
Abstract
Background:
Acute kidney injury (AKI) is common in critically ill patients, but the optimal dosing of beta-lactam antibiotics in this setting remains controversial. It is not known whether the benefit of initiating beta-lactams at normal doses outweighs the risk of accumulation and toxicity.
Objective:
We aimed to evaluate the association between early dose adjustment of piperacillin/tazobactam (PT) and 28-day intensive care unit (ICU) mortality in critically ill patients with AKI.
Methods:
We conducted a retrospective multicenter cohort study using the eICU Collaborative Research Database v2.0 and included adult ICU patients with AKI who received PT and had a pretreatment serum creatinine level corresponding to an estimated glomerular filtration rate (eGFR) <40 mL/min/1.73 m2. The exposure was PT dose in the first 24 hours, which was categorized as normal (≥13.5 g/24 h) or adjusted (<13.5 g/24 h). The primary outcome was 28-day ICU mortality.
Results:
Among 1639 eligible patients, 224 (13.7%) received normal-dose PT and 1415 (86.3%) received adjusted doses. The overall 28-day ICU mortality was 11%, with significantly lower mortality in the normal-dose group (6.7%) compared with the adjusted-dose group (11.7%) (unadjusted odds ratio [OR] 1.85, 95% confidence interval [CI] 1.07-3.20; P = .028). After multivariable adjustment, early dose adjustment was independently associated with higher 28-day ICU mortality (adjusted OR 2.11, 95% CI 1.13-3.96; P = .020). Results were consistent across multiple subgroup and sensitivity analyses, but statistical significance was attenuated when the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation was used for eGFR estimation.
Conclusion and Relevance:
Early dose adjustment of PT in critically ill patients with AKI is associated with increased 28-day ICU mortality. This finding suggests that renal dose adjustment of PT should be deferred beyond the first 24 hours of therapy in this population. Prospective studies are needed to confirm this finding, define the optimal timing of subsequent dose adjustments, and assess safety outcomes.
Keywords
Introduction
Dosing antimicrobials for critically ill patients with acute kidney injury (AKI) is challenging. An expert consensus by the Kidney Disease: Improving Global Outcomes (KDIGO) recommends initiating hydrophilic antimicrobials such as beta-lactams at normal or near-normal maintenance doses, followed by dose adjustments on the basis of therapeutic drug monitoring (TDM) or, if unavailable, clinical monitoring of efficacy and safety. 1 This recommendation is based on pharmacokinetic (PK) changes in this population; 1 however, the clinical impact of this strategy has not been previously evaluated.
Beta-lactams have time-dependent bactericidal activity, with their efficacy determined by the proportion of the dosing interval during which free drug concentrations remain above the bacterial minimum inhibitory concentration (% fT > MIC). 2 Early dose adjustment of beta-lactams may result in subtherapeutic concentrations, potentially leading to treatment failure and increased mortality in patients with sepsis.
Limited studies have compared the clinical outcomes of the normal-dose strategy of beta-lactam antimicrobials with those of early dose adjustment in patients with AKI, yielding conflicting results. Two retrospective studies reported no differences in mortality or clinical recovery between the 2 dosing strategies.3,4 However, these studies had small sample sizes, and one of them 3 was not restricted to critically ill patients and lacked adjustment for the confounding effect of AKI on clinical outcomes. In contrast, early dose adjustment of antipseudomonal beta-lactams was associated with an increased risk of in-hospital mortality in another prospective study. 5
Piperacillin/tazobactam (PT) is the most commonly prescribed beta-lactam in critically ill patients because of its broad spectrum against Gram-positive, Gram-negative, and anaerobic bacteria.6,7 It represents an ideal model for evaluating the dosing of beta-lactams in AKI because it relies on renal function for elimination. 6 While early dose adjustment of PT may decrease its antimicrobial efficacy, the normal-dose strategy poses safety risks due to its concentration-dependent neurotoxicity.8,9 De Corte et al 10 found that PT levels often exceed the neurotoxicity threshold in critically ill patients with AKI, even when doses are adjusted. Therefore, it is crucial to evaluate whether the potential toxicity of the normal-dose strategy is outweighed by a clear benefit in terms of sepsis-related outcomes. In this study, we aimed to evaluate the association between early adjustment of PT maintenance dose and mortality in critically ill patients with AKI.
