
Abstract
Background:
Poly (ADP-ribose) polymerase inhibitors (PARPis) are commonly used as maintenance therapy following first-line chemotherapy for ovarian cancer and are associated with myelosuppression during treatment. However, there is limited guidance on the potential impact of prior PARPi exposure on the tolerance of subsequent chemotherapy.
Objective:
The purpose of this study was to evaluate the association between prior PARPi maintenance therapy and myelosuppression during second-line chemotherapy for ovarian cancer.
Methods:
A retrospective, single-center, cohort study was conducted of adult women with ovarian cancer who received second-line chemotherapy between January 2017 and June 2024 at a community-teaching hospital. Patients receiving PARPi maintenance following first-line therapy were compared with those who did not receive maintenance. The primary outcome was neutropenia (absolute neutrophil count [ANC] <1500 cells/µL) during second-line chemotherapy. Secondary outcomes included severe neutropenia, anemia, thrombocytopenia, chemotherapy delay, and use of granulocyte colony-stimulating factors (G-CSFs) during second-line chemotherapy.
Results:
Forty-two patients were included; 11 received prior PARPi maintenance and 31 did not. Neutropenia occurred more frequently in the PARPi-exposed group compared with the non-PARPi group (91% vs 52%, odds ratio [OR] = 9.35, 95% CI = 1.07-83.3, P = .030), with effect estimates remaining large and directionally consistent on multivariable analysis adjusting for baseline ANC (OR = 6.36) and propensity score (OR = 6.10). Median nadir ANC was significantly lower with the PARPi-exposed group (1004 vs 1380 cells/µL, P = .019), and secondary G‑CSF prophylaxis was more frequently utilized (73% vs 23%, P = .008). No patients received erythropoiesis-stimulating agents. Limitations included the retrospective design, small sample size, single-center setting, and heterogeneity in second-line chemotherapy regimens.
Conclusion and Relevance:
This exploratory, hypothesis-generating study suggests prior PARPi maintenance may increase the risk of neutropenia and the need for G-CSF use during subsequent chemotherapy. These findings highlight the need for heightened monitoring and supportive care consideration in this population and warrant validation in larger studies.
Introduction
Myelosuppression is a common and expected adverse effect of chemotherapy, and a degree of hematopoietic suppression is considered an acceptable consequence of treatment; however, even moderate myelosuppression may necessitate treatment delays and can adversely impact quality of life through anemia-related fatigue. Severe cases of myelosuppression may be life-threatening due to the risk for febrile neutropenia or bleeding in the setting of severe thrombocytopenia. Given the potentially serious consequences of febrile neutropenia, National Comprehensive Cancer Network (NCCN) guidelines recommend granulocyte colony-stimulating factors (G-CSFs) in all individuals receiving a regimen with a high risk of febrile neutropenia (>20%) and in those with additional risk factors receiving a regimen with an intermediate risk (10%-20%). 1 Established patient-specific risk factors include prior chemotherapy or radiation, persistent neutropenia, tumor involvement of the bone marrow, recent surgery, open wounds, organ dysfunction, and advanced age (>65 years). 1
In the treatment of ovarian cancer, neutropenia occurs in upwards of 50% of patients receiving chemotherapy, and febrile neutropenia occurs in approximately 7%.2,3 These rates are consistent with the myelosuppressive regimens commonly used in this disease, which typically include a platinum agent combined with a taxane as first-line therapy, followed by agents such as liposomal doxorubicin, taxanes, or gemcitabine with or without a platinum agent in the recurrent setting. 4 In addition, maintenance therapy with poly(ADP-ribose) polymerase inhibitors (PARPis) following primary chemotherapy has become a standard component of ovarian cancer management. 4
Poly-ADP ribose polymerase (PARP) enzymes play a critical role in the repair of single-strand DNA breaks through the base excision repair pathway. 5 Inhibition of PARP results in the accumulation of DNA damage and subsequent cell death, an effect that is particularly pronounced in tumor cells with deficiencies in the homologous recombination repair pathway, such as those with BReast CAncer gene (BRCA) mutations. 5 The PARPi utilized in the maintenance setting after primary chemotherapy for ovarian cancer (niraparib, olaparib, and rucaparib) have demonstrated an improvement in progression-free survival among patients with International Federation of Obstetrics and Gynecology (FIGO) stage III and IV disease who achieve a complete or partial response to first-line platinum-based chemotherapy.4,6 An established adverse effect of PARPi is myelosuppression, including anemia in 37% to 50% of patients, neutropenia in 18% to 30% of patients, and thrombocytopenia in 14% to 61% of patients. 7 These hematologic toxicities usually occur within the first 3 months of therapy and are generally managed with treatment interruption and dose reduction.7,8 In the phase 3 SOLO2 trial of olaparib maintenance, the median time to resolution of neutropenia in patients experiencing this adverse effect was 29 days. 9
Although myelosuppression often improves after discontinuation of PARPi therapy, as demonstrated in the SOLO2 trial, emerging evidence suggests the potential for long-term effects on the bone marrow. The PARPi use has been associated with an increased risk of treatment-related myeloid neoplasms, including myelodysplastic syndrome and acute myeloid leukemia, potentially related to impaired DNA repair and alterations in clonal hematopoiesis (CH).7,10,11 While prior chemotherapy is an established risk factor for neutropenia in patients receiving additional cytotoxic therapy, it remains unknown whether PARPi exposure contributes to impaired marrow reserve, thereby impacting post-PARPi chemotherapy tolerance. The objective of the current exploratory study was to address this gap by examining the association between prior PARPi exposure and the incidence of myelosuppression in patients with ovarian cancer receiving subsequent chemotherapy, including assessment of whether this association persists after adjustment for key baseline characteristics.
