
Abstract
Introduction
Traumatic brain injury (TBI) represents a significant burden in critical care settings resulting in nearly 200 related deaths per day in the United States, disproportionately affecting the geriatric population due to age related vulnerability.1,2 After a TBI occurs, patients are at an increased risk of developing posttraumatic seizures (PTS), which can increase mortality and exacerbate neurological issues including increased intracranial pressure (ICP), delayed neurological recovery and inappropriate neurotransmitter release. 3 Posttraumatic seizures can be characterized as early onset (≤ 7 days from TBI) or late onset (>7 days from TBI). 3
Guidelines from the Brain Trauma Foundation suggest the use of antiepileptic agents for hospitalized patients during the first 7 days following the TBI, as early PTS have been reported as high as 12%. 4 Historically, phenytoin has been used for early PTS prophylaxis in critically ill patients in order to mitigate unwanted complications, however, retrospective data indicate that levetiracetam is a viable option for the prophylaxis against PTS. A study by Patanwala et al 5 evaluated patients who had received phenytoin for seizure prophylaxis, and found that it increased length of hospital stay and patients had worse functional outcomes long-term. A second analysis conducted by Ohman and colleagues supported the use of levetiracetam for PTS prophylaxis, along with determining that there is no statistically significant difference in PTS within 7 days when levetiracetam is dosed at 500 mg twice daily, 750 mg twice daily, or 1000 mg twice daily. 6 Phenytoin may also be a less favorable option due to numerous drug interactions and known pharmacokinetic idiosyncrasies. 7
Levetiracetam, a soluble ethyl analogue of the nootropic agent piracetam, is utilized primarily for the treatment of epilepsy. Its unique effects are induced by binding to the synaptic vesicle SVA2, a protein known to modulate synaptic vesicle exocytosis and neurotransmitter release. 8 When compared to phenytoin, levetiracetam has preferrable pharmacokinetic and pharmacodynamic properties, has equipotent intravenous and oral doses with nearly 100% bioavailability, and does not routinely require therapeutic drug monitoring.7,9 Despite the favorable drug characteristics as opposed to the traditional use of phenytoin, levetiracetam has been associated with neuropsychiatric events, including agitation, delirium, hallucinations, mania, and aggression.2,10 Geriatric patients also have a higher risk of developing adverse drug reactions and levetiracetam has been listed in the 2019 Beer’s Criteria List as one to be used in caution with reduced kidney function due to the potential for neuropsychiatric events. 11
The objective of this evaluation was to determine the incidence of neuropsychiatric effects of levetiracetam when utilized for PTS prophylaxis.
Methods
This retrospective cohort analysis was conducted at The University of Toledo Medical Center, a 300-bed, Level II trauma academic medical center located in Toledo, Ohio, USA. Institutional review board approval was obtained prior to the initiation of the study. Patients admitted to the surgical intensive care unit (SICU) at The University of Toledo Medical Center between January 1, 2023, and March 15, 2025, were eligible for inclusion. Patients were included if they were at least 18 years of age and received a dose of levetiracetam for seizure prophylaxis associated with a TBI. The indication for levetiracetam was clearly stated in the patient medical records by the healthcare provider. Patients were excluded if they received levetiracetam for a different indication, were taking levetiracetam as a home medication, or if they were ineligible to receive levetiracetam due to a clinical contraindication or other consideration documented by the attending physician. Patient data were obtained directly from the electronic medical record. The primary study outcome was to assess the incidence of neuropsychiatric events attributed to levetiracetam. Secondary outcomes included levetiracetam dose/route, seizure occurrence, time to onset of neuropsychiatric event, SICU length of stay, and duration of levetiracetam treatment.