Method
Design and Population
This was a retrospective multicenter cohort study using the eICU Collaborative Research Database (eICU-CRD) v2.0, a published data set of over 200 000 critical care admissions across the United States between 2014 and 2015, 11 and the largest and most diverse publicly available intensive care unit (ICU) data set. 12 We included adult patients (≥18 years old) with AKI who received PT and had a pretreatment serum creatinine (SCr) value corresponding to an estimated glomerular filtration rate (eGFR) <40 mL/min/1.73 m2 based on the Modification of Diet in Renal Disease (MDRD) equation. The AKI was defined as either a pretreatment SCr at least 0.3 mg/dL above baseline 13 or an elevated SCr without a documented history of chronic kidney disease (CKD). The baseline SCr level was defined as the lowest value during the admission. This eGFR cutoff was chosen to exclude patients whose renal function, despite AKI, would not typically warrant dose adjustment in clinical practice. Owing to missing or implausible recorded weights, the MDRD equation, which does not require weight input, was used to estimate the eGFR.
We excluded patients who received renal replacement therapy before or within 24 hours of PT initiation, patients who received PT for less than 24 hours, patients who died or were discharged within 24 hours of PT initiation, patients whose PT therapy was interrupted for 12 hours or more, patients started on PT earlier than 24 hours prior to ICU admission, and patients with incomplete details of doses and frequencies of PT therapy.
Exposure, Outcomes, and Covariates
The exposure was the cumulative PT dose in the first 24 hours calculated from PT orders (Supplemental Appendix A) and was categorized as normal dose (≥13.5 g/24 h) or adjusted dose (<13.5 g/24 h). This cutoff of ≥13.5 g/24 h was chosen to represent the ‘normal or near-normal initial maintenance dose’ strategy recommended by KDIGO for dosing hydrophilic antimicrobials in critically ill patients with AKI. 1 Given the overlap in recommended doses across different degrees of renal dysfunction and the inability to determine whether renal adjustment was applied to the regimen of 4.5 g every 6 hours or 4.5 g every 8 hours, we selected a low cutoff of 13.5 g as a conservative approach that would be expected to shift the effect estimate toward the null.
The primary outcome was 28-day ICU mortality. Covariates were determined a priori based on domain knowledge and directed acyclic graphs; they included age, sex, hypertension, diabetes, CKD, liver cirrhosis, immunosuppression, sepsis or septic shock at admission, Acute Physiology and Chronic Health Evaluation (APACHE) IV score at admission, intubation at admission, vasopressor therapy before PT initiation, time from ICU admission to PT initiation, and the first PT dose. Vasopressor therapy was defined as the infusion of norepinephrine, epinephrine, phenylephrine, dopamine, or vasopressin within 24 hours before PT therapy. We planned to collect data on infusion times of PT, but these data were not available in the eICU-CRD. The data sources of these variables are detailed in Supplemental Appendix B.
Statistical Analysis
Categorical data were summarized as frequencies with percentages and continuous data as medians with interquartile ranges (IQRs). Chi-square or Fisher’s exact tests were used for comparing categorical data, and Wilcoxon rank-sum test was used for comparing continuous and ordinal variables. Multivariable logistic regression was used to evaluate the association between PT dosing strategy and 28-day ICU mortality with results expressed as odds ratios (ORs) with 95% confidence intervals (CIs). Covariates were included in the initial models, and the final models were selected through backward elimination by removing covariates with P values > .2 based on the Wald test. In all models, robust variance estimators were used to account for clustering at the hospital level. Goodness of fit was assessed using the Hosmer-Lemeshow test. Missing data on APACHE IV score (12.6%), intubation status (2.6%), and immunosuppression (2.6%) were handled using multiple imputation by chained equations. The probability of survival over time was visually presented using an unadjusted Kaplan-Meier survival estimator in which time zero was set at the initiation of PT and survival was estimated separately for each study group.
To assess the robustness of the results, we conducted 3 sensitivity analyses: a complete case analysis excluding patients with missing data, a second analysis restricted to patients with AKI based on the KDIGO criteria, and a third analysis using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation instead of the MDRD equation for evaluating the inclusion criterion of eGFR <40 mL/min/1.73 m2. The covariates included in the sensitivity analyses were those retained in the final model of the primary analysis.
In addition, the primary outcome was investigated in the following subgroups: patients receiving vasopressor therapy before PT and patients with sepsis or septic shock at admission. Heterogeneity between subgroups was assessed using interaction terms in the regression model. In all analyses, P values of less than .05 were considered statistically significant. Data were extracted from the eICU-CRD using PostgreSQL 15.2 and analyzed using Stata version 17.
