
Abstract
Glomus tumor is a rare mesenchymal neoplasm originating from the modified smooth muscle cells of the glomus body. Primary colonic glomus tumor is extremely rare with only 5 cases published in the English literature. In this article, we report the sixth case of primary colonic glomus tumor in a 50-year-old female with no significant past medical history who presented with routine screening colonoscopy. The entire colon was endoscopically unremarkable except an incidental 6-mm sessile polyp located in the descending colon. Biopsy showed a densely cellular neoplasm composed of small, bland, slightly spindled to predominantly epithelioid cells with clear to eosinophilic cytoplasm arranged in nests and sheets. The tumor cells were interspersed with slit-like thin-walled vessels and scattered short nerve bundles. Immunohistochemically, the tumor cells were positive for smooth muscle actin, h-caldesmon, and CD34 (focal), but completely negative for HMB45, S100, EMA, desmin, DOG-1, and CD117. The histologic features and immunohistochemical profile supported a diagnosis of primary colonic glomus tumor. The patient was asymptomatic and disease free after the procedure.
Background
Glomus tumor is a rare mesenchymal neoplasm representing <2% of all the soft tissue tumors. The comprehensive symptomatology and histology were first described by Barré and Masson in 1924. 1 The tumor is composed of 3 components: glomus cells, modified smooth muscle cells, and blood vessels, resembling normal perivascular glomus body that regulates temperature via arteriovenous shunting of blood. Depending on the proportion of each component, glomus tumor can be further subcategorized into solid glomus tumor, glomangioma, and glomangiomyoma. 2 It is most commonly found in the subungual region of the distal extremities, with a female predilection and age of onset at 30 years. 3 The classical triad of symptoms include intermittent excruciating pain, localized tenderness, and temperature hypersensitivity. Extradigital manifestations are rare, mostly involving the liver and gastrointestinal (GI) tract, particularly the stomach. 4 The colon is an extremely rare site for glomus tumor, with only 5 cases been reported so far in the literature.4-8 Herein, we describe a sixth case of primary colonic glomus tumor to recapitulate the importance of recognizing this rare benign entity in GI tract and utilizing immunostains for proper diagnosis. A brief review of all 6 colonic glomus tumors is performed to summarize its clinicopathologic features.
Case Summary
A healthy 50-year-old Indian-American female with no significant past medical history presented to a gastroenterologist for her first routine screening colonoscopy. She had no complains and was asymptomatic prior to arrival. During the procedure, she was found to have a 6-mm sessile polyp in the descending colon (Figure 1). The polyp was removed with cold snare and sent to pathology for histologic analysis (Figure 2). Hematoxylin and eosin–stained sections of the polyp revealed hypercellular tissue fragments consisting of small, uniform, slightly spindled but predominantly round to polygonal cells with clear to eosinophilic cytoplasm, centrally located nuclei, and indistinct cell borders. The cells were arranged in sheets and nests, interspersed with slit-like capillary-sized blood vessels, and short nerve bundles. No significant nuclear atypia or pleomorphism is identified. Among the tumor cells, only 2 mitotic figures were noted and none of them appeared atypical.

Endoscopic image of a polyp (6 mm) in the descending colon.