Methods
Study Design
This hypothesis-generating study was a retrospective review of electronic health records from a community-teaching hospital in the Midwestern United States. The cohort consisted of all females treated at the institution, 18 years old or older, who initiated second-line chemotherapy for the treatment of ovarian cancer between January 1, 2017, and June 30, 2024. Second-line therapy was defined as the first systemic chemotherapy regimen initiated following completion or discontinuation of first-line therapy. Patients were excluded if they had any additional concomitant or prior cancer diagnosis, underlying bone marrow disorder, or neutropenia immediately prior to starting second-line chemotherapy. Data were collected from the time of second-line chemotherapy regimen initiation and stopped either upon discontinuation of the second-line regimen or on the data cutoff date of November 1, 2024, if therapy continued past this date. Patients receiving a PARPi as maintenance after first-line therapy were compared to patients not receiving maintenance. Included patients receiving PARPi maintenance had PARPi discontinued prior to initiation of second-line chemotherapy. The local Institutional Review Board reviewed/approved the study and determined it was exempt/limited from Institutional Review Board (IRB) review as defined in 45 CFR 46.101(b).
The primary endpoint of the study was the incidence of neutropenia (absolute neutrophil count [ANC] <1500 cells/μL) during second-line chemotherapy. Secondary endpoints included the incidence of severe neutropenia (ANC <500 cells/μL), anemia (hemoglobin [Hgb] <10 g/dL), thrombocytopenia (<100 000 platelets/μL), febrile neutropenia (occurrence of ANC <1000 cells/μL and a single temperature >38 °C), and delay in therapy due to hematologic toxicity during second-line chemotherapy. The use of G-CSF and erythropoietin-stimulating agents (ESAs) during second-line chemotherapy was also compared between groups to identify the potential impact on myelosuppression risk mitigation strategies.
Data Collection
Baseline data collected from the electronic health records included receipt of PARPi and agent, second-line chemotherapy regimen, age, weight, Eastern Cooperative Oncology Group Performance Status (ECOG PS), the presence of BRCA mutations, homologous repair deficiency (HRD) status, and first-line chemotherapy regimen. In addition, established risk factors for febrile neutropenia were collected, including receipt of prior radiation, presence of an open wound, tumor bone marrow involvement, and surgery within 30 days of starting second-line chemotherapy. Baseline laboratory data collected included ANC, Hgb, platelet, bilirubin, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) within 1 week of starting second-line chemotherapy.
Data collected for study outcomes included nadir ANC, Hgb, and platelet count during second-line chemotherapy. In addition, the occurrence of febrile neutropenia and dose delay due to myelosuppression during second-line chemotherapy was collected. The use of G-CSF and ESA agents during second-line chemotherapy was collected and categorized as primary prophylaxis (starting with the initiation of second-line chemotherapy) or secondary prophylaxis (starting with cycle 2 or beyond of second-line chemotherapy). All laboratory measurements were performed at the local laboratory, an accredited institutional laboratory operating within the same center where the study was conducted, ensuring consistency of results across all participants.