Results
Study Population
Among 16 268 PT-treated patients in the eICU-CRD, 1639 met the inclusion criteria (Figure 1). Of these, 224 (13.7%) received a normal dose and 1415 (86.3%) received an adjusted dose. Overall, the median age was 70 years (IQR 58-80 years), and approximately half of the patients were male. The prevalence of hypertension and diabetes was 55.9% and 39.8%, respectively. CKD was less common in patients who received a normal dose (11.2% vs 17%, P = .028). Liver cirrhosis and immunosuppression were present in less than 5% of both groups.
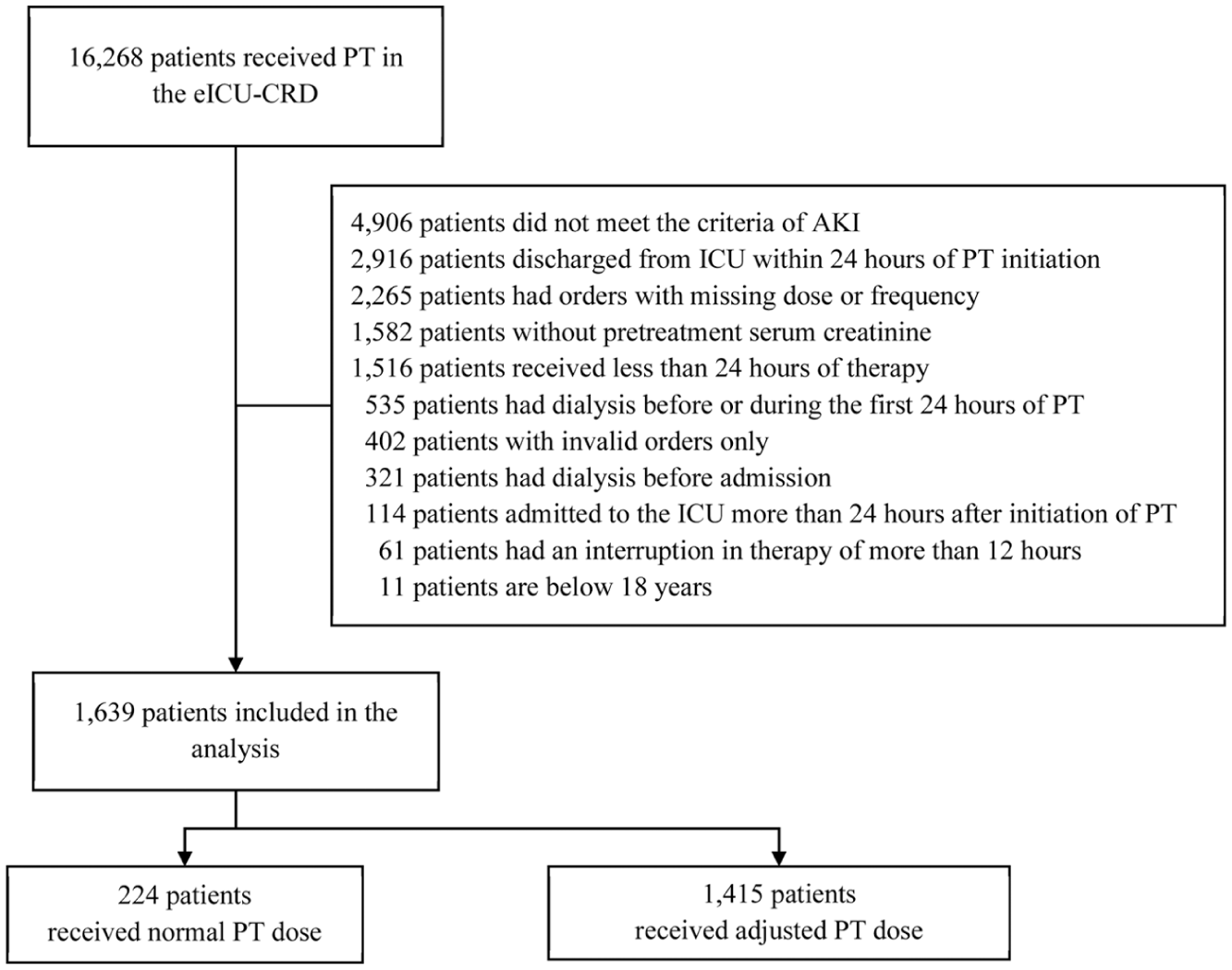
Flow chart of included patients with reasons for exclusion.
