
Abstract
Basal cell carcinomas of prostate (BCCP) are very rare. Most arise in the transition zone and thus are associated with lower urinary tract symptoms and rarely associated with elevated prostate-specific antigen (PSA). These features make diagnosis/early diagnosis difficult because of the routine protocols followed. Basal cell carcinomas have distinctive histopathological, immunohistochemical, and to some extent also different molecular characteristics. Basal cell carcinoma in situ (BCCIS) is a nonexistent histological lesion as per the current literature, but here is an attempt to describe it through this case.
A 74-year-old man presented with hematuria and previous diagnosis of prostatic hyperplasia. Based on this history, he underwent a prostatectomy ad modum Freyer. Pathological examination surprisingly revealed a diffusely infiltrative tumor with nonacinar adenocarcinoma morphology and many glandular structures probably representing BCCIS. Tumor was diagnosed as BCCP. Patient presented with metastasis to the abdominal wall 8 months postprostatectomy.
BCCP is an aggressive type of prostate cancer, which might be challenging to diagnose based on routine protocols. This results in delayed diagnosis and treatment and thus poor prognosis. Furthermore, patients with this subtype of prostate cancer need appropriately designed, and maybe a totally different follow-up regimen as PSA is of no use for BCCP patients. Finally, diagnosis of BCCIS, if agreed upon its existence needs to be studied in larger cohorts as a precursor lesion.
Keywords
Introduction
Prostate carcinomas are the most common cancer type among men in developed countries with acinar and ductal adenocarcinomas being the most common types. Basal cell carcinomas of prostate (BCCPs) are very rare, constituting <0.01% of all the malignant prostate tumors. 1 BCCP typically arises in the transition zone and leads to lower urinary tract symptoms (LUTS), leading to clinical suspicion of benign hyperplasia. 2 They might be missed by the standard prostate biopsy procedure as biopsies are taken from the peripheral zone. And thus diagnosis can be only/most often made on transurethral prostate resection specimens. 3 These tumors are known to have an aggressive clinical course 4 and 5-year survival is 28.2%, according to a recent review. 5 Prostate-specific antigen (PSA) is a relatively reliable marker for prostate adenocarcinomas, and thus used in standard protocols for follow-up. BCCP does not produce PSA as do acinar/ductal adenocarcinomas, wherein it is used for follow-up. However, it can neither be used for diagnosis nor follow-up in BCCP. 2 BCCP characteristically shows immunohistochemical positivity for basal cell markers but is negative for prostate adenocarcinoma markers and urothelial markers. Human epidermal growth factor receptor 2 (HER2) might be overexpressed in a majority of cases, and thus might be useful from the treatment perspective. 6 The terminology “Basal cell carcinoma in situ” (BCCIS) has not been coined in the published literature till date. However, somewhat similar morphologic features have been attempted to be labeled as “Basal cell hyperplasia with atypia”, “Atypical basal cell hyperplasia,” and so on.7,8 On the molecular front, BCCP has shown association with the MSMB gene, but MSMB–NCOA4 gene fusion, which has been previously detected in usual adenocarcinoma of the prostate, has never been reported in BCCP as per the latest literature. 9 The MSMB gene encodes a secretory protein, which is secreted by the prostate. The NCOA4 gene is a coregulator of the androgen receptor and is located <10 kDa from the MSMB gene. 9
Case Report
The patient had a long urological history going back 15 years prior to the BCCP diagnosis and underwent a total of 3 transrectal ultrasound (TRUS)-guided biopsies all with benign prostatic hyperplasia. A specific mention about presence or absence of “Basal cell proliferation” was lacking. A total of 10 years later, he presented with weight loss, diffuse abdominal pain and urinary retention. A computed tomographic (CT) scan disclosed Bosniak type 2F kidney cysts. A digital rectal examination disclosed a relatively symmetrically enlarged prostate without suspicion of malignancy.
Following additional 5 years at the age of 74, the patient presented with a PSA 2.9 µg/L, acute urinary retention, and he subsequently developed macroscopic hematuria in relation to intermittent catheterization. Ultrasound scanning disclosed a huge prostate volume of 262 mL and an open transvesical prostatectomy ad modum Freyer was performed, with removal of 100 g of tissue. Basal cell carcinoma was suspected on initial pathological examination at the local pathology department and subsequently confirmed at our pathology department, Rigshospitalet. As the patient had constant voiding problems and hematuria a radical prostatectomy was planned; however, surgery was postponed due to unrelated vascular surgery. The patient had a CT scan performed routinely as a part of the follow-up for his renal cyst. This demonstrated further enlargement of the prostate and a biopsy confirmed metastatic lesion in the abdominal wall. The patient is currently receiving oncological treatment with pembrolizumab and is alive 2 years after the initial BCCP diagnosis.
Material and Methods
Clinical Specimen
Histological material submitted after prostatectomy (∼100 g of tissue) and needle biopsies of abdominal wall metastasis were subjected to detailed examination. The prostatic needle biopsy performed in 2005 was also retrieved. DNA and RNA from tumor samples and DNA from blood sample (germline variants) were extracted.