Statistical Analysis
Data were compared between those receiving PARPi maintenance after first-line chemotherapy and those not receiving maintenance PARPi. Categorical data were analyzed using a chi-square or Fisher’s exact test (as appropriate based on cell frequency). Continuous data were compared using the Mann-Whitney U-test (nonparametric data) or Student’s t-test (parametric data), and ordinal data were compared using the Mann-Whitney U-test. Odds ratios (OR), median difference, mean difference, and 95% confidence intervals (CI) were calculated as measures of association between PARPi exposure and outcomes. To assess the potential impact of confounding on the primary endpoint (neutropenia), 2 multivariable binary logistic regressions were utilized. The first model included baseline ANC as a single covariate. As a sensitivity analysis, a propensity score incorporating age, primary G-CSF prophylaxis use, baseline ANC, and regimen type (platinum-containing or non-platinum-containing regimen) was included as a covariate in a second separate model. Data were censored as of November 1, 2024, if patients continued second-line chemotherapy past this date. Each endpoint was analyzed as cumulative incidence at the patient level (≥1 event during second-line therapy). Recurrent episodes were not modeled separately. Missing data was not imputed. All analyses were conducted on a complete case basis, including only those with available data for each respective outcome or variable. All statistical tests were conducted with IBM SPSS Statistics version 29 (IBM Corp, Armonk, New York) software.
Results
