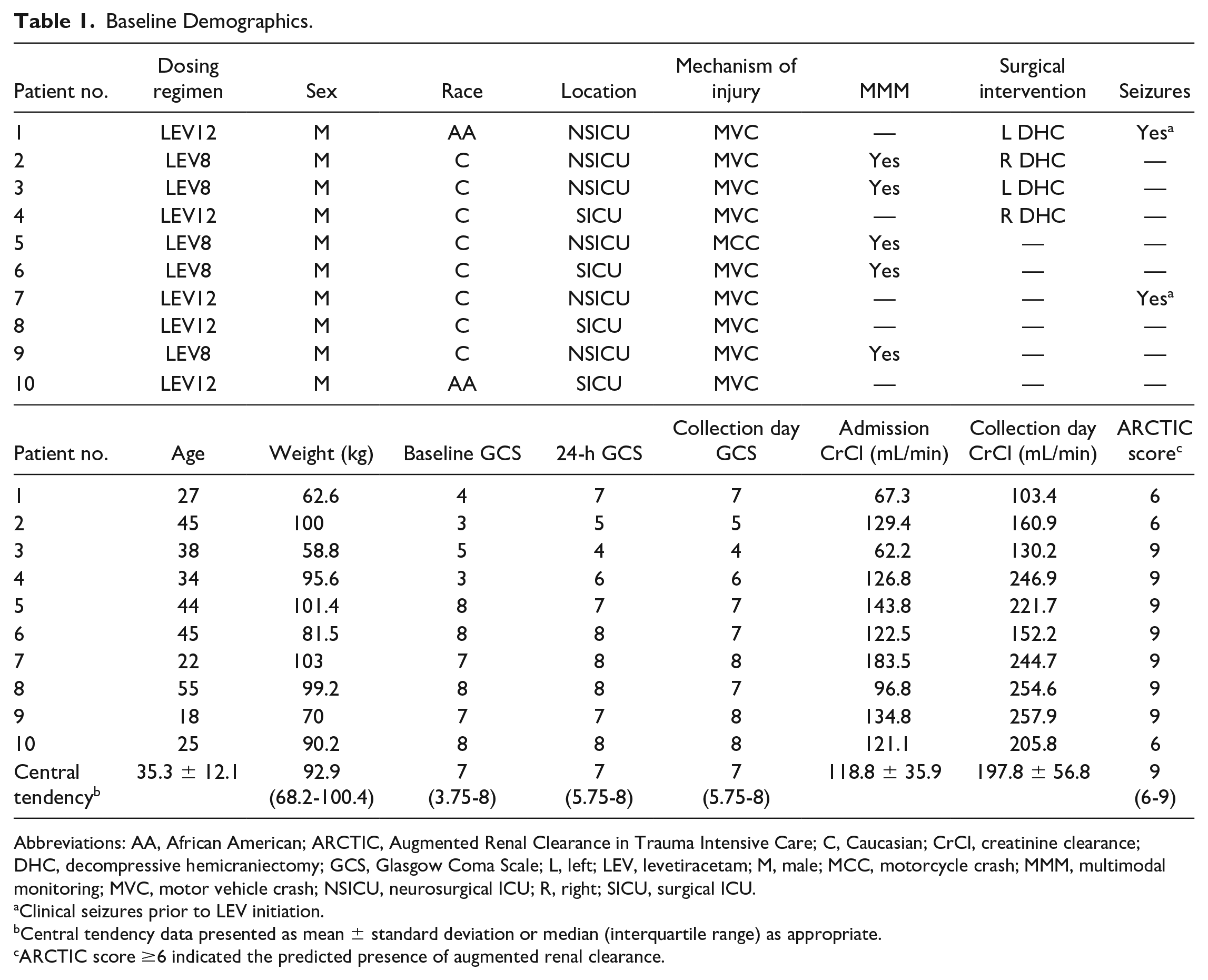
Abbreviations: AA, African American; ARCTIC, Augmented Renal Clearance in Trauma Intensive Care; C, Caucasian; CrCl, creatinine clearance; DHC, decompressive hemicraniectomy; GCS, Glasgow Coma Scale; L, left; LEV, levetiracetam; M, male; MCC, motorcycle crash; MMM, multimodal monitoring; MVC, motor vehicle crash; NSICU, neurosurgical ICU; R, right; SICU, surgical ICU.
Clinical seizures prior to LEV initiation.