Fewer patients in the normal-dose group had sepsis or septic shock at ICU admission (38.4% vs 48.7%, P = .004) or were receiving vasopressor therapy before PT (16.5% vs 22.6%, P = .041). More patients in the normal-dose group were intubated at ICU admission (49.3% vs 40.6%, P = .015). Admission APACHE IV scores were similar between the 2 groups (P = .56). The baseline characteristics of both groups are detailed in Table 1.
Baseline Characteristics of the Included Patients Stratified by Piperacillin/Tazobactam Dosing Strategy.
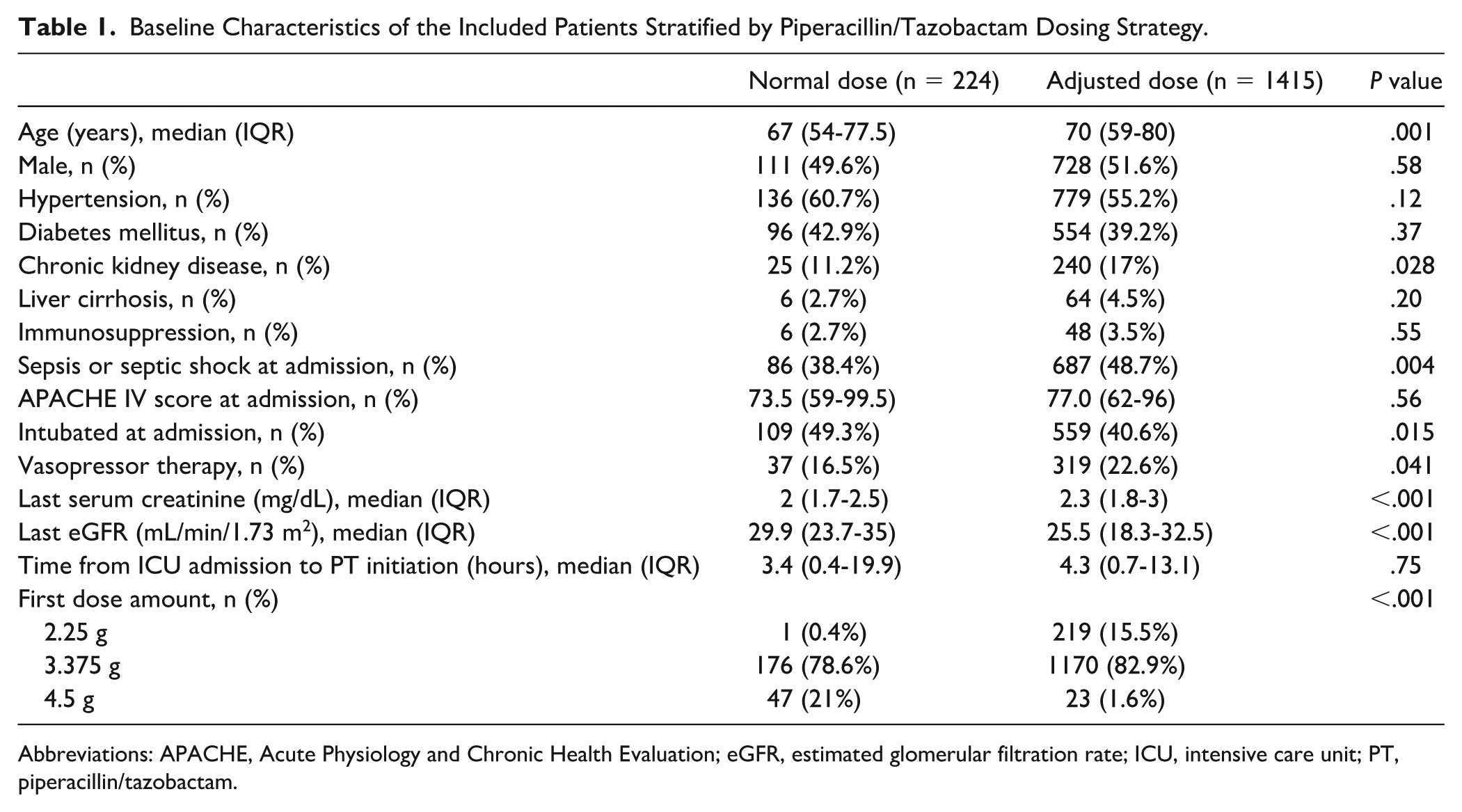
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; eGFR, estimated glomerular filtration rate; ICU, intensive care unit; PT, piperacillin/tazobactam.