Fifty women were identified as meeting inclusion criteria, and after exclusion of 8 who had a prior or concomitant cancer diagnosis other than ovarian cancer, a total of 42 were included, with 1 patient censored as of the data cutoff date of November 1, 2024. Eleven women (26%) received PARPi maintenance prior to second-line chemotherapy, and 31 (74%) did not receive PARPi maintenance. In total, 2 patients received rucaparib and 9 received niraparib for a mean duration of PARPi maintenance of 7.3 months (standard deviation 6.5 months). Reasons for discontinuation of PARPi maintenance were disease progression in 9 (82%) patients, cytopenia in 1 (9%) patient, and non-hematologic adverse effect in 1 (9%) patient. The median time lapsing between discontinuation of PARPi maintenance and second-line chemotherapy was 4.9 weeks (interquartile range: 4.71 weeks). In the group of women who did not receive PARPi maintenance, 7 (23%) received bevacizumab maintenance after first-line chemotherapy. Included women had a mean age of 64 years, a median ECOG PS of 1, and the median duration of second-line chemotherapy was 20 weeks. Overall baseline characteristics were similar between those receiving PARPi maintenance and those not receiving PARPi maintenance (Table 1). A statistically significant difference was present between groups in mean ANC prior to starting second-line chemotherapy, which was 3333 cells/μL (standard deviation [SD] 1068 cells/μL) in those receiving PARPi maintenance compared to 4608 cells/μL (SD 1651 cells/μL) in women not receiving PARPi maintenance (P = .022). Second-line chemotherapy regimens utilized were also similar between groups and included those with and without platinum agents and/or bevacizumab (Table 2). Given the number of regimens used and their varying degrees of myelosuppression, the regimens were further classified as platinum-containing or non-platinum-containing, and there remained no difference between groups.