Central tendency data presented as mean ± standard deviation or median (interquartile range) as appropriate.
ARCTIC score ≥6 indicated the predicted presence of augmented renal clearance.
Levetiracetam PK
Regression analysis indicated these data best fitted a one-compartment model, which was then employed for projecting steady-state peak and trough levetiracetam concentrations. This was based on observed goodness of fit, Akaike information criterion, and Schwarz criterion. The steady-state pharmacokinetic parameters are shown in Table 2. Predicted steady-state trough concentration (Cssmin) was 10 ± 4.96 mg/L. Systemic clearance and terminal elimination half-life (t1/2) were 5.3 ± 1.2 L/h and 4.8 ± 0.64 hours, respectively. Pharmacokinetic parameters were compared between LEV8 and LEV12 groups in Table 3. Predicted Cssmin was significantly higher with LEV8 compared with LEV12 (13.7 ± 4.3 mg/L vs 6.3 ± 1.7 mg/L, P = 0.008). No other significant differences were observed between groups.
LEV Pharmacokinetic Calculations.
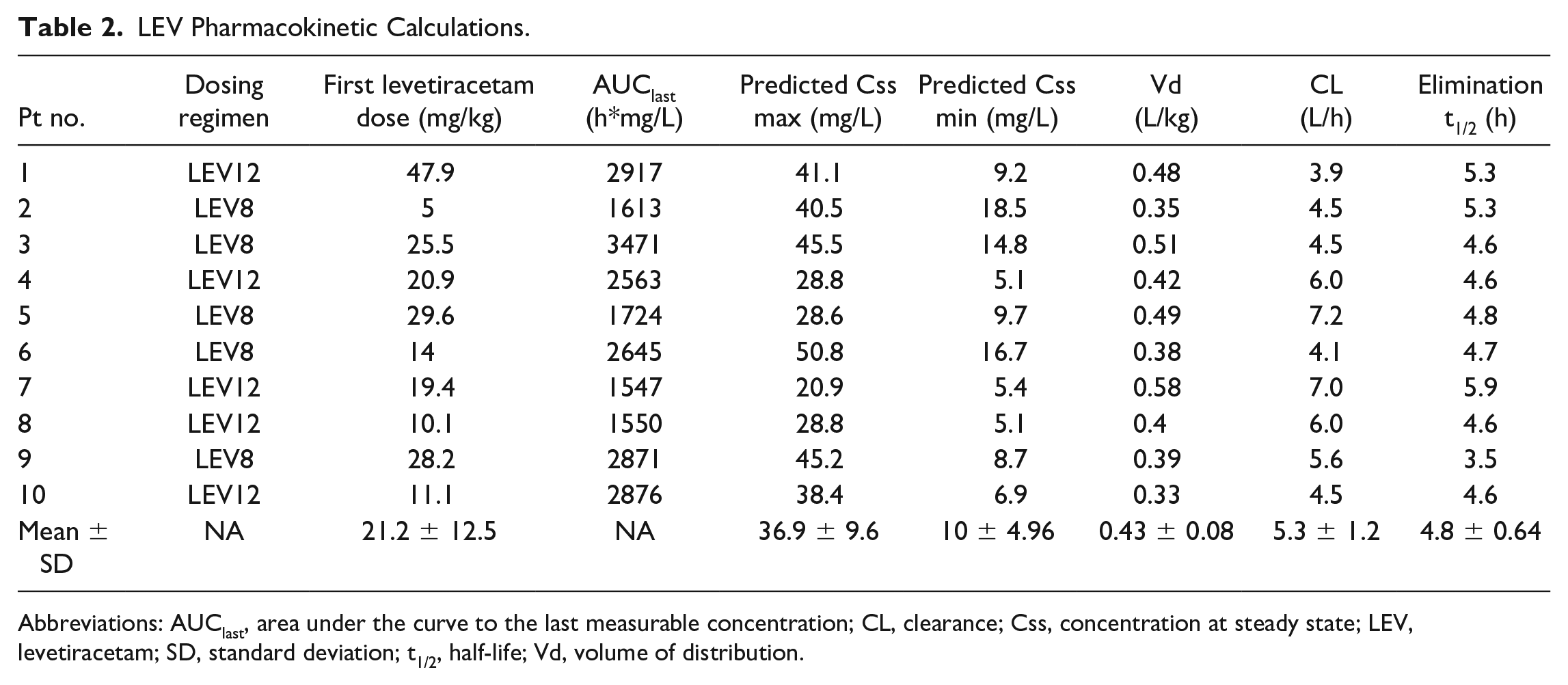
Abbreviations: AUClast, area under the curve to the last measurable concentration; CL, clearance; Css, concentration at steady state; LEV, levetiracetam; SD, standard deviation; t1/2, half-life; Vd, volume of distribution.