Molecular Analysis
Archer FusionPlex Solid Tumor panel was performed on the abdominal wall metastasis. 10
Whole Exome Sequencing
Genomic and tumor DNA (500 ng) was processed for whole exome sequencing by KAPA HTP Library Preparation Kit (Roche) and enrichment by SureSelectXT Clinical Research Exome kit (Agilent). Paired-end sequencing (2 × 100 bp or 2 × 150 bp) was performed using Illumina HiSeq2500 or NextSeq500. Data were processed using the GATK4.1 pipeline. Germline Class 4 and Class 5 variants are reported only for selected genes (BRCA1 DNA repair associated (BRCA1), BRCA2 DNA repair associated (BRCA2), ataxia telangiectasia mutated (ATM), mutL homolog 1 (MLH1), mutS homolog 2 (MSH2), mutS homolog 3 (MSH3), PMS1 homolog 1, mismatch repair system component (MLH2), mutL homolog 3 (MLH3), mutS homolog 6 (MSH6), PMS1 homolog 2, mismatch repair system component (PMS2), partner and localizer of BRCA2 (PALB2), RAD51 paralog C (RAD51C) RAD51 paralog D (RAD51D), methyl-CpG binding domain 4, DNA glycosylase (MBD4)).
Single Nucleotide Polymorphism Arrays
A CytoScan assay (Affymetrix, Santa Clara, USA) was performed and data were analyzed by NEXUS software (BioDiscovery).
Results
Histology
Histologic examination showed a large tumor comprising approximately 75% to 80% of the total tissue submitted. The tumor was widely infiltrative with tumor cells arranged in large and small islands, solid sheets, trabecular arrangement and focally in pseudopapillary formations (Figure 1). The