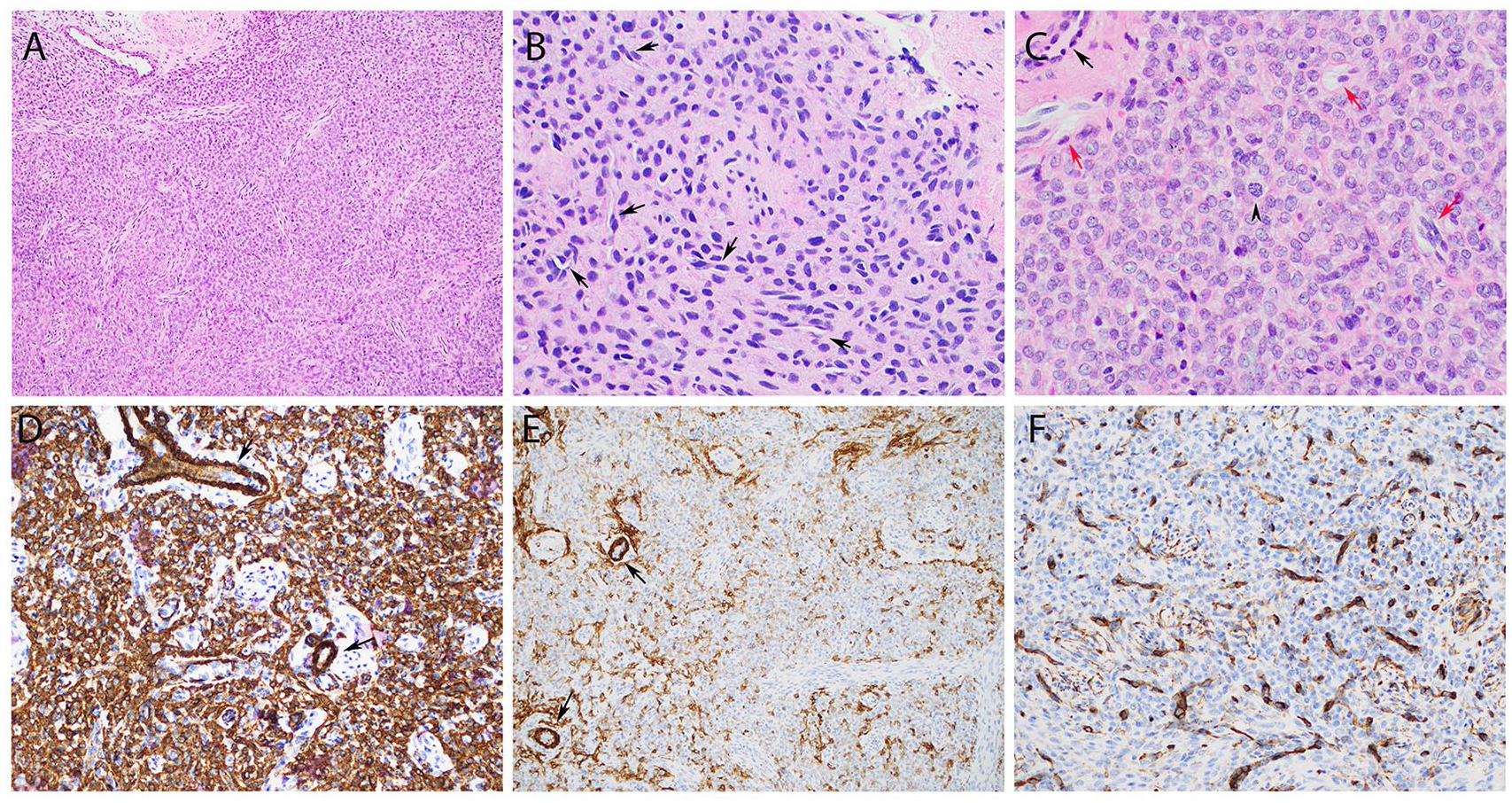
Histology and immunoprofile. (A) The tumor is solid and hypercellular with a small fragment of colonic muscularis mucosae attached (magnification: 100×). (B) The tumor cells are slightly spindled, irregularly dispersed, with indistinct cell borders. Scattered slit-like blood vessel rimed by a layer of hyperchromatic tumor cells is a characteristic feature (black arrows; magnification: 200×). (C) Another field showing round nuclei with rare intranuclear pseudo-inclusions and scattered short nerve bundles (red arrows) resembling a nerve sheath tumor. A rare mitotic figure (arrowhead) is present. A slightly dilated vessel surrounded by hyperchromatic tumor cells can be seen at the left upper field (black arrow; magnification: 400×). Immunohistochemistry shows tumor cells to be positive for SMA (strong and diffuse, D), h-caldesmon (patchy, E), and CD34 (focal, F). Arrows indicate tumor cells surrounding the vascular spaces (magnification: 200×).
Based on the histomorphology, a preliminary diagnosis of benign mesenchymal neoplasm was considered with a list of differential diagnosis including epithelioid nerve sheath tumor, epithelioid leiomyoma, GI stromal tumor (GIST), and glomus tumor. Immunohistochemical studies were performed with satisfactory controls and showed that the tumor cells were diffusely positive for smooth muscle actin, h-caldesmon (patchy), and CD34 (focal; Figure 2D-F), but negative for HMB45, S100, EMA, desmin, DOG-1, and CD117. Ki-67 mitotic index labeled ~2% of the tumor cells (data not shown). The overall findings are consistent with a benign glomus tumor, with solid growth pattern.
The patient remained asymptomatic after the procedure. She was doing well with no evidence of recurrence or metastatic disease during 3-month follow-up.