Results
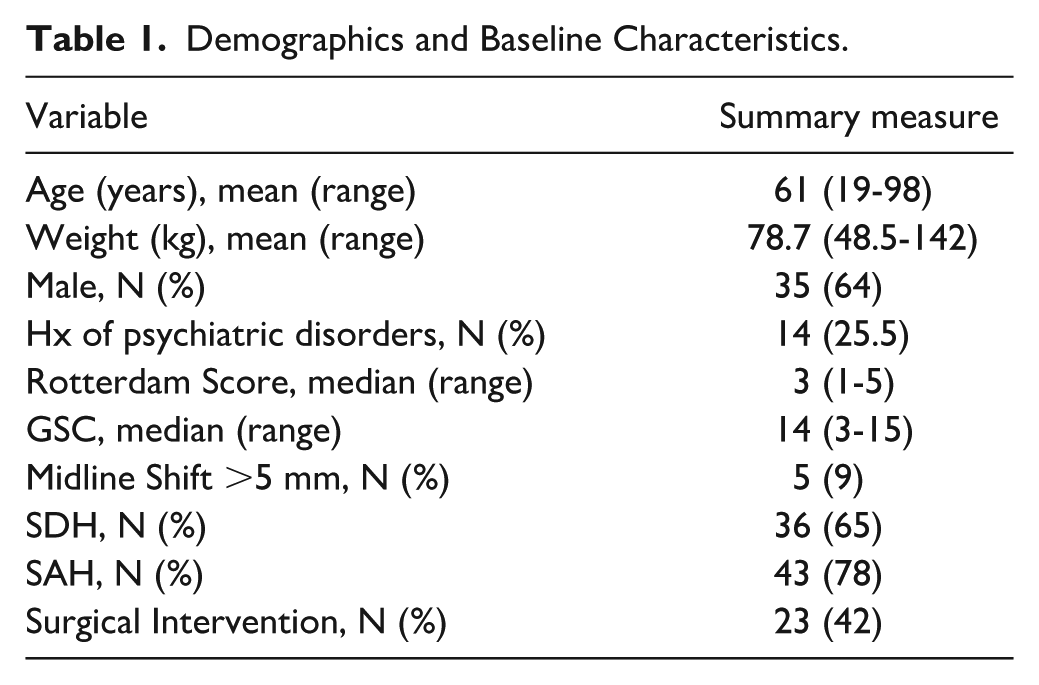
Of the 122 patients who were screened, 55 patients met the inclusion criteria and were included in the final analysis. Baseline demographic and clinical characteristics are presented in Table 1. Primary and secondary outcomes are summarized in Table 2. Regarding baseline characteristics, it should be noted that the psychiatric disorders for the participants included substance abuse, anxiety, depression, personality disorder, bipolar, attention-deficit/hyperactivity disorder (ADHD), and suicidal ideation/self-harm. Of the 14 patients (25.5%) with a history of psychiatric disorders, only 1 of those patients experienced a neuropsychiatric event while receiving levetiracetam.
Demographics and Baseline Characteristics.
Primary and Secondary Endpoints.
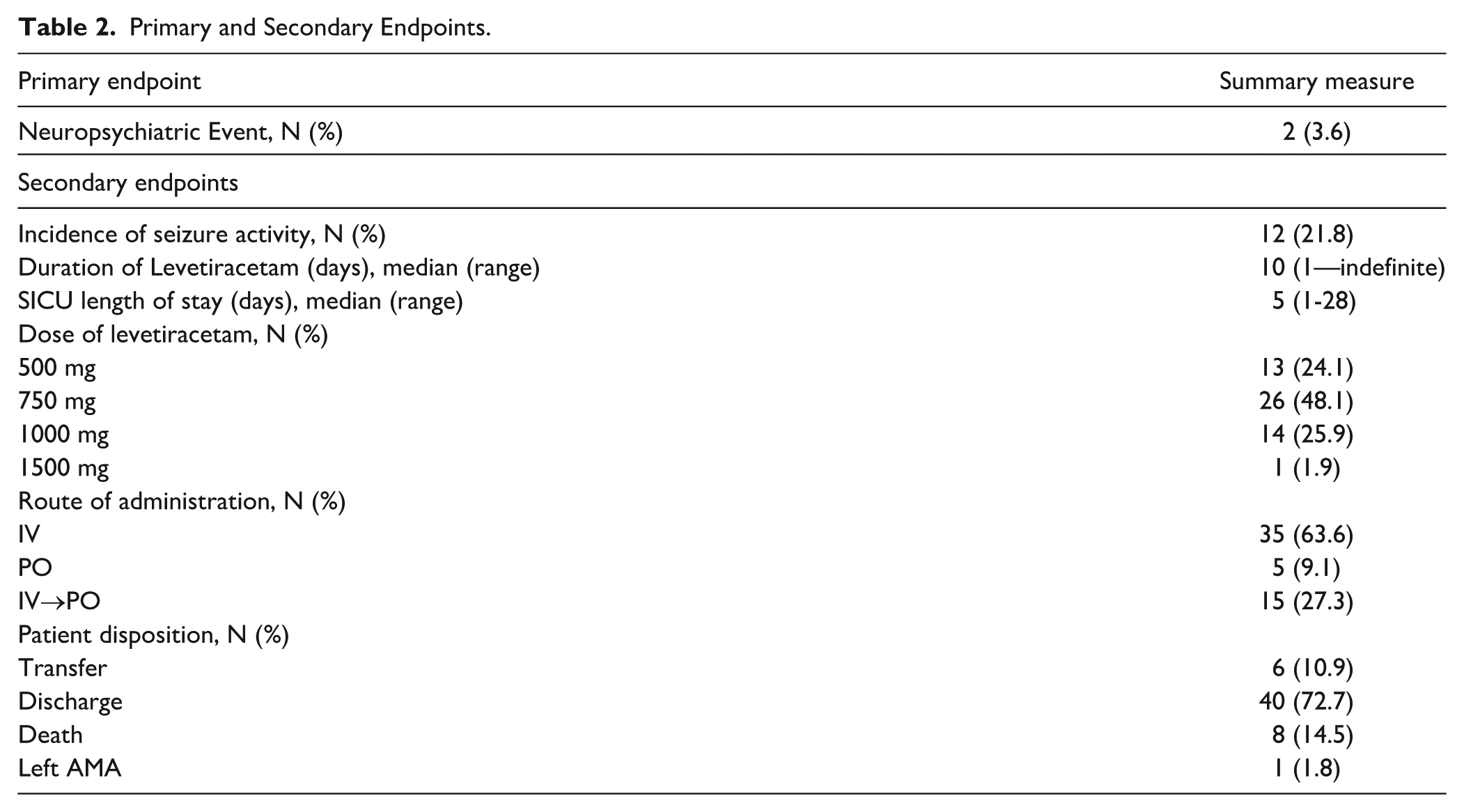
For the primary outcome, 2 patients (3.6%) experienced a neuropsychiatric event while receiving levetiracetam. The first case was a 49.8 kg, 98-year-old with a Glasgow Coma Scale (GCS) of 14 and a Rotterdam score of 2. Upon admission following a fall, computed tomography (CT) scans showed a 1-cm left, frontoparietal, temporal lobe subdural hematoma (SDH) with mild mass effect and a midline shift to the right of approximately 2 mm. She was given 500 mg of levetiracetam by mouth twice daily for 5 doses. Approximately 20 hours after initiation of oral levetiracetam, the nurse documented episodes of agitation and the patient was switched to oral lacosamide 50 mg twice daily. The second case was a 61.8 kg, 77-year-old with a GCS of 15 and a Rotterdam score of 3. Upon admission following a fall, CT scans showed an acute bifrontal SDH and subarachnoid hemorrhage (SAH) measuring 