islands showed peripheral palisading of tumor cells. The cells were medium sized with pale eosinophilic to clear vacuolized cytoplasm. The nuclei were round to oval, hyperchromatic with few showing nucleoli. There were many mitotic figures including atypical mitoses. Frequent areas with comedo necrosis (Figure 2) and hemorrhage were present. Squamous metaplasia was prominently present, though focally and so was basal lamina material in the center of tumor islands; however, a classic “adenoid cystic” morphology was not seen. This case therefore represents a “solid variant” of BCCP. There were areas where glands were seen 2-layered, the adluminal single cell layer of normal cubical cells and abluminal broad layer of neoplastic basal cells (Figures 3 and 4). This morphology showed distinct immunohistochemistry as described below. These glands with prominent bilayering, noninfiltrative character, and a stiff basement membrane highlight a probable “basal carcinoma in situ (BCCIS),” which has not been named as such.
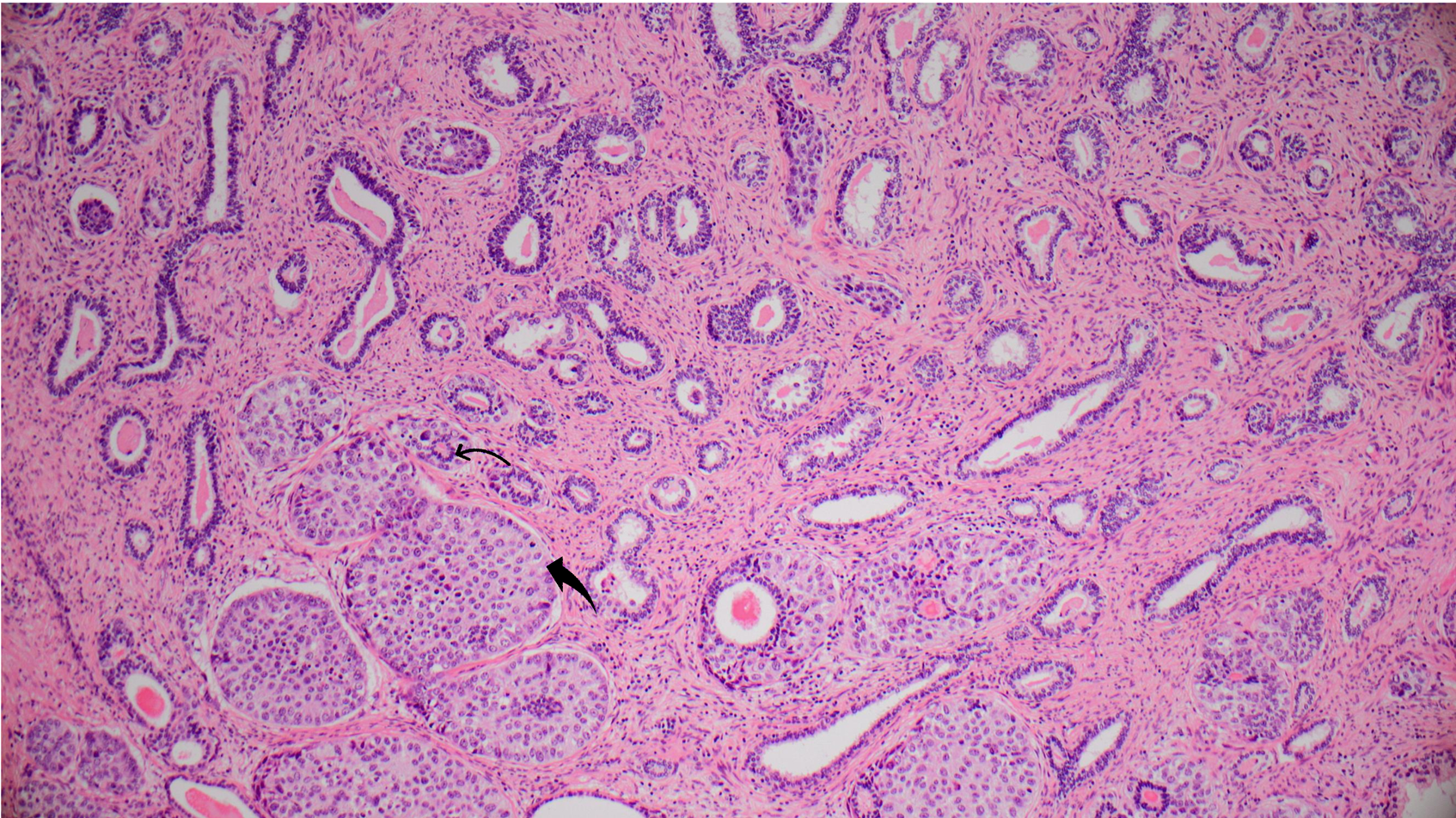
Shows areas of basal cell hyperplasia with solid nests (thick arrow) of malignant basal cells. There are nests with normal luminal epithelial cells (thin arrow) and peripheral layer of malignant basal cells (hematoxylin & eosin [HE], 10×).
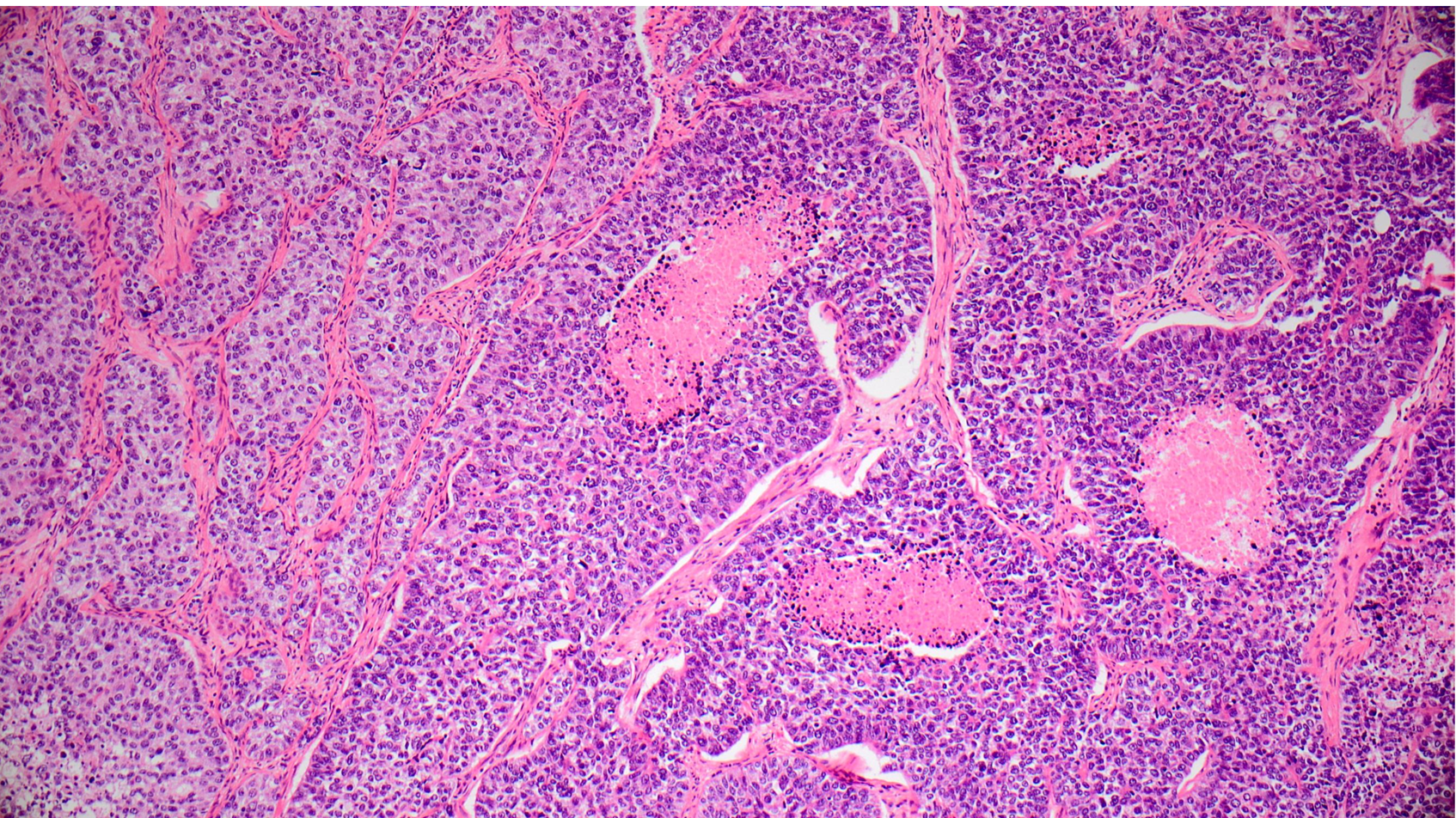
Diffusely infiltrating tumor with high-grade malignant features with multiple foci of tumor necrosis/comedo necrosis (hematoxylin & eosin [HE], 10×).
