
Abstract
Thymic epithelial neoplasms are the most common tumors of thymic origin but are overall rare in the general population. Their morphologic diversity, ranging from low grade to overtly malignant lesions, along with various histologic growth patterns make them a diagnostically challenging group of tumors. Very occasionally, thymomas and thymic carcinomas may develop in combination with other benign or malignant lesions of thymic origin, further complicating the diagnostic process. The focus of this review lies on the spectrum of thymic epithelial tumors that present with other thymic lesions in the same tumor mass, such as multilocular thymic cysts, neuroendocrine neoplasms, lymphomas, and germ cell tumors among others. Awareness of the existence of such unusual tumors may not only aid in their diagnosis but may also have implications for prognostic and therapeutic purposes.
Introduction
The thymic gland can give rise to a wide spectrum of benign and malignant conditions, including tumors of epithelial, mesenchymal, hematopoietic and germ cell origin. In the adult population, thymic epithelial tumors, namely thymomas and thymic carcinomas, are the most common neoplasms, accounting for approximately 25% to 30% and 14% to 22% of all mediastinal tumors, respectively.1–3 The histologic variability of these tumors is a well-recognized phenomenon; in fact, approximately 50% of thymomas are of mixed histology, composed of more than one histological pattern. 4 Moreover, spindle cell thymomas (World Health Organization type A) and thymic carcinomas, in particular, are a very heterogeneous group of tumors, characterized by a wide morphologic spectrum.5,6 Consequently, definitive tumor subtyping can be challenging when dealing with small volume core biopsies.
Patients with thymoma are also known to harbor an increased incidence of synchronous and metachronous neoplasms in sites other than the mediastinum, including various carcinomas, hematolymphoid neoplasms and sarcomas.7–11 The simultaneous occurrence of thymoma or thymic carcinoma with other lesions of thymic origin, both benign and malignant, in the same tumor mass is an unusual event that has only been recorded in the literature very infrequently.
The existence of such composite lesions adds to the complexity of thymic epithelial neoplasms with consequences for diagnosis, treatment and prognosis. This review offers an overview of the reported literature, explores the presumed histogenesis and discusses the clinicopathologic characteristics of these unusual tumors.
Clinicopathologic Features
Thymic Epithelial Neoplasms and Multilocular Thymic Cyst
Initially thought to be a rare occurrence, the concurrent presence of a multilocular thymic cyst associated with thymomas or thymic carcinomas has since been documented in up to 17% of thymomas and 12% of thymic carcinomas in the largest reported series.12,13 Despite this, overall, only approximately 50 such lesions have been reported in the literature.12–15