10 mm on the right and 8 mm on the left. The CT scan also identified an intraparenchymal hemorrhage within the inferior left temporal lobe, but no evidence of midline shift. She was given 750 mg of intravenous (IV) levetiracetam twice daily and on day 3, lorazepam 0.5 mg was added to her antiepileptic regimen. Approximately 72 hours after initiation of levetiracetam, the critical care team reported altered mental status and ordered 2 doses of oral olanzapine 5 mg. After a week of receiving levetiracetam, the neurosurgery team discontinued the order and noted it to be the offender for the disorientation, and lorazepam was continued for further seizure prophylaxis.
Regarding secondary outcomes, 10 patients (18.2%) had breakthrough seizure activity during therapy. The median duration of levetiracetam administration was 10 days, ranging from a single dose to indefinite outpatient use. The median length of stay in the SICU was 5 days, with a range of 1 to 28 days. As shown in Table 2, 35 patients received levetiracetam exclusively via the IV route, 5 received oral therapy only, and 15 were transitioned from IV to oral administration for continued inpatient or outpatient use. Dosing regimens ranged from 500 mg every 12 hours to 1500 mg every 12 hours. A total of 9 patients (16%) received a loading dose, which varied from 750 mg to 2 g. One patient received a single loading dose of levetiracetam and died before maintenance therapy could be initiated. Regarding disposition, among the six patients who were transferred, destinations included hospice care, skilled nursing facilities, trauma rehabilitation centers, or other institutions. Notably, 1 patient elected to leave the hospital against medical advice.