LEV Pharmacokinetic Dosing Comparison.
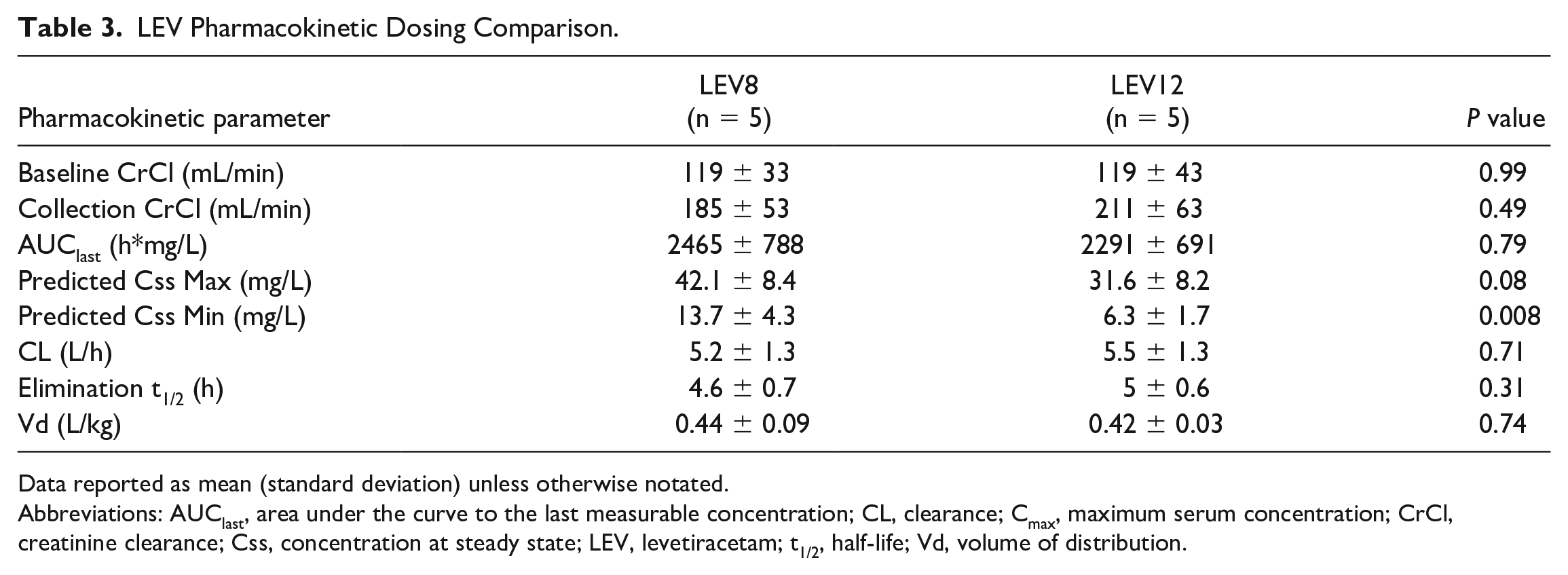
Data reported as mean (standard deviation) unless otherwise notated.
Abbreviations: AUClast, area under the curve to the last measurable concentration; CL, clearance; Cmax, maximum serum concentration; CrCl, creatinine clearance; Css, concentration at steady state; LEV, levetiracetam; t1/2, half-life; Vd, volume of distribution.