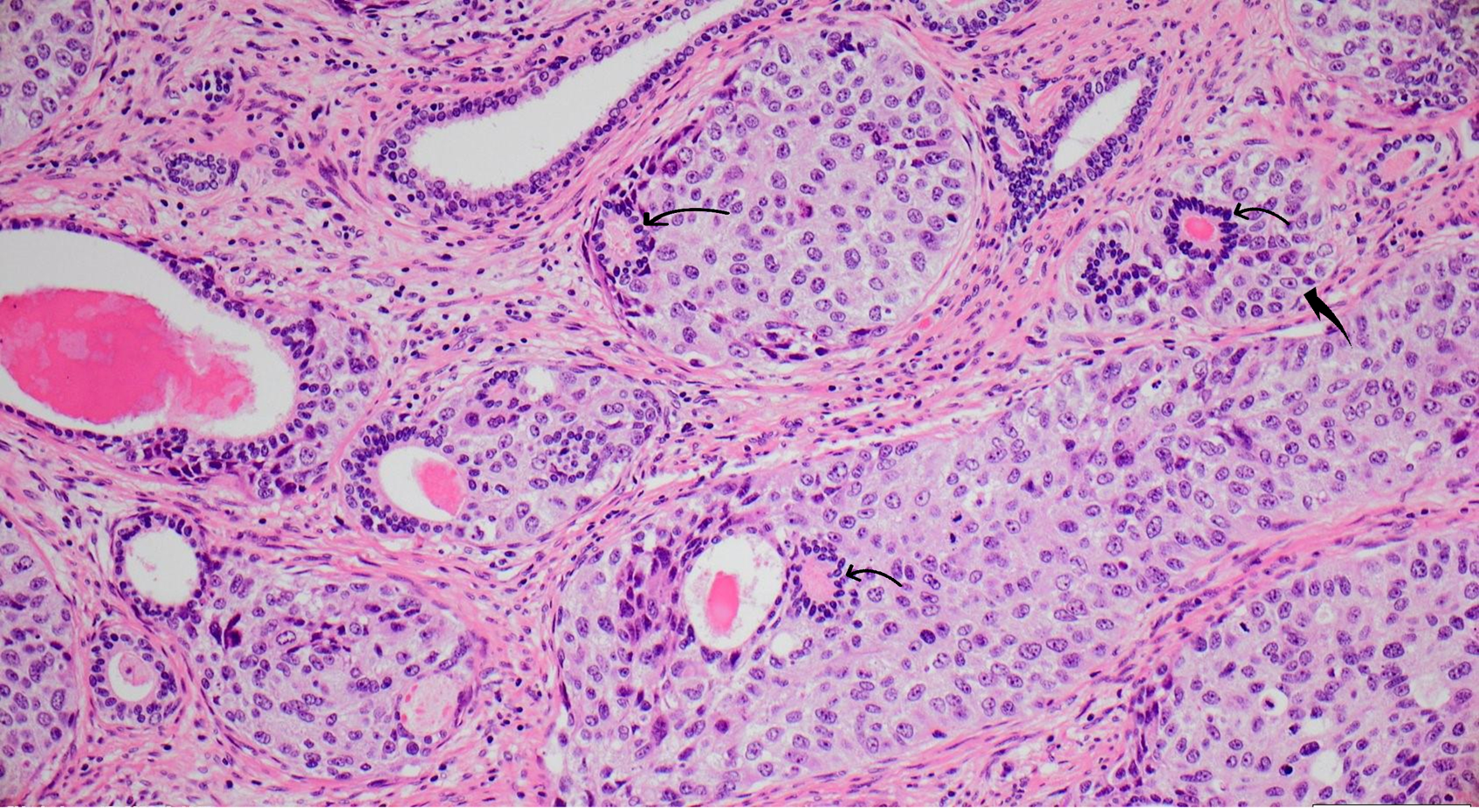
Photographs highlighting the “Classic bilayering” of normal luminal epithelial cells (thin arrows) and malignant basal cells (thick arrows) (20×). A classic BCCIS lesion.