Baseline Characteristics.
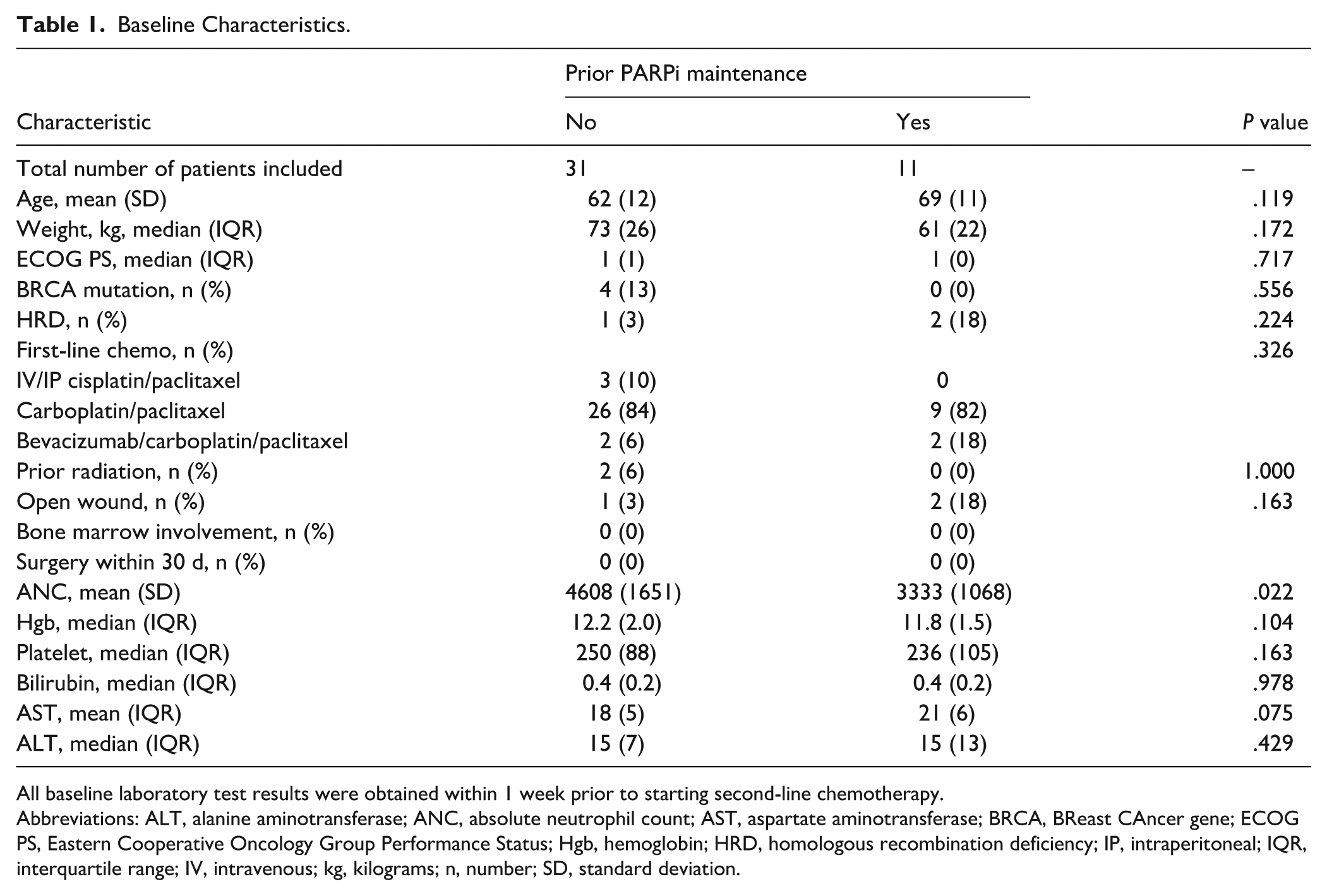
All baseline laboratory test results were obtained within 1 week prior to starting second-line chemotherapy.
Abbreviations: ALT, alanine aminotransferase; ANC, absolute neutrophil count; AST, aspartate aminotransferase; BRCA, BReast CAncer gene; ECOG PS, Eastern Cooperative Oncology Group Performance Status; Hgb, hemoglobin; HRD, homologous recombination deficiency; IP, intraperitoneal; IQR, interquartile range; IV, intravenous; kg, kilograms; n, number; SD, standard deviation.
Characteristics of Second-Line Chemotherapy Regimen.
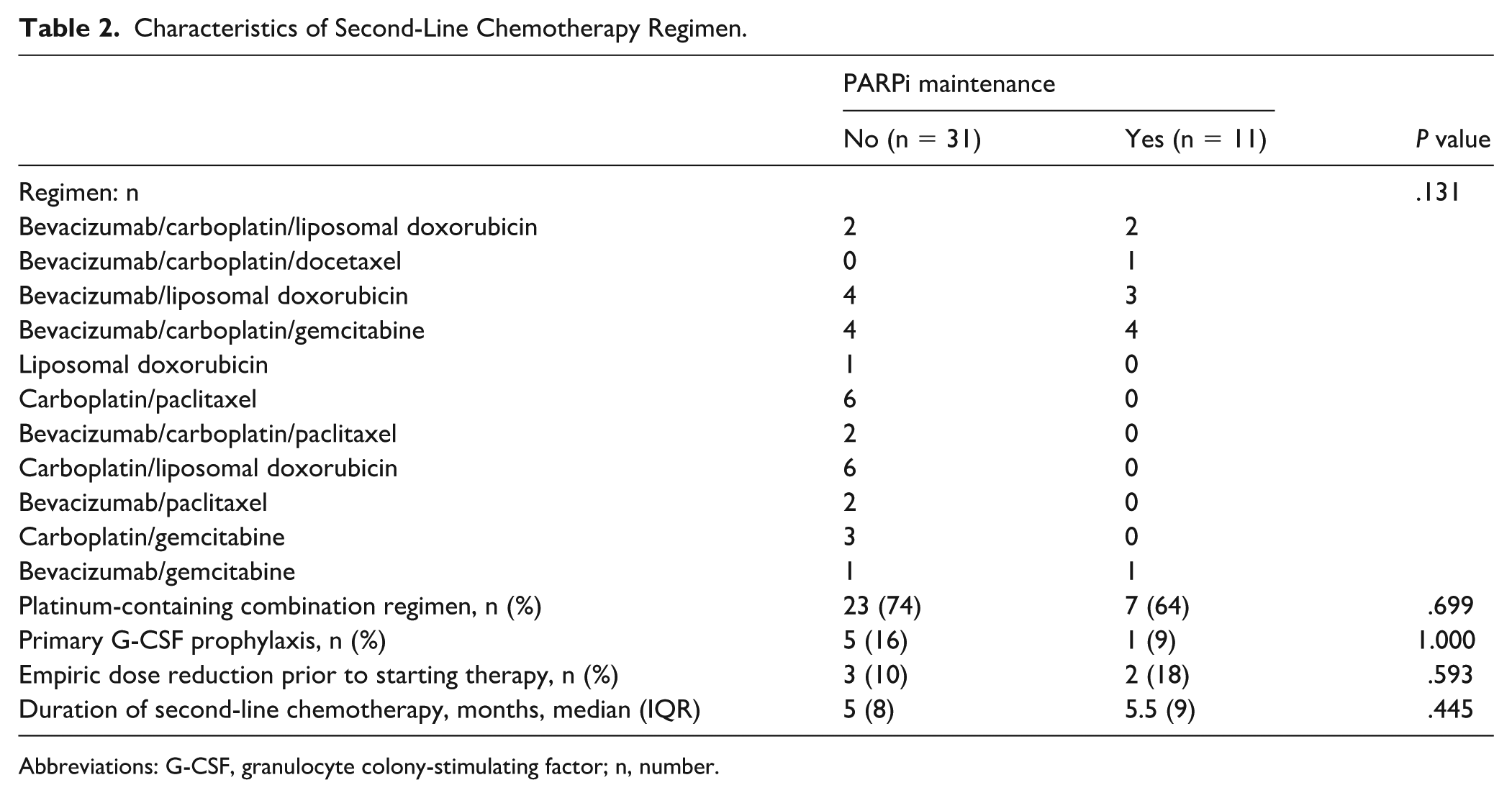
Abbreviations: G-CSF, granulocyte colony-stimulating factor; n, number.
The primary endpoint of neutropenia (ANC <1500 cells/μL) occurred more often in the group receiving PARPi maintenance (91% vs 52%, respectively, OR = 9.35, 95% CI = 1.07-83.33, P = .030). Upon multivariable binary logistic regression, the OR (95% CI) when including baseline ANC as a covariate was 6.36 (0.68-58.8) and was 6.10 (0.64-58.8) when the propensity score was included as a covariate (Table 3). Severe neutropenia occurred more commonly in those receiving PARPi maintenance (27% vs 6%, respectively, OR = 5.43, 95% CI = 0.77-38.46, P = .103); however, the difference did not reach statistical significance. The incidence of anemia (73% vs 52%, respectively, OR = 2.50, 95% CI = 0.56-11.24, P = .299) and thrombocytopenia (45% vs 39%, respectively, OR = 1.32, 95% CI = 0.33-5.29, P = .733) were non-significantly higher with PARPi maintenance.
Primary Endpoint – Neutropenia (ANC <1500).
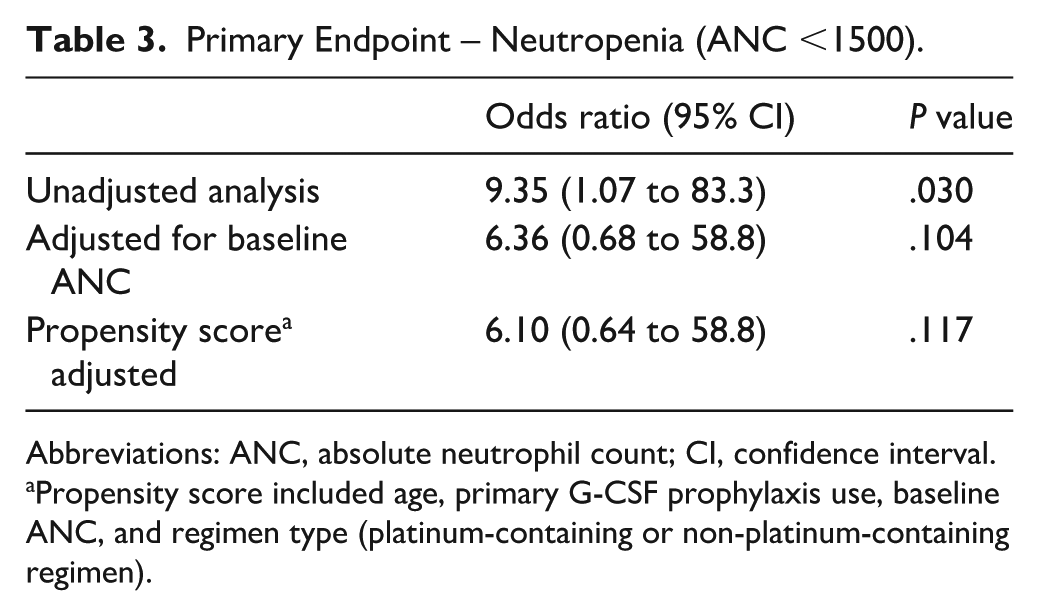
Abbreviations: ANC, absolute neutrophil count; CI, confidence interval.