A total of 7 (70%) patients (5 [100%] LEV8, 2 [40%] LEV12) had levetiracetam trough concentrations between 6 and 20 mg/L. The probability of achieving Cssmin ≥6 mg/L and >20 mg/L for simulated dosing schemes is reported in Figure 1. LEV8 demonstrated a 99.5% probability of achieving trough concentrations ≥6 mg/L compared with 50.7% with LEV12. Toxicity assessment demonstrated a probability for trough concentrations >20 mg/L as 5.5% in the LEV8 group and 0% in the LEV12 group. Levetiracetam 500 mg every 12 hours had the lowest probability of achieving trough concentrations ≥6 mg/L at 1.5%. Regimens providing a total daily levetiracetam dose ≥2000 mg had the highest probability (>90%) of achieving target trough ≥6 mg/L except for levetiracetam 1000 mg every 12 hours (50.7%). Regimens providing a total daily levetiracetam dose >6000 mg had the highest probability of toxicity, with levetiracetam 2000 mg every 6 hours demonstrating a 99.8% probability of trough concentration >20 mg/L. The following levetiracetam dosing strategies demonstrated therapeutic target attainment: 500 mg every 6 hours, 1000 mg every 8 hours, and 2000 mg every 12 hours.
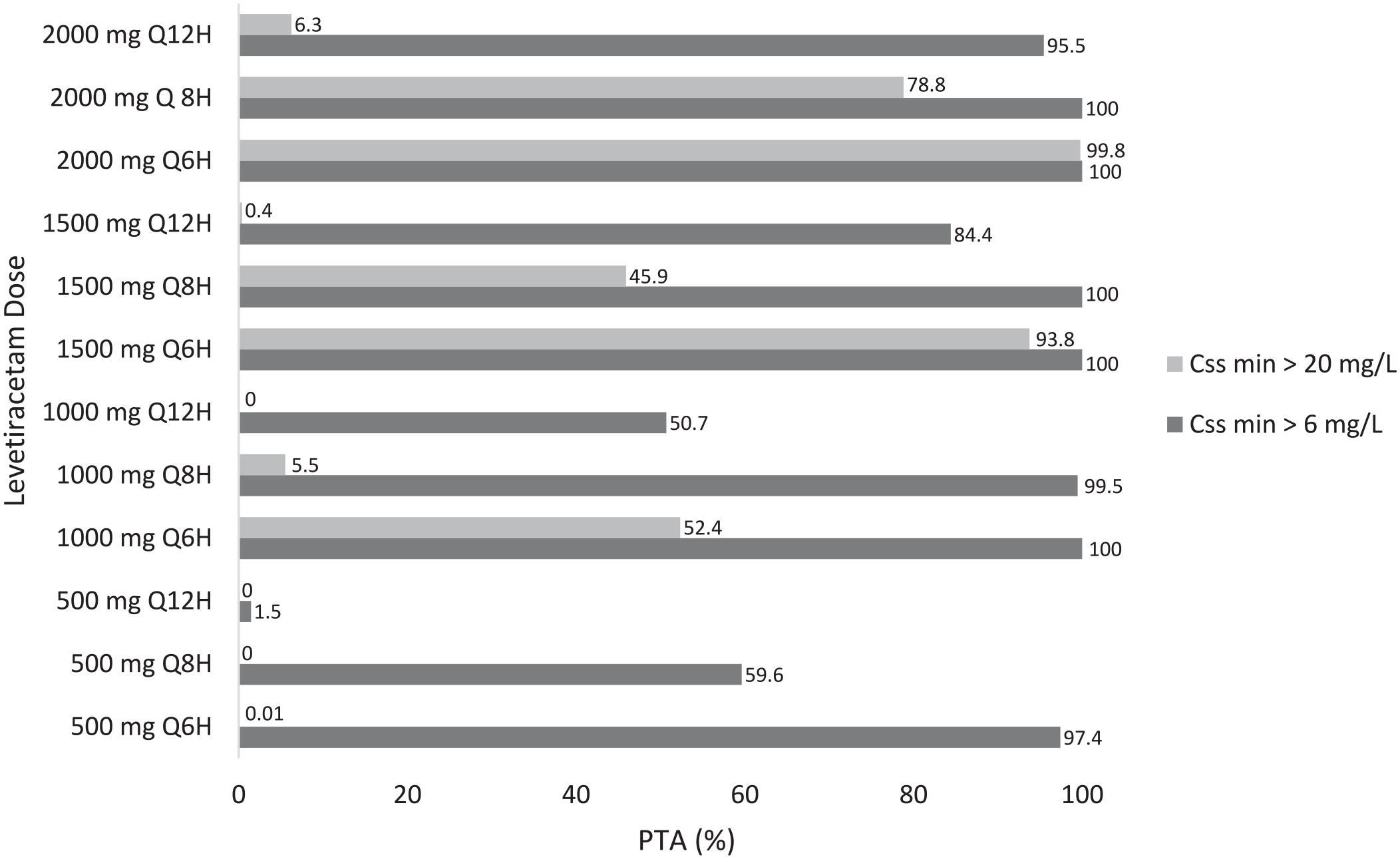
Probability of target attainment at steady state.