Discussion
The study results showed remarkably low incidence of neuropsychiatric events, thus, supporting the assumption that levetiracetam is a safe and well-tolerated treatment option for seizure prophylaxis in patients who have suffered a TBI. Out of the 55 participants included in the final analysis, only 2 (3.6%) had adverse events attributed to levetiracetam administration and were consequently switched to an alternative therapy. Of note, both affected participants were over the age of 75, female, and weighed less than 80 kg. These clinical findings may suggest population-dependent vulnerability to levetiracetam in elderly, low-weight females. 12
In addition to evaluating the incidence of neuropsychiatric events, several key findings were revealed about clinical decision-making with regards to the use of levetiracetam for seizure prophylaxis following a TBI. Our study reinforces the findings from Ohman et al, 6 demonstrating that higher doses of levetiracetam does not correlate to improved functional outcomes. Similar to their results, we did not observe a significant difference in early PTS incidence, hospital length of stay or overall mortality across levetiracetam dosing regimens. These findings emphasize the notion that dose escalation does not increase efficacy, supporting the clinical utility of lower-dose regimens which will also decrease the risk of neuropsychiatric events. In addition, the data highlight that seizure prophylaxis is commonly continued beyond the recommended 7-day treatment window, despite available evidence disproving improved outcomes. 3 Unnecessary extensions of levetiracetam therapy beyond guideline recommendations may inadvertently increase the risk of duration-dependent adverse effects, including agitation, aggression and mood disturbances. Collectively, these findings support the analysis conducted by Patanwala and colleagues that clinicians should prioritize the minimum effective dose, for the shortest effective duration in order to reduce neuropsychiatric events while maintaining adequate seizure prophylaxis. 5 Although strategies exist to minimize adverse events related to levetiracetam administration, close monitoring remains essential, particularly in the elderly population with additional risk factors for psychiatric complications. 2
In regard to efficacy, levetiracetam revealed poor performance, with 12 of the 55 participants (21.8%) experiencing seizure activity following administration. This represents a notable disparity from existing literature, where seizure rates are frequently reported to be less than 5% in severe TBI and under 2% in mild to moderate cases. 13 However, our findings may have overestimated the true incidence due to inclusion criteria used for data collection. Specifically, we recorded seizures that were visually reported or electrographically confirmed during the patient’s entire hospital stay. Other studies differ by employing a narrower research question, which specifies seizures identified by electroencephalogram within the first 7 days following TBI. 13 With regard to our data, 12 patients (21.8%) had a documented seizure, but only six (10.9%) had seizures that were electrographically recorded and just five (9.1%) of the confirmed seizures occurred within the defined 7-day window of early PTS. This discrepancy between documented and confirmed seizure incidence may have inflated the overall incidence rate in our study and highlights the variability of seizure documentation in clinical practice. Therefore, while our data suggest poor prophylactic ability of levetiracetam in patients post-TBI, the true incidence is lower when aligned to the traditional definitions used in other studies.
There were several limitations to this study. As a retrospective chart review study, it was inherently prone to inaccuracy and completeness due to variable charting documentation of the medical records. There was also a limited sample size because most participants received a treatment dose of levetiracetam due to seizure activity or were taking levetiracetam as a home medication. While the Richmond Agitation-Sedation Scale (RASS) and Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) scores were initially intended to be included in this evaluation as potential confounding variables, the data were either not available for review or not documented appropriately for the majority of our patients, thereby prohibiting the inclusion of these scores in our evaluation. Additionally, the study was conducted at a single, moderate sized level II trauma medical center, where patients may present with milder cases of TBI.
Conclusion
The results of this study support levetiracetam as a practical antiepileptic agent for PTS prophylaxis in TBI patients. Although a low incidence of adverse events were reported, clinicians should be cautious with administration in the geriatric population due to an increased risk of neuropsychiatric side effects. Levetiracetam should be considered a reliable and safe agent for seizure prophylaxis in TBI patients, however, it’s superiority to other agents has yet to be determined.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.