Discussion
Glomus tumor is a rare mesenchymal neoplasm arising from the modified smooth muscle cells around the Sucquet-Hoyer canal of the glomus body. It is commonly found in the subungual region of the extremities and often appears small, red-blue, solitary, and painful. GI tract glomus tumor is rare compared with its peripheral counterpart, with the stomach being the most common visceral organs involved by this tumor. The first case of primary colonic glomus tumor was published in 1988 by Barua describing an incidental glomus tumor found in the adventitia of a colon resected for colonic adenocarcinoma. 5 Since then, only 4 additional cases were reported.4,6-8 The clinical and histopathologic features of those cases, including the current one, are summarized in Table 1. As seen, for all 6 cases, the median age was 45 (range = 34-74) years. The tumor occurred in both males and females with no apparent sex predilection. The size of tumor ranged from <1.0 cm to 7.0 cm. Depending on the tumor size, patients were either asymptomatic or presented with nonspecific symptoms, such as abdominal pain, nausea, vomiting, or GI bleed. They were frequently an incidental finding on imaging studies or by colonoscopy. Rarely the tumor was too big (7.0 cm) and obstructing, causing symptoms. Histologically, most tumor cells were described as regular and cuboidal with distinct cell borders. Mitoses varied from rare to high (15 per 50 high-power field). One tumor demonstrated transmural growth extending to paracolic fat with vascular invasion. 7 However, follow-up revealed a benign clinical course and no recurrence or distant metastasis has been reported.
Clinicopathologic Features of 6 Primary Colonic Glomus Tumors.
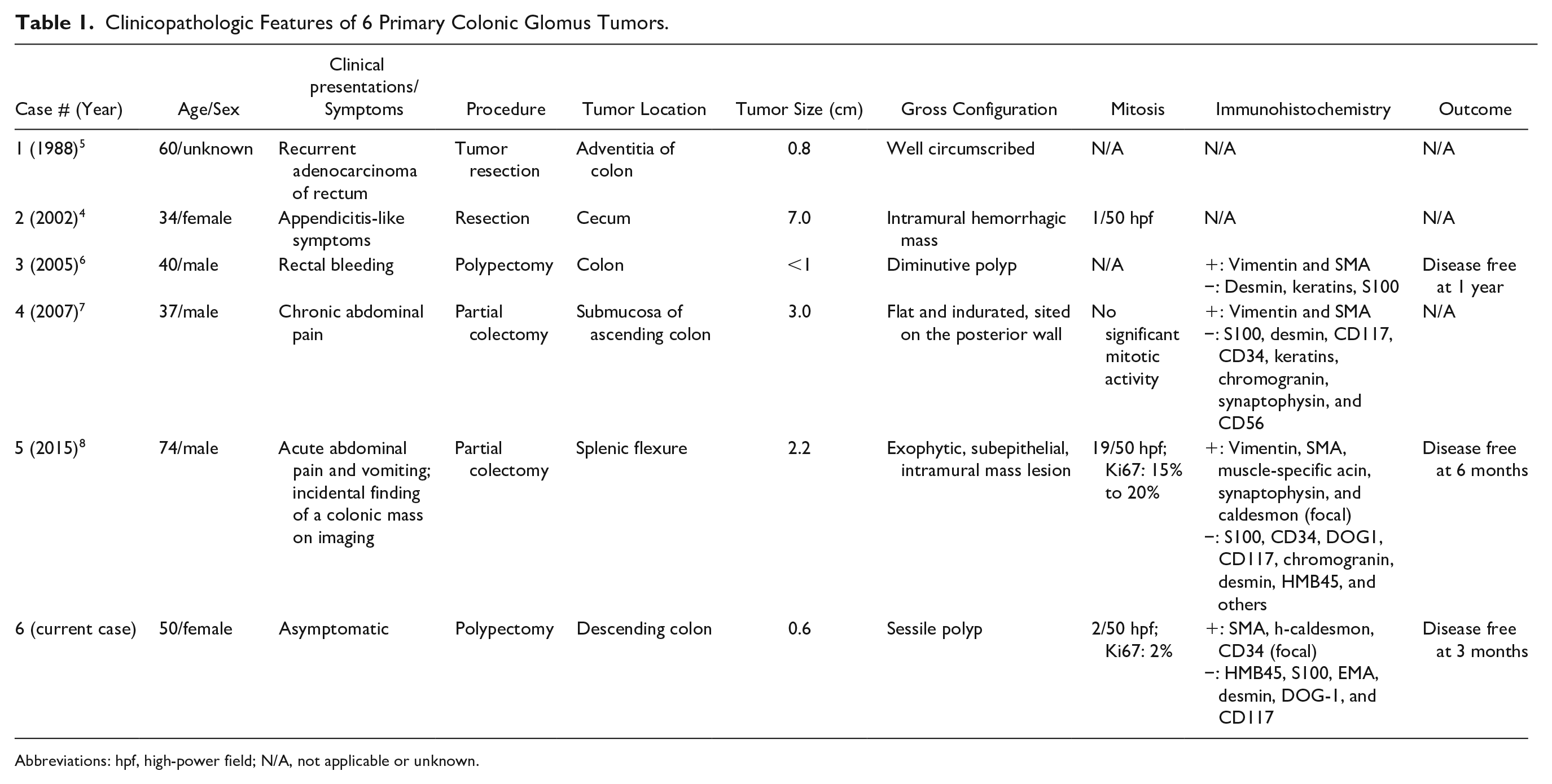
Abbreviations: hpf, high-power field; N/A, not applicable or unknown.