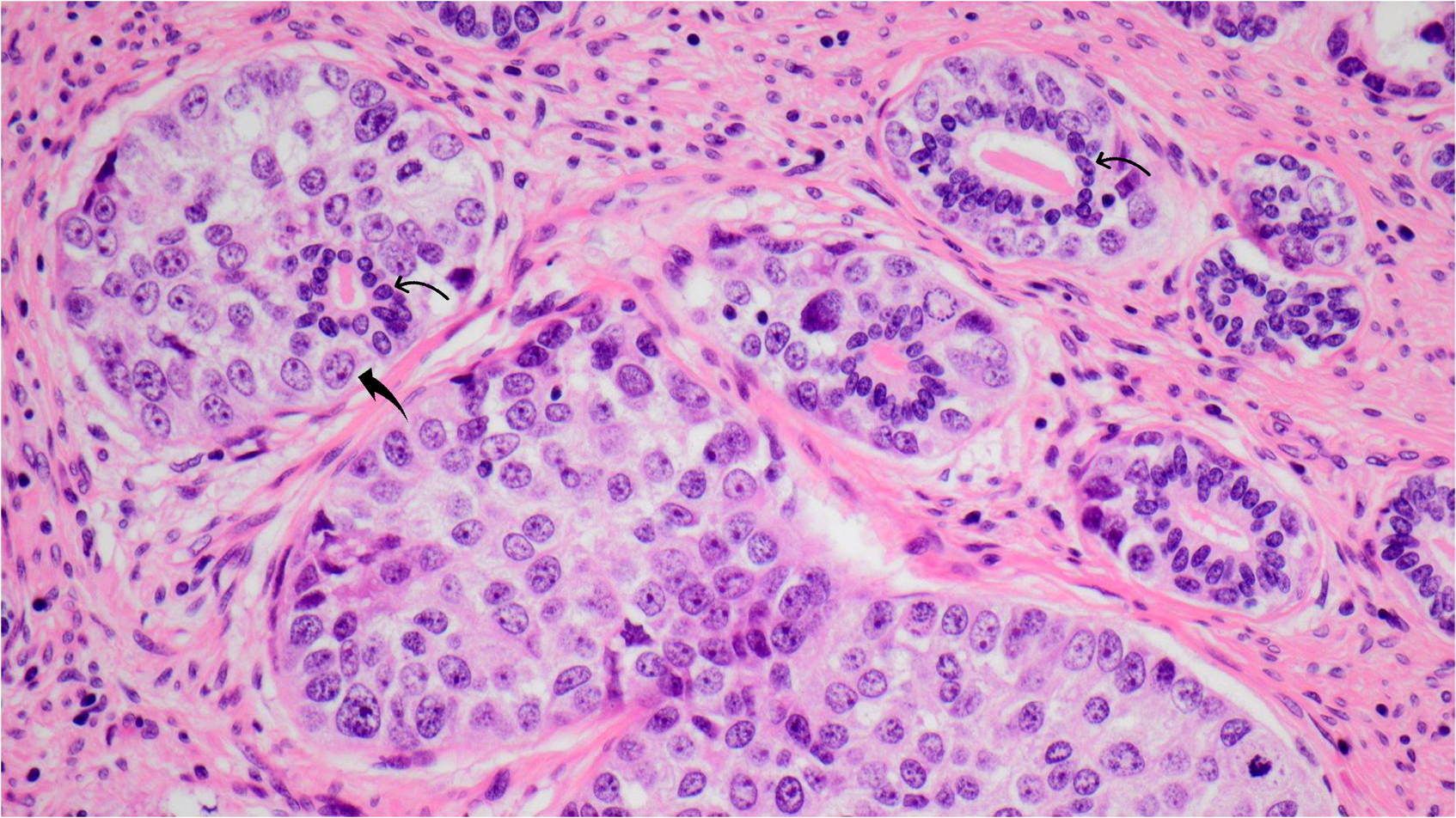
A close-up view of figure 3 (40×), highlighting BCCIS lesion.
Immunohistochemistry showed tumor cells positive for basal cell markers p63, p40, and vimentin. The cells were also positive focally for GATA binding protein 3 (GATA3). PSA, NK3 homeobox 1 (NKX 3.1) along with cytokeratin 7 (CK7), CK20, and uroplakin 2 were all negative (Figures 5 and 6). There was negative reaction for synaptophysin, chromogranin, smooth muscle myosin heavy chain (SMMS1), actin, SRY-Box transcription factor 10 (SOX10), S-100, calponin, caldesmon, B-cell lymphoma 2 (Bcl-2), thyroid transcription factor 1, and HER2. The Ki67 proliferation index was ∼30%. The BCCIS component showed adluminal cells positive for NKX 3.1, and PSA, whereas the abluminal cells were nicely decorated by basal cell markers as described above. The atypical abluminal cells showed a very high expression of Ki67 similar to the invasive component (Figure 7).