The PTA of a trough ≥6 mg/L and >20 mg/L stratified by weight category is reported in Figures 2a and b, respectively. Weights observed in this population ranged from 65 to 103 kg. A negative linear decrease in the probability of achieving a Cssmin ≥6 mg/L was observed with increasing weight category in the levetiracetam 500 mg every 8 hour, 1000 mg every 12 hour, 1500 mg every 12 hour, and 2000 mg every 12 hour regimens. A similar negative linear decrease was seen between increasing weight category and probability of achieving a Cssmin > 20 mg/L. Patients weighing <75 kg demonstrated therapeutic target attainment with levetiracetam 500 mg every 6 hours and 1500 mg every 12 hours. Patients weighing ≥75 kg demonstrated therapeutic target attainment with levetiracetam 500 mg every 6 hours, 1000 mg every 8 hours, and 2000 mg every 12 hours.
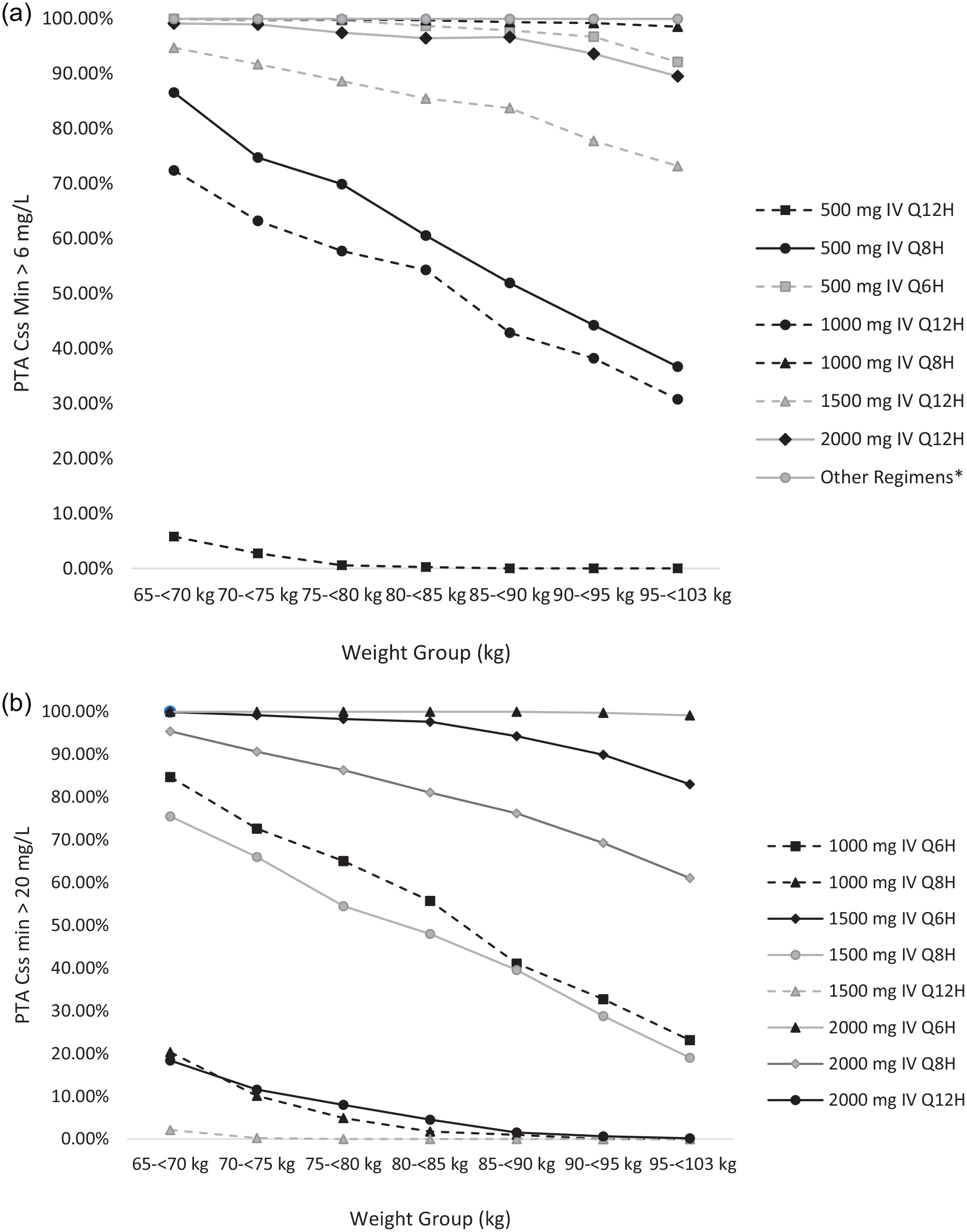
(a) Probability of target attainment stratified by weight: therapeutic threshold. (b) Probability of target attainment stratified by weight: Toxicity threshold.