Propensity score included age, primary G-CSF prophylaxis use, baseline ANC, and regimen type (platinum-containing or non-platinum-containing regimen).
Similarly, there were no significant differences in the incidence of dose delays due to myelosuppression (36% vs. 19%, OR: 2.38, 95% CI: 0.52-10.87, P = .410), despite occurring more frequently in the PARPi maintenance group. There was a statistically significant difference between groups in nadir ANC during second-line chemotherapy; however, there was not a significant difference in nadir Hgb or platelets (Table 4). Finally, the use of secondary G-CSF prophylaxis was significantly more common in patients receiving PARPi maintenance (Table 4). None of the women included received ESAs during second-line chemotherapy.
Secondary Endpoints.
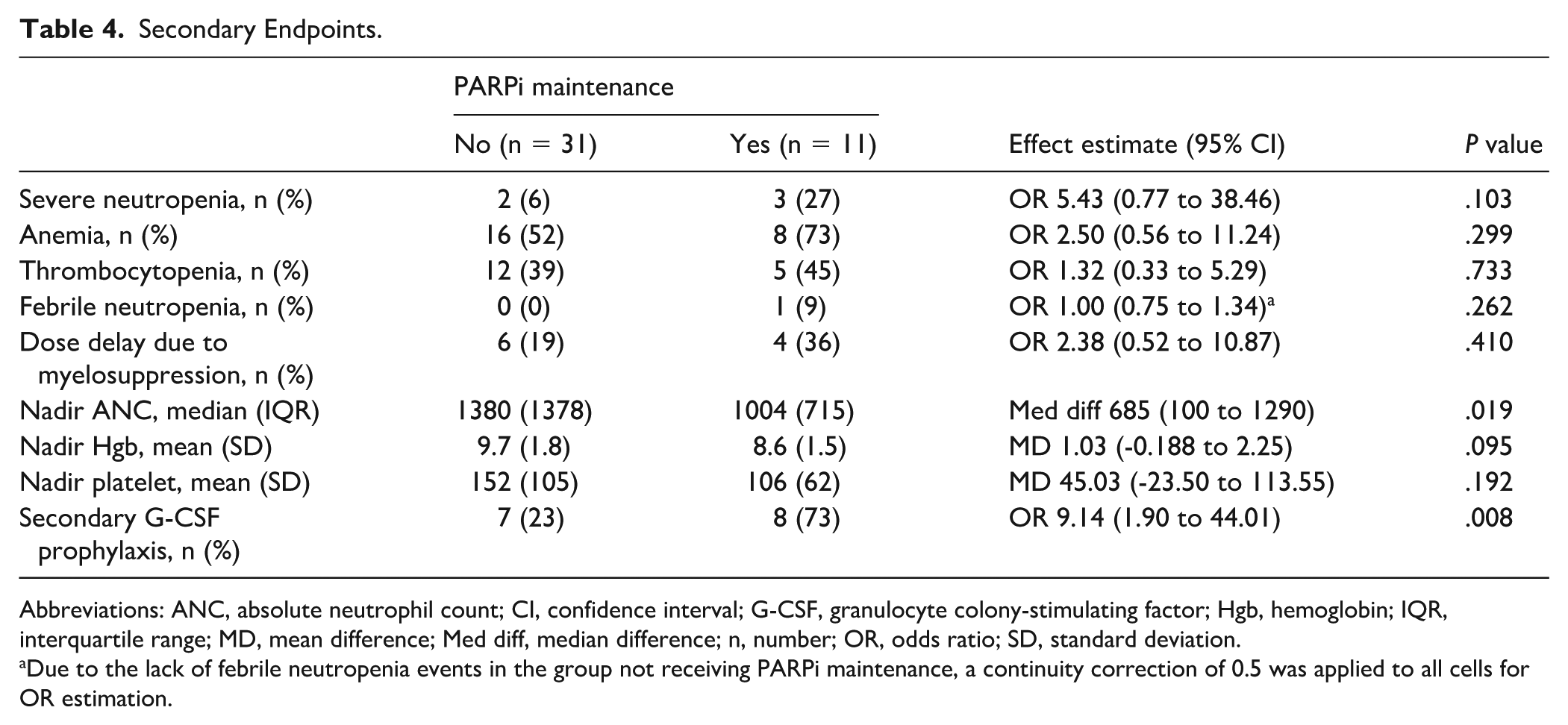
Abbreviations: ANC, absolute neutrophil count; CI, confidence interval; G-CSF, granulocyte colony-stimulating factor; Hgb, hemoglobin; IQR, interquartile range; MD, mean difference; Med diff, median difference; n, number; OR, odds ratio; SD, standard deviation.