Piperacillin/Tazobactam Therapy Details
The median pretreatment SCr for the overall cohort was 2.2 mg/dL (IQR 1.8-3 mg/dL), which was lower in the normal-dose group than in the adjusted-dose group (P < .001). The overall median eGFR prior to PT therapy was 26.4 mL/min/1.73 m2 (IQR 18.9-33 mL/min/1.73 m2), which was higher in the normal-dose group than in the adjusted-dose group (P < .001) (Table 1). The median time from ICU admission to PT initiation was 4.2 hours (IQR 0.7-13.4 hours). Overall, most patients received 3.375 g as the first PT dose, but more patients in the normal-dose group received 4.5 g. The cumulative dose in the first 24 hours of therapy ranged from 13.5 to 18 g in the normal-dose group and from 4.5 to 12.375 g in the adjusted-dose group. The median duration of PT therapy was 2.7 days (IQR 1.7-4.9 days) in the normal-dose group and 3 days (IQR 1.9-5 days) in the adjusted-dose group.
Outcomes
By 28 days following PT therapy initiation, 181 patients (11%) died: 166 (11.7%) in the adjusted-dose group and 15 (6.7%) in the normal-dose group (crude OR 1.85, 95% CI 1.07-3.20; P = .028). Figure 2 shows the unadjusted survival curves by PT dosing strategy. In the multivariable logistic regression model, dose adjustment was independently associated with more than a twofold increase in the odds of 28-day ICU mortality (adjusted OR 2.11, 95% CI 1.13-3.96; P = .02) (Table 2, Supplemental Appendix C).
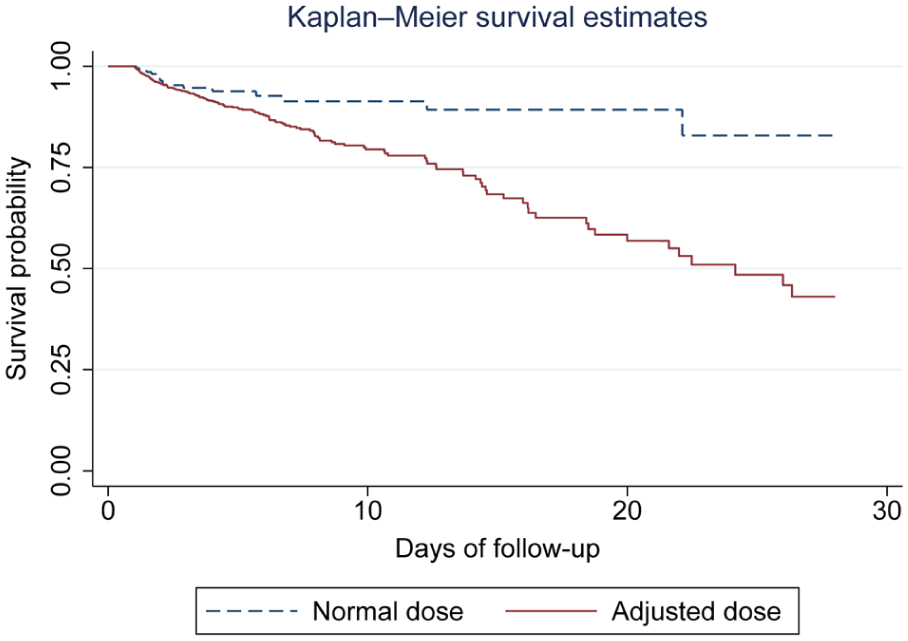
Kaplan-Meier survival curves comparing time to death between normal and adjusted dosing of piperacillin/tazobactam over 28 days of follow-up.
Logistic Regression Models of the Association of Early Dose Adjustment of PT With ICU Death at 28 Days.