The World Health Organization classification of glomus tumor applies to both soft tissue tumor and digestive system, with 3 categories being proposed: benign, uncertain malignant potential, and malignant. 9 The diagnostic criteria are primarily based on a large series of 52 cases, where tumor size, location, atypical mitotic figures, mitosis count, and nuclear grade were systematically evaluated and correlated with prognosis. 10 With a deep location and size of >2 cm, plus any atypical mitotic figures and/or high nuclear grade, metastasis was observed in 38% of tumors fulfilling the criteria of malignancy. The category of uncertain malignant potential is reserved for those that do not fulfill all malignant criteria but show at least one atypical features. 10 Although high mitotic activity and nuclear atypia were associated with risk of metastasis in most cases, the malignant potential of the glomus tumors are not always predictable, as a tumor with low mitotic rate (1 per 50 high-power field) and mild nuclear atypia was found to metastasize to the liver and the patient died of disease at 50 months after surgery. 4 Of note, vascular invasion is not a prognostically adverse feature or diagnostic criteria for malignancy. 9
The diagnosis of the primary colonic glomus tumor relies on histology and immunohistochemical profile, similar to its soft tissue counterparts. Among the 3 histologic variants (solid, glomangioma, and glomangiomyoma), 2 the solid glomus tumor can mimic other mesenchymal tumors and pose great diagnostic challenges. Immunoprofiling is critical in this situation. Since GIST is the most common mesenchymal tumor in the GI tract, it should always be considered in differential diagnosis. However, GIST is typically positive for DOG-1 and CD117, while glomus tumor is negative for both. Epithelioid leiomyoma can resemble glomus tumor given diffuse positivity for smooth muscle actin; however, strong desmin expression in this tumor is a key. Epithelioid nerve sheath tumors are morphologically very similar to glomus tumor; however, those tumors are typically strongly positive for S100 and/or CD34. 11 Neuroendocrine tumor is another differential diagnosis, which are positive for cytokeratin and neuroendocrine markers such as synaptophysin and chromogranin. Yet a potential pitfall to keep in mind is that some glomus tumor, including a primary colonic glomus tumor, can stain positive for synaptophysin. 8
The pathogenesis of glomus tumors is still not clear. Multiple familial glomus tumors occur due to inactivating mutations in the glomulin gene. The most common mutation encountered is 157delAAGAA, which is seen in 48.8% of the affected families. 12 In contrast, sporadic glomus tumors are most likely associated with NOTCH family gene rearrangements or BRAF mutations. In 2013, Mosquera et al described NOTCH gene rearrangements in ~60% of benign and malignant glomus tumors, with NOTCH2-MIR143 fusion being the most common findings. 13 Chakrapani et al detected a small rate (10.7%) of BRAF V600E mutation in patients with sporadic glomus tumor. 14 Interestingly, another study found that 6% of glomus tumors harbored BRAF V600E mutation and all of which were previously classified as malignant glomus tumor or with uncertain malignant potential, suggesting that this mutation may be associated with malignant potential, and likely a target for future treatment. 15 Unlike GIST, GI tract glomus tumors are negative for CD117 and harbor no mutation in c-kit gene. 4
In summary, we present a rare case of primary colonic glomus tumor, adding to literature a total of 6 cases identified in this location. Although primary colonic glomus tumor is rare, it should be included in the differential diagnosis when dealing with mesenchymal tumors of the GI tract. Future studies focusing on the pathogenesis may necessitate understanding its malignant potential and long-term clinical behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.