On average, patients with these unusual neoplasms are in the sixth decade of life at the time of diagnosis; males appear to be more frequently affected with a male to female ratio of 3:1. The majority of patients presents with symptoms of chest pain, dyspnea, or cough, although some patients may be entirely asymptomatic. Imaging reveals the presence of anterior mediastinal masses with variable evidence of invasion into adjacent structures. Interestingly, cystic changes are only identified preoperatively in about half of these tumors. 15
Grossly, in addition to a solid tumor mass, most tumors contain a peripheral cystic component characterized by multiloculated spaces with thin walls and an individual cyst size ranging from 0.5 to 3.0 cm12,13,15 (Figure 1). Overall, the entire tumors can measure up to 15 cm in maximum diameter.12–15 Microscopically, in addition to the thymoma or thymic carcinoma components, the adjacent remnant thymic tissue contains multiple cystic structures lined by stratified squamous, low cuboidal or columnar epithelium with bland cytologic features and filled with amorphous material, cellular debris or desquamated epithelial cells. The cyst walls are composed of fibroconnective tissue and may contain remnant thymic tissue and prominent inflammatory changes, including reactive lymphoid follicles with germinal centers, cholesterol clefts, areas of fibrosis or a granulomatous response.12,13,15 The associated thymic epithelial neoplasm will show the typical morphological features of these tumors (Figure 2). Briefly, thymomas consist of a neoplastic epithelial proliferation and variable infiltrate of non-neoplastic T lymphocytes (thymocytes). The World Health Organization classifies these tumors based on the shape of the epithelial cells and extent of infiltrating thymocytes into types A, AB, B1, B2 and B3 16 (Table 1). The cytologic features of the neoplastic epithelial cells are generally bland, mitotic activity is low and organotypical characteristics of the thymic gland (lobulation, fibrous bands, perivascular spaces, lymphocytic infiltrate) are retained. Moreover, there is a range of thymomas that cannot be categorized into the existing world health organization schema and are classified separately. 16 Thymic carcinomas on the other hand, are overtly malignant neoplasms that have lost the organotypical attributes and are characterized by malignant epithelial cells with nuclear pleomorphism, mitotic activity and necrosis embedded in a sclerotic background. Squamous cell carcinoma is the most common type, but various other histological subtypes are on record.6,16
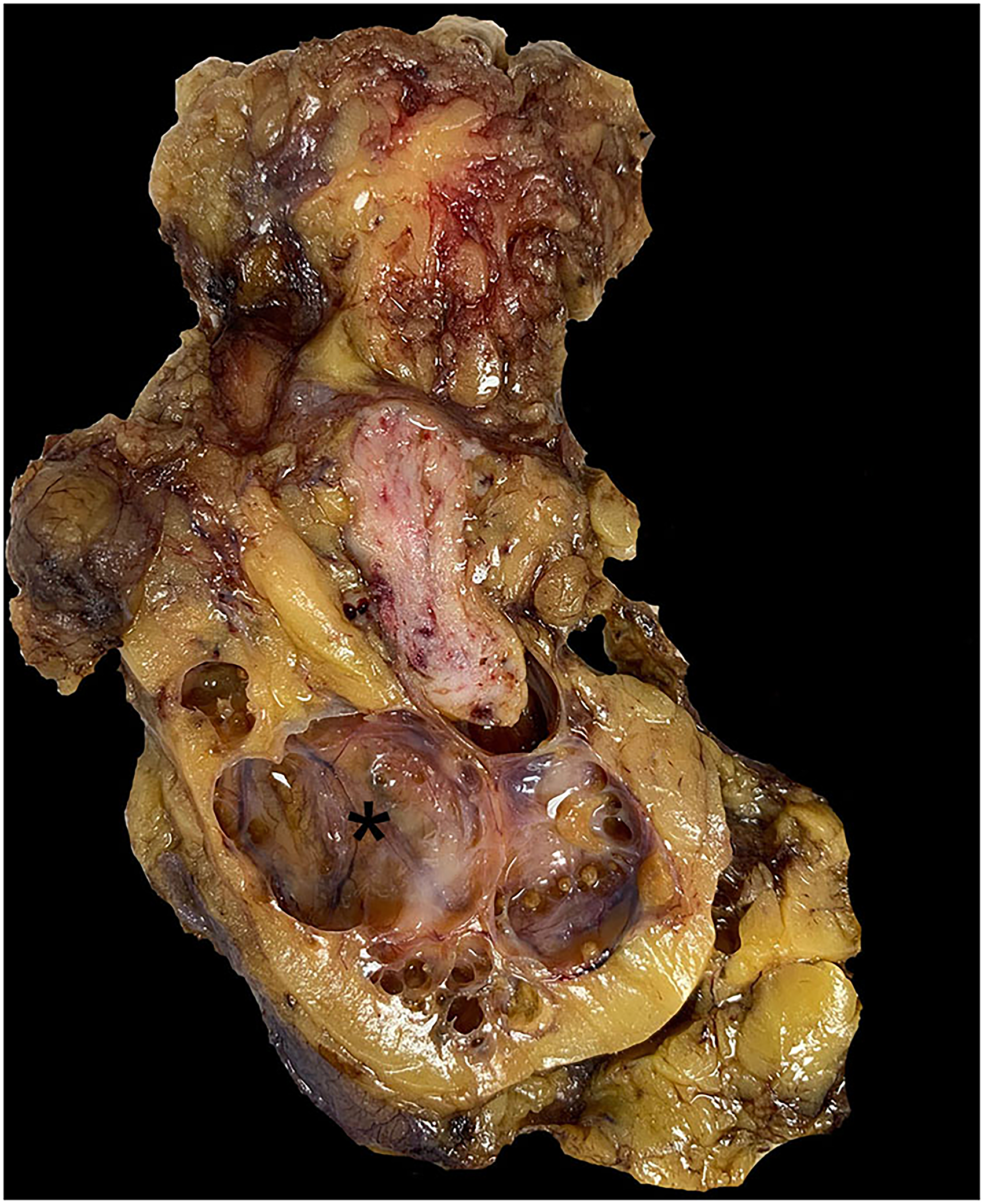
Multiple cystic spaces (asterisk) are seen adjacent to a thymoma in this combined thymoma with multilocular thymic cyst.