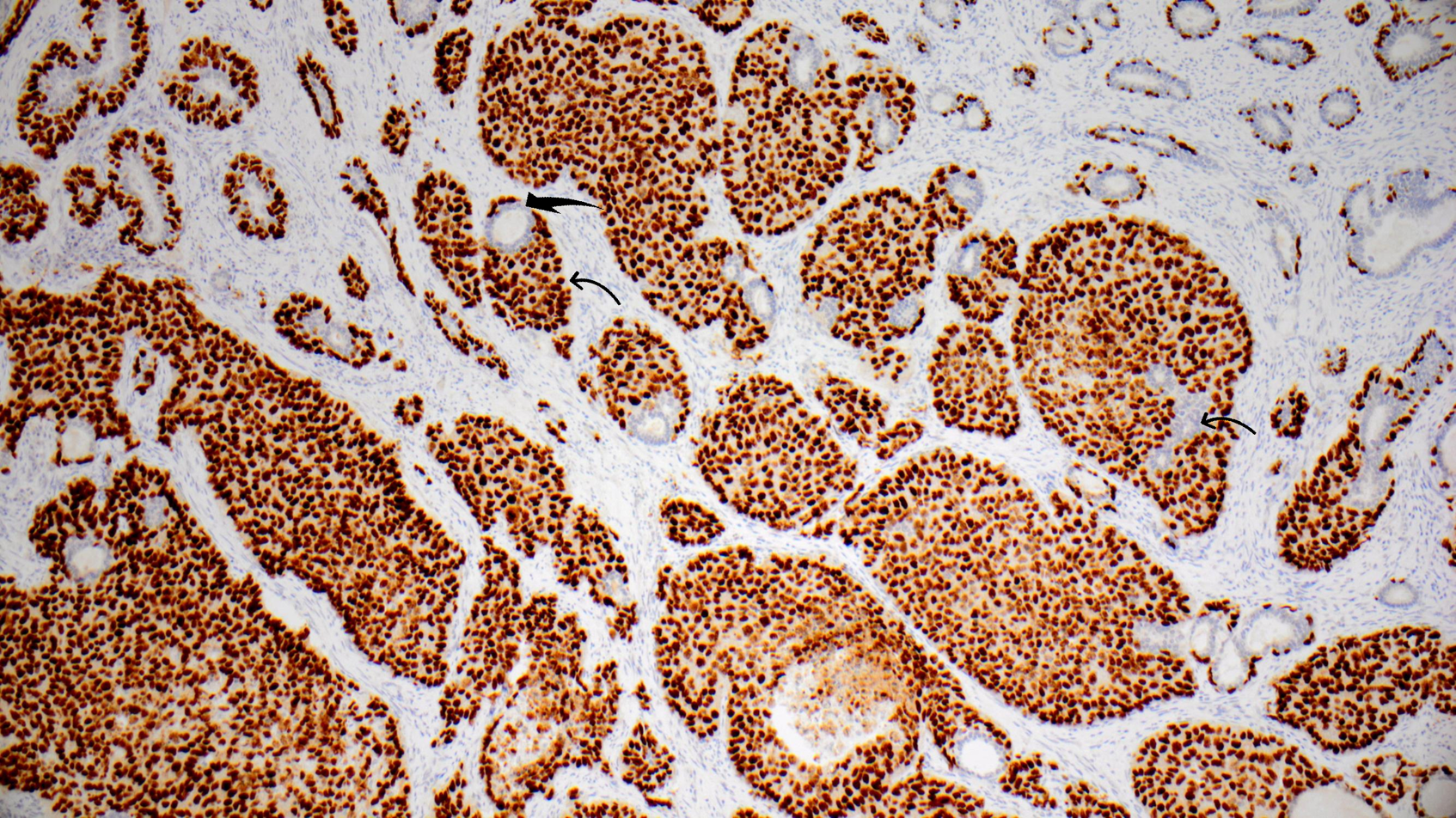
Malignant basal cells showing strong positive reaction for P63, whereas the luminal epithelial cells are completely negative (10×).

Malignant basal cells strongly positive for (a) CK5 (20×), (b) P40 (10×), and (c) vimentin (10×), whereas (d) NKX 3.1 is negative in malignant basal cells, but decorates the luminal epithelial cells (20×) (thin arrows indicate luminal epithelial cells and thick arrows indicate malignant basal cells).