Due to the lack of febrile neutropenia events in the group not receiving PARPi maintenance, a continuity correction of 0.5 was applied to all cells for OR estimation.
Discussion
In this single-center retrospective cohort study, neutropenia during second-line chemotherapy for ovarian cancer was observed more frequently in patients with prior PARPi maintenance exposure, who also demonstrated a lower nadir ANC and more frequent use of secondary G-CSF prophylaxis, which may reflect both greater myelosuppressive burden and heightened clinical vigilance in this population. These observations may have been influenced by the lower baseline ANC in the PARPi-exposed group; after adjustment for baseline ANC, the odds of neutropenia remained elevated but did not retain statistical significance, a finding that may reflect the limited power of the adjusted model given the sample size. Despite not reaching statistical significance, those receiving PARPi maintenance had higher rates of severe neutropenia, anemia, thrombocytopenia, and chemotherapy delays. While prior studies have focused on the risk of myelosuppression during PARPi therapy and therapy-related myeloid malignancies, little attention has been directed toward the possibility of more subtle or intermediate impairments in bone marrow reserve that may influence tolerance of subsequent chemotherapy. The findings of this study suggest that prior PARPi exposure may influence the hematologic toxicity profile of subsequent treatment and may increase risk for myelosuppression during future chemotherapy regimens. However, this analysis was designed as an exploratory, hypothesis-generating evaluation rather than a confirmatory assessment, and findings should be interpreted accordingly.
Potentially consistent with the known myelosuppressive effects of PARPi, a significant difference in baseline ANC was observed between patients with and without PARPi maintenance, which may reflect either a residual effect of prior PARPi exposure or baseline differences in marrow reserve.7,8 The unadjusted OR for neutropenia of 9.35 was attenuated to 6.36 after adjustment for baseline ANC and to 6.10 in the propensity score model. While this attenuation suggests that baseline ANC partially accounts for the association, the adjusted effect estimates remain large and consistent in direction, and the loss of significance may reflect reduced power in the adjusted model, given the small sample size rather than an absence of a true effect.
Furthermore, the lower baseline ANC in the PARPi-exposed group may itself reflect a persistent effect of PARPi on bone marrow reserve following treatment discontinuation. If baseline ANC represents an intermediate step in the pathway between prior PARPi exposure and subsequent myelosuppression rather than an independent confounding variable, adjustment for it could potentially underestimate the total effect of prior PARPi exposure. While this distinction cannot be resolved in this retrospective analysis, it warrants consideration when interpreting the adjusted analyses.