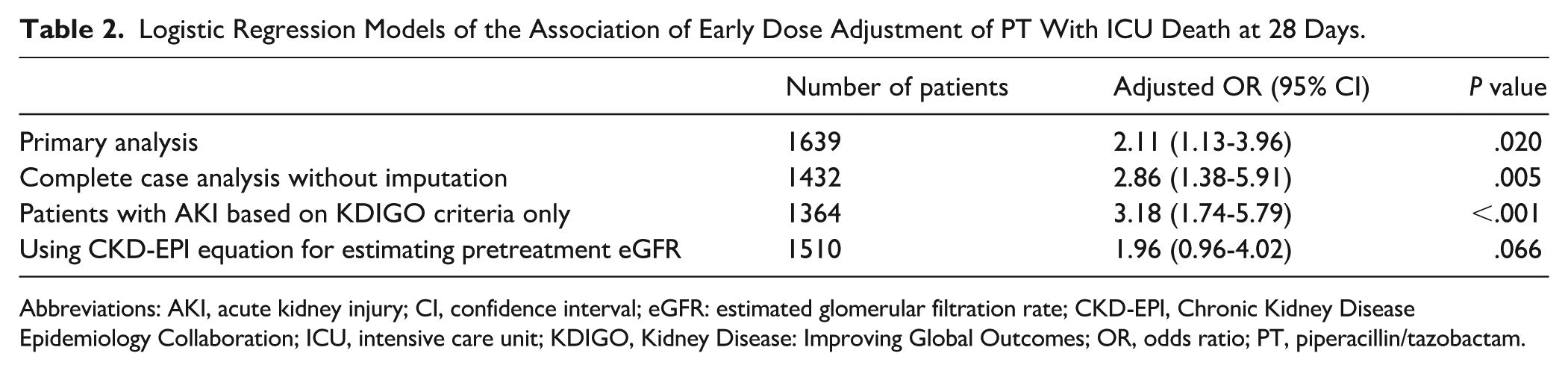
Abbreviations: AKI, acute kidney injury; CI, confidence interval; eGFR: estimated glomerular filtration rate; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; ICU, intensive care unit; KDIGO, Kidney Disease: Improving Global Outcomes; OR, odds ratio; PT, piperacillin/tazobactam.
A complete case analysis excluding patients with missing data yielded consistent results (n = 1432; adjusted OR 2.86, 95% CI 1.38-5.91; P = .005) (Table 2, Supplemental Appendix D). Similarly, a sensitivity analysis restricted to patients with AKI based on the KDIGO criteria revealed a consistent association of PT dose adjustment with increased odds of 28-day ICU mortality (n = 1364; adjusted OR 3.18, 95% CI 1.74-5.79; P < .001) (Table 2, Supplemental Appendix D). In another sensitivity analysis, using the CKD-EPI equation instead of the MDRD equation for eGFR estimation, the association of PT dose adjustment with higher odds of 28-day ICU mortality was not statistically significant (n = 1510; adjusted OR = 1.96, 95% CI 0.96-4.02; P = .066) (Table 2). In a post hoc exploratory analysis of patients with pretreatment MDRD eGFR less than 20 mL/min/1.73 m2 (n = 459), the primary outcome occurred in 12.7% of the patients who received adjusted doses, while none of the patients who received normal doses developed the primary outcome (P = .058, adjusted OR could not be calculated due to zero events in the normal-dose group).
Two subgroup analyses according to vasopressor therapy before PT therapy and according to sepsis or septic shock at admission showed a consistent association of dose adjustment with 28-day ICU mortality (Figure 3). Among patients discharged alive from the ICU, the median time from PT initiation to ICU discharge was 3.5 days (IQR 2.1-6.3 days). The normal-dose group had a longer time to ICU discharge (median 4.2 days; IQR 2.3-9.9 days) compared with the adjusted-dose group (median 3.4 days; IQR 2-6.1 days) (P < .001).