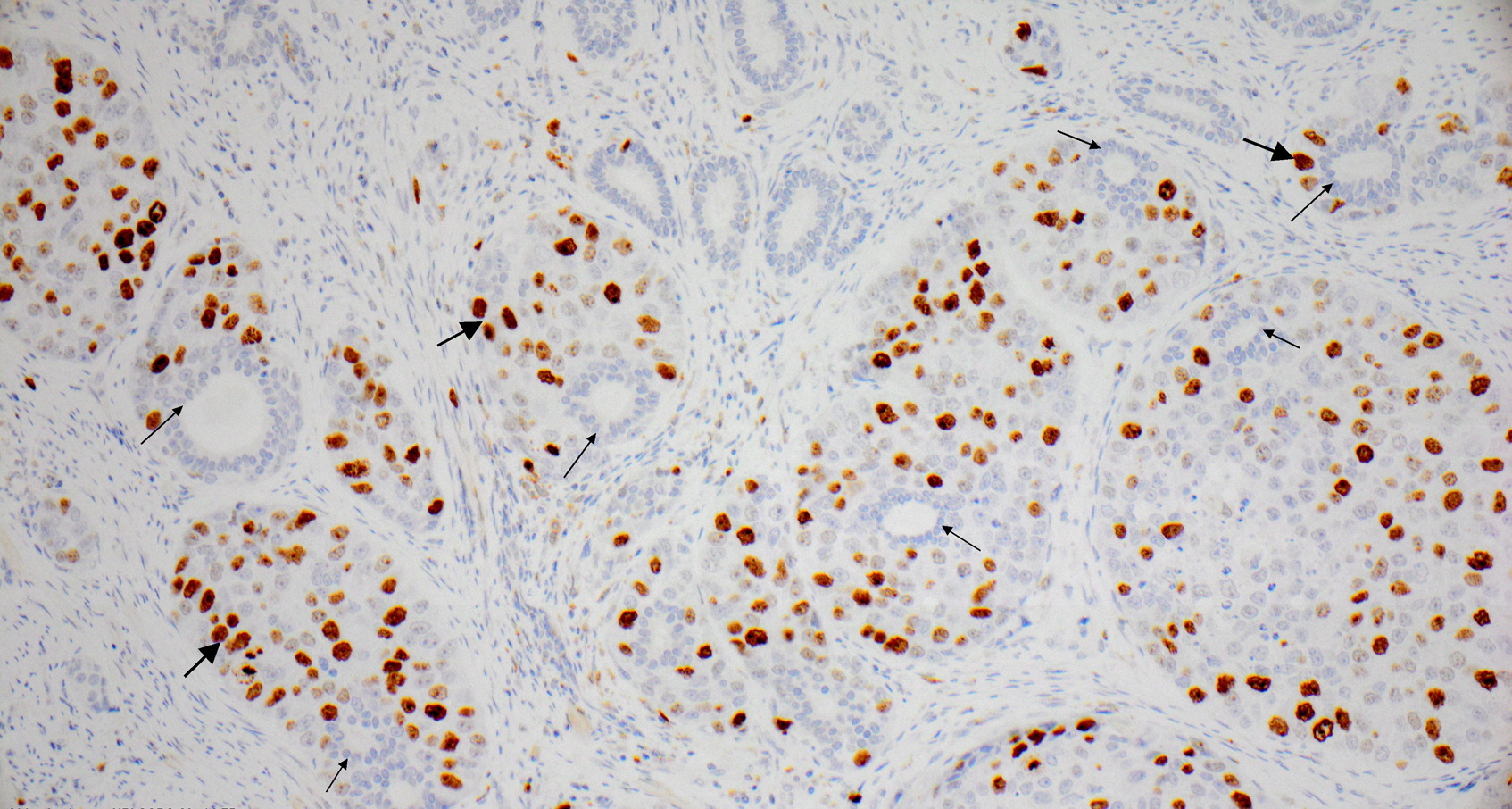
Ki67 immunohistochemistry highlighting high proliferation rate in the abluminal cells (wide pointed arrows) and negative adluminal cells (thin pointed arrows). There are also normal glands seen in the upper part without proliferation (20×).
Molecular Findings
Molecular examination detected microseminoprotein beta (MSMB)–nuclear receptor co-activator 4 (NCOA4) fusion (breakpoint chr10:51556856 and chr10:51579128). Due to the tumor content being <10% in the biopsies, extensive genomic analysis was limited; somatic amplification of fibroblast growth factor receptor 1 and BMP/retinoic acid inducible neural specific 2, and of Class 4 germline variant in ATM (c.3284 + 1 G > A) was reported.
Discussion
BCCP, also referred to as adenoid cystic carcinoma, is a very rare malignant neoplasm of the prostate. Age at presentation is similar to acinar/ductal prostate adenocarcinoma. Rarity, need of appropriate management guidelines, and tumor nonresponsiveness to standard treatment are the reasons for poorer prognosis.2-5 BCCP shows either adenoid cystic, basaloid, or solid pattern; the most common being the mixed variety. Our case belonged to the solid variant, which is quite rare. Differential diagnosis includes benign basal cell hyperplasia and the most common variant of prostate cancer, the acinar adenocarcinoma. Infiltrative growth pattern, cellular atypia, mitoses, and necrosis are deficient in basal cell hyperplasia. The peripheral location in most nonadvanced cases, elevated serum PSA, morphology, and characteristic immunohistochemical profile defines acinar prostate adenocarcinoma. On immunohistochemical analysis BCCPs express basal cell markers, and HER2 is usually positive; however, it was negative in this case. 2 Also, Bcl-2, which is reported to be strongly and diffusely positive in BCCP, was found to be completely negative. 11 A very rare p63 positivity has been described in acinar adenocarcinoma, but in such cases other basal cell markers are always negative and NKX 3.1 and PSA are positive. The Ki67 index coupled with morphology can usually help distinguish BCCP from benign “mimickers of neoplastic lesions” including basal cell hyperplasia.