To our knowledge, this is the first investigation into myelosuppression risk in patients receiving second-line chemotherapy post-PARPi maintenance, and the mechanism remains speculative. Nevertheless, plausible mechanisms for a lingering impact of prior PARPi on hematologic tolerance are largely based on the cytotoxic mechanism of PARPi and some emerging evidence of their impact on CH. Poly-ADP ribose polymerase enzymes play a central role in DNA repair, and inhibition results in the accumulation of DNA damage. 12 Although the myelosuppression induced by this DNA damage during PARPi therapy is reversible, some effects of the damage may persist. The possible persistence of DNA damage may have resulted in the lower baseline ANC among those receiving prior PARPi in this study and may have increased the risk for myelosuppression upon initiation of second-line chemotherapy. Furthermore, PARPi’s possible association with an elevated risk for therapy-related myeloid neoplasms may be due to accumulated and persistent DNA damage. In fact, PARPi has been linked to DNA damage response-driven CH. 10 Clonal hematopoiesis is due to somatic mutations in hematopoietic stem cells, resulting in a clonal population.10,13 Interestingly, in an analysis of CH in the ADjuVANt Chemotherapy in Elderly (ADVANCE) breast cancer trial, the presence of CH was associated with an increase in any grade neutropenia (67% CH present vs 58% CH absent) and a significant increased risk for cyclophosphamide doses being held or reduced (64% CH present vs 0% CH absent, P = .02). 13 Although the analysis of breast cancer patients was relatively small (n = 40), the identified risks of CH were similar to those of prior PARPi, where we identified an increased risk for neutropenia and almost doubling of the incidence of dose delay. These similarities, taken together with the potential increased risk of therapy-related myeloid neoplasms, suggest that CH associated with PARPi therapy may play a role in the increased risk of myelosuppression in those previously exposed to PARPi. Importantly, should CH represent a contributing mechanism in this context, it may also offer an additional potential explanation for the lower baseline ANC observed in the PARPi-exposed group, possibly reflecting an underlying reduction in hematopoietic reserve prior to the initiation of second-line chemotherapy. While our study did not evaluate CH directly, these observations are consistent with a pathway whereby PARPi-related DNA damage responses could influence subsequent hematologic tolerance.
The inclusion of patients undergoing a homogenous treatment sequence represents an important strength of our study. All patients received second-line chemotherapy following first-line platinum-based treatment, ensuring that differences in hematologic toxicity were not attributable to varying degrees of cumulative prior chemotherapy exposure. This must be taken into consideration with the limitations of the study including the retrospective design and limited sample size. The small sample size, particularly in the PARPi-exposed group, may have reduced statistical power to detect differences in several of the clinically relevant secondary outcomes that demonstrated a numeric, yet statistically insignificant, increased risk of myelosuppression with post-PARPi second-line chemotherapy. Additionally, the small sample size increases the risk for spurious findings, and results should be interpreted with caution pending evaluation in adequately powered studies in the future. Likewise, therapy may have been impacted by factors not considered (disease biology, prescriber decision-making, changes in care over time, etc), and while baseline characteristics were broadly similar, residual confounding cannot be ruled out. Finally, although the study population was homogenous with respect to the number of prior lines of therapy, variation in the specific regimens utilized in the second-line setting may influence the degree of myelosuppression observed. In an attempt to address the impact of chemotherapy regimen on myelosuppression, we classified the type of regimen received as platinum or non-platinum-containing; groups were similar with respect to regimen type. Regimen type was further incorporated into the propensity score utilized in the multivariable binary logistic regression model. Nevertheless, given the potential influence of specific regimen on myelosuppression, the second-line chemotherapy regimen should be more comprehensively controlled for in future prospective studies.
Conclusion and Relevance
The present study provides preliminary, hypothesis-generating evidence suggesting PARPi exposure may influence tolerance of subsequent chemotherapy in patients with ovarian cancer, specifically increasing risk for neutropenia and greater G-CSF use. As the use of PARPi has expanded in multiple malignancies, more patients will be exposed to these agents prior to chemotherapy. Understanding the impact of prior PARPi use on the hematologic toxicity profile of subsequent chemotherapy is therefore of increasing clinical importance. These findings are particularly relevant given that the primary benefit of PARPi maintenance is improvement of progression-free survival, where toxicity and the potential for increased hematologic toxicity with future therapy may represent an additional consideration, if confirmed, in the overall clinical management of patients for whom PARPi therapy is being discussed. 6 Larger studies that control for second-line chemotherapy regimen are needed to confirm these findings and to further characterize the magnitude of effect. Such data would clarify whether prior PARPi exposure should be integrated into formal risk stratification for chemotherapy‑induced myelosuppression. In the absence of additional data, practitioners should consider the potential for increased myelosuppression with subsequent chemotherapy after PARPi therapy and institute monitoring and mitigation strategies, as appropriate.
Footnotes
Ethical Considerations
The local Institutional Review Board (Franciscan Health IRB) reviewed/approved (approval 2247182-1) the study and determined it was “exempt/limited from IRB review as defined in 45 CFR 46.101(b).”
Author Contributions
Project concept and design (EHC, DJR), acquisition of the data (EHC), analysis and interpretation of the data (EHC, DJR), drafting of the manuscript (EHC), critical revision of the manuscript for important intellectual content (DJR), approval of the version to be published (EHC, DJR), and agreeing to be accountable and willing to investigate and resolve all questions pertaining to accuracy and/or integrity of the work (EHC, DJR).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on request.