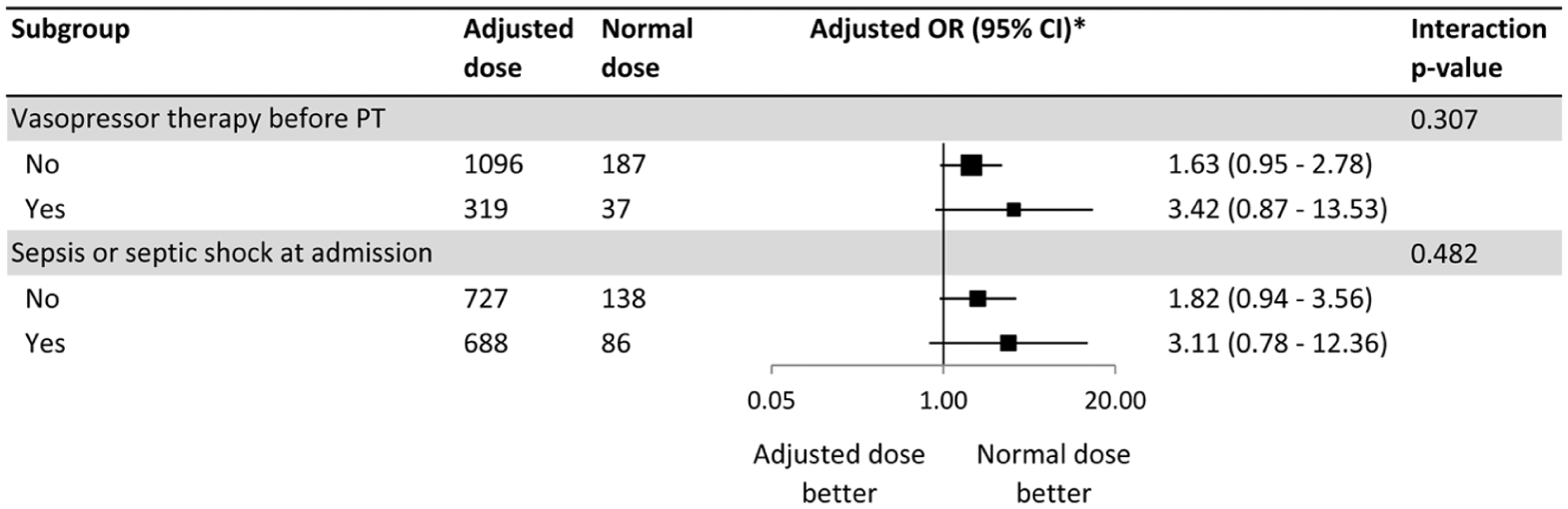
Subgroup analyses of the primary outcome (ICU mortality at 28 days).
Discussion
In this analysis of a large multicenter dataset of adult critically ill patients, our findings demonstrate that early dose adjustment of PT in AKI is a common practice that is independently associated with an increased risk of 28-day ICU mortality. This association was consistent across predefined subgroups. It was also demonstrated in the sensitivity analyses but did not reach statistical significance when the CKD-EPI equation was used for calculating pretreatment eGFR. Overall, our findings are consistent with the KDIGO recommendation to avoid early dose adjustment of beta-lactams in critically ill patients with AKI.
Our findings are consistent with a prospective observational study that reported an independent association of early dose adjustment of antipseudomonal beta-lactams with an increased risk of in-hospital mortality among 224 adult critically ill patients with sepsis and AKI. 5 However, this study was limited by its small sample size and the use of time to hospital mortality as the primary outcome, which may not be the most clinically relevant endpoint in critically ill patients. 14 In addition, in-hospital mortality may be affected by factors other than initial dosing of antimicrobials. In our study, we used a large database of ICU patients and defined 28-day ICU mortality as the primary outcome. We did not restrict our primary analysis to patients diagnosed with sepsis or septic shock to maintain statistical power, but we conducted a subgroup analysis that demonstrated a consistent association irrespective of the initial diagnosis of sepsis or septic shock.
Another multicenter retrospective cohort study compared low-dose PT (48-hour cumulative dose <27 g) and normal-dose PT (≥27 g) in 608 propensity score-matched septic shock patients. 15 Compared with the low-dose group, the normal-dose group had more median norepinephrine-free days and lower rates of in-hospital mortality or hospice disposition. This study was not restricted to patients with renal dysfunction and did not differentiate between AKI and CKD. Therefore, its findings do not directly address the question of early dose adjustment in AKI.
In contrast, there was no significant difference in hospital mortality, vasopressor-free days, or ventilator-free days with renal dose adjustment of antipseudomonal beta-lactams in a retrospective study of 173 adult patients with septic shock secondary to Gram-negative bacteremia and AKI. 4 Similarly, another retrospective study of patients with Gram-negative bacteremia and AKI not requiring renal replacement therapy reported no significant difference in clinical recovery between adjusted doses [8/11 (72.7%)] and normal doses [73/86 (84.9%)] of beta-lactams. 3 The divergent findings observed in our study may be attributed to our larger sample size, different study populations, the use of 28-day ICU mortality as the primary outcome, and adjustment for pretreatment renal function.
The findings of our study may be explained in the context of pharmacokinetic/pharmacodynamic (PK/PD) target attainment. The antimicrobial activity of PT depends on % fT > MIC. In critically ill patients, targets ranging from 100% fT > MIC up to 100% fT > 2-5 × MIC have been associated with improved clinical outcomes. 2 While evidence on the impact of early PK/PD target nonattainment on clinical outcomes in critically ill patients remains mixed,16-18 our observation that early dose adjustment in AKI patients is associated with increased mortality may, in part, reflect lower drug exposure during the initial 24 hours of therapy.