As described above, we found a very characteristic morphological finding described in the histology section. This might represent BCCIS and after an extensive literature search we can conclude that to the best our knowledge, this morphologic feature has not been named as BCCIS yet.7,8,12 Similar morphologic features have previously been labeled “Atypical basal cell hyperplasia”, as described above. In this, the cells are enlarged with prominent nucleoli, and Rioux-Leclercq and Epstein 7 have also included presence of mitoses in its definition. To avoid the confusion because of overlapping definitions, we suggest the 2-layered, well-defined, noninvasive glandular structures with normal adluminal cell layer and malignant abluminal cell layer being the defining characteristics of “basal cell carcinoma in situ” with typical immunohistochemical reaction described above. The term malignant has been applied because (a) the abluminal cells had a similar morphologic appearance as the infiltrating tumor cells, (b) Ki67 expression was very high, (c) mitotic figures were present, (d) prominent nucleoli were present, and (e) the cells were arranged in a completely unorderly manner. As per our best understanding, these criteria separate BCCIS from a well-described “Atypical basal cell hyperplasia”. The differential diagnoses of BCCIS other than basal cell hyperplasia are pagetoid spread of the usual prostate acinar adenocarcinoma and pagetoid carcinoma in situ (CIS)/spread of urothelial carcinoma. Extensive sampling of the prostatic tissue, morphology and immunohistochemistry will help rule out the first. Urothelial CIS shows relatively large malignant cells with many having clear cytoplasm, urothelial neoplasia elsewhere and positive immunohistochemical reaction for GATA3, CK7, and Uroplakin 2. The detailed work-up in our case ruled out these possibilities.
As previously mentioned, there is no evidence that atypical basal cell hyperplasia is a precursor to cancer. 7 However, BCCIS, if well accepted among uropathologists, might represent a premalignant lesion and probably a risk factor for development of subsequent BCCP. As this is probably the first observation of this morphologic feature, to the best of our knowledge, it is not possible to comment on the behavior of BCCIS compared to the other atypical lesions described. A multi-institutional study with special emphasis on looking for this novel pathology (BCCIS) in a larger cohort will help elucidate further details. This will include emphasizing our hypothesis whether this might serve as a precursor lesion. Diagnosis of BCCIS, as with other carcinomas in situ, if carried out early might result in overall better prognosis. Glands with similar morphology have been labeled in the past as basal cell hyperplasia with atypia, but in our case the cells are frankly neoplastic and not just atypical and are also associated with an infiltrative tumor in the vicinity.7,8
There have been several genetic alterations described in the common adenocarcinoma of the prostate, including the PI3 K pathway, the phosphatase and tensin homolog (PTEN), MYC proto-oncogene, bHLH transcription factor (MYC), and tumor protein P53 (TP53) genes and gene fusions such as transmembrane serine protease 2 (TMPRSS2)–ETS transcription factor ERG (ERG3)3 and MSMB–NCOA4. 13 Gene fusions like proto-oncogene, transcription factor (MYB)–nuclear factor I B (NFIB) have also been previously described in prostatic basal cell carcinoma. 14 In a study by Bishop et al, 12 MYB rearrangement was found exclusively in tumors with adenoid cystic morphology and none in pure solid variants. In our case, a pure solid variant, MSMB–NCOA4 fusion was detected for the first time in BCCP. As both fusion genes are relevant for prostate tissue and MSMB for prostate cancer, 13 this fusion can be considered of importance for BCCP tumorogenesis. However, more functional studies are needed.
The patient was followed up with clinical examination and serum PSA. However, as mentioned earlier, PSA is an inappropriate marker to monitor recurrence or metastases. Therefore, we recommend follow-up after the prostatectomy for basal cell carcinoma should be reviewed. It would be suggested that as an alternative to PSA, radiologic and detailed clinical studies could potentially provide a better outcome and a search for an easier, noninvasive and noncumbersome marker should be initiated.
Very rare tumor. LUTS symptoms can hamper early diagnosis. Localized in transition zone unlike the common acinar variant. May harbor gene fusions. PSA is not useful either for diagnosis or follow-up. Delay in diagnosis and treatment resulting in worse prognosis. Need for consensus guidelines for treatment and follow-up.
Conclusion
Basal cell carcinoma of prostate is a rare tumor and there is need for an appropriate management protocol as it cannot be followed up by serum PSA. A multi-institutional cohort might pave the way for better understanding of this rare tumor.
Footnotes
Author Contributions
The first draft of the manuscript was written by Vilde Pedersen with guidance from Anand C Loya, who laid out the framework of article, and all authors commented on this version. Katrine Stenfeldt Petersen and Anand C Loya performed the histopathological evaluation. Klaus Brasso provided the clinical data. Anand C Loya and Olga Østrup performed the molecular analysis and interpreted its results. The authors read and approved the final manuscript.
Acknowledgment
The authors would like to thank Nina Claire Woller, consultant pathologist, for critical editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or information included in this article.
Trial Registration
Not applicable, because this article does not contain any clinical trials.