Discussion
This study investigated levetiracetam dosing regimens for PTS prophylaxis in patients with sTBI receiving intravenous levetiracetam 1000 mg every 8 to 12 hours. To our knowledge, this study is the first to directly measure a 1000 mg every 8 hour intravenous dosing regimen. Study findings indicate better target levetiracetam concentration attainment with doses exceeding 1000 mg every 12 hours, achieved through more frequent administration and/or higher per-dose exposure. The LEV8 regimen demonstrated a higher PTA for trough concentrations ≥6 mg/L compared with LEV12 with an acceptably low incidence (< 10%) of trough concentrations >20 mg/L. Monte Carlo simulations predicted regimens of 500 mg every 6 hours, 1000 mg every 8 hours, and 2000 mg every 12 hours would achieve therapeutic target attainment. No patients in this study had clinical or electrographic seizure activity following levetiracetam administration.
Nine patients enrolled in this study demonstrated predicted ARC. The one remaining patient had an ARCTIC score of 6 but did not meet the defined CrCl threshold. Increased levetiracetam clearance of 5.3±1.2 L/h was observed in this population compared with 4 L/h in healthy volunteers. 1 In addition, the levetiracetam t1/2 of 4.8 ± 0.64 hours is faster than the package insert reported half-life of 6 to 8 hours. 23 These findings are similar to a previous pharmacokinetic evaluation of neurocritically ill patients (clearance [5.6 ± 1.8 L/h] and t1/2 5.2 ± 1.2 hours). 18 Another recent evaluation of levetiracetam PK in neurologically injured patients with confirmed ARC found a 50% decrease in serum trough concentration with each 40 mL/min increase in CrCl, highlighting the impact of ARC on levetiracetam elimination. 4 In conjunction, findings support more aggressive levetiracetam dosing regimens in this population.4,18 Levetiracetam has a wide safety margin and there is limited evidence supporting exposure-related toxicity.4,24 Due to the enhanced safety profile, more aggressive dosing regimens suggested for kinetic optimization in patients with enhanced renal elimination may be appropriate. 4 No adverse events were reported in this study utilizing a more aggressive 1000 mg every 8 hour regimen.
A strong association between target levetiracetam trough concentrations and clinical efficacy for PTS prophylaxis has yet to be established. Therapeutic drug monitoring (TDM) of levetiracetam is not commonly used for prophylaxis but it has shown a potential role for dose optimization in epilepsy. 25 Therapeutic drug monitoring can potentially be used to evaluate the impact of altered PK in critically ill populations and aid in determining levetiracetam doses needed to achieve target concentrations for seizure prevention. While a variety of target trough concentrations have been evaluated, a conservative goal of 6 to 20 mg/L has been suggested.17,18,26 In this evaluation, Cssmin for LEV8 was significantly higher than LEV12 (13.7 ± 4.3 mg/L vs 6.3 ± 1.7 mg/L); however, both resulted within the target range. No study patient had levetiracetam trough concentrations >20 mg/L. These results are similar to a previous MCS evaluation of neurocritically ill patients. 18 In this evaluation, the optimal regimen for therapeutic target attainment was found in levetiracetam 500 mg every 6 hours, 1000 mg every 8 hours, and 2000 mg every 12 hours regimens.
Weight-based dosing of levetiracetam is commonly used for treatment of status epilepticus, but seizure prophylaxis recommendations are often fixed-dose regimens.27,28 A secondary analysis stratified by weight found decreased PTA of trough concentrations ≥6 mg/L with increasing weight category for levetiracetam 1000, 1500, and 2000 mg every 12 hours groups. A weight breakpoint of 75 kg was identified as a possible threshold for dose adjustments, with doses of levetiracetam 1000 mg every 8 hours and 2000 mg every 12 hours demonstrating therapeutic target attainment in patients weighing >75 kg. These same regimens, however, demonstrated a >10% PTA of trough concentrations >20 mg/L in patients weighing <75 kg. Conversely, levetiracetam 1500 mg every 12 hours demonstrated therapeutic trough attainment in patients weighing <75 kg but had a <90% PTA for trough concentrations ≥6 mg/L in patients >75 kg. To our knowledge, this is the first study to evaluate the impact of weight on achieving levetiracetam target concentrations for seizure prophylaxis and suggest there may be a role for weight-tiered assessment when determining the optimal dosing regimen for seizure prophylaxis in sTBI.
There were several limitations to this study. While initial intent was to enroll up to 20 patients, enrollment was stopped after 10 patients for feasibility and resource availability during the COVID-19 pandemic. Patients enrolled in this study were from a single institution, and while all screened patients meeting inclusion criteria were approached for consent, all study patients were men and 80% were Caucasian. Only severe TBI patients were included in this evaluation, limiting generalizability to other neurologically injured populations. The predicted presence of ARC was assessed using ARCTIC score and estimated CrCl; however, an ARCTIC score > 6 has a positive predictive value of 68%, limiting the ability to definitively confirm the presence of ARC. No direct creatinine measurement, such as a 24-hour urine creatinine collection, was collected to definitively assess the presence of ARC. In addition, this study only assessed renal function at the time of sample collection and did not account for fluctuating renal function often observed in critical illness. The role of levetiracetam TDM in clinical practice is limited and a variety of serum trough concentrations have been proposed. Some evaluations have suggested a more aggressive trough concentration range of 12 to 46 mg/L; however, this target has not been shown to improve clinical outcomes.4,29,30 The small sample size of patients enrolled in this study limits the ability to fully evaluate the clinical efficacy and safety of a more aggressive levetiracetam regimen.
Conclusion and Relevance
Severe TBI patients receiving LEV8 or LEV12 in this study demonstrated rapid systemic clearance and a short elimination half-life. Regimens of levetiracetam 500 mg every 6 hours, 1000 mg every 8 hours, or 2000 mg every 12 hours may be required for optimal therapeutic target attainment. Patient weight of 75 kg may serve as a breakpoint for weight-guided dosing to optimize levetiracetam therapeutic target attainment. This study is the first to directly measure a levetiracetam 1000 mg every 8 hour intravenous regimen and suggest weight-guided dosing for seizure prophylaxis, however future multicenter evaluations are needed to validate these findings.
Supplemental Material
sj-docx-1-aop-10.1177_10600280231202246 – Supplemental material for Pharmacokinetics of Levetiracetam Seizure Prophylaxis in Severe Traumatic Brain Injury
Supplemental material, sj-docx-1-aop-10.1177_10600280231202246 for Pharmacokinetics of Levetiracetam Seizure Prophylaxis in Severe Traumatic Brain Injury by Sarah Schuman Harlan, Carolyn D. Philpott, Shaun P. Keegan, Molly E. Droege, Aniruddha S. Karve, Brandon Foreman, Devin Wakefield, Eric W Mueller, Kiranpal Sangha, Laura B. Ngwenya, Joshua D. Courter, Pankaj Desai and Christopher Droege in Annals of Pharmacotherapy
Footnotes
Acknowledgements
Thank you to Margaret M Powers-Fletcher and Kristin Weghorm for assistance in coordinating collaboration with UC Clinical Laboratory services. Thank you to Roman Jandarov for assistance in statistical plan design. Thank you to John Shinn and Katelin Roth for assisting with patient enrollment. Thank you to Julie Farrar for critical manuscript review.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.F. received honoraria from UCB Pharma and serves on the scientific advisory boards for Marinus Pharmaceuticals, Inc and SAGE Therapeutics. He receives research funding from the National Institutes of Health, US Department of Defense, and National Science Foundation and is the site principal investigator for studies funded by Biogen, Inc and Marinus Pharmaceuticals, Inc. B.F. has no relevant conflicts of interest to this research. L.B.N. conducts traumatic brain injury–related research funded by grants to the University of Cincinnati College of Medicine from Abbott Laboratories and Biogen, Inc. L.B.N. has no relevant conflicts of interest to this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the American College of Clinical Pharmacy Critical Care Pharmacy and Research Network.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.