In our study, patients who received a normal dose of PT in the first 24 hours had a longer time to ICU discharge. This finding may reflect survivorship bias in this outcome, as the analysis of ICU stay was restricted to patients who were discharged alive, and mortality was lower in the normal-dose group. The most severely ill patients—who otherwise may have died—likely required longer ICU stay for recovery. Nonetheless, alternative explanations of this finding such as differences in recovery trajectory or adverse effects cannot be excluded and warrant further investigation in future studies.
This study demonstrates an association between the administration of normal maintenance doses of PT for at least the first 24 hours of therapy (≥13.5 g/24 h) and survival in critically ill patients with AKI. A 24-hour timeframe was chosen because many patients recover from AKI, die, or have their antibiotic changed thereafter. Restricting the analysis to those continuing PT without such deviations would have markedly reduced the sample size, limiting conclusions about initial dosing effects. However, the optimal time for dose adjustment in patients with persistent renal dysfunction remains uncertain, and the decision to extend the duration of normal dosing should consider the risk of drug accumulation and adverse effects. Prospective studies that use TDM are needed to evaluate the appropriate approach for subsequent dose adjustment.
To our knowledge, this is the largest study to evaluate the clinical outcomes of adjusting the dose of beta-lactam antibiotics in critical illness and AKI. In addition, the data were collected from many hospitals across the United States, thereby reflecting diverse clinical practices and patient populations. Nonetheless, several limitations warrant consideration. The administered PT doses were not directly recorded in the eICU-CRD but calculated from PT orders, which may have introduced inaccuracies. Renal function was estimated using MDRD and CKD-EPI equations because they do not require weight input, although they are suboptimal in this setting. The use of alternative equations was not feasible due to missing weight and preadmission creatinine values. Inclusion of patients in the analysis based on pretreatment CKD-EPI eGFR resulted in loss of statistical significance, indicating that the results may be sensitive to the pretreatment eGFR calculation method, which warrants consideration in future studies.
The retrospective nature of the study also entails inherent limitations, including imbalance in study group sizes, potential residual confounding, and absence of data about infusion times, sources of infection, and microbiological results. Furthermore, subsequent dosing beyond the first 24 hours was not evaluated, because our study hypothesis focused on initial therapy. Although outcomes of critically ill patients are more linked to the appropriateness of initial antimicrobial therapy, 19 dose adjustments occurring after the initial 24 hours may have influenced outcomes. Finally, generalizability may be limited to ICUs with similar patient populations and clinical practices. Given the relatively low mortality of patients in the eICU-CRD, 12 the administration of normal maintenance doses may have a greater survival benefit in critically ill patients with AKI and higher baseline risk of mortality.
Conclusion and Relevance
In this study, most critically ill patients with AKI received adjusted doses of PT (<13.5 g) during the first 24 hours of therapy. Early dose adjustment was independently associated with increased ICU mortality at 28 days. These findings suggest that renal dose adjustment of PT should be deferred beyond the first 24 hours of therapy in critically ill patients with AKI. Prospective studies are warranted to confirm these findings, evaluate the safety of administering normal doses of beta-lactams in AKI, and determine the appropriate approach for subsequent dose adjustments.
Supplemental Material
sj-docx-1-aop-10.1177_10600280261452547 – Supplemental material for Impact of Early Dose Adjustment of Piperacillin/Tazobactam on Mortality in Critically Ill Patients With Acute Kidney Injury: A Retrospective Multicenter Cohort Study
Supplemental material, sj-docx-1-aop-10.1177_10600280261452547 for Impact of Early Dose Adjustment of Piperacillin/Tazobactam on Mortality in Critically Ill Patients With Acute Kidney Injury: A Retrospective Multicenter Cohort Study by Mohamed Omar Saad, Mohd Hafiz Abdul-Aziz, Ousama Rachid and Mohamed Izham Mohamed Ibrahim in Annals of Pharmacotherapy
Footnotes
Ethical Considerations
The study is exempt from institutional review board approval due to its retrospective design, lack of direct patient intervention, and the security schema for which the reidentification risk was certified as meeting safe harbor standards by an independent privacy expert (Privacert, Cambridge, MA) (Health Insurance Portability and Accountability Act Certification No. 1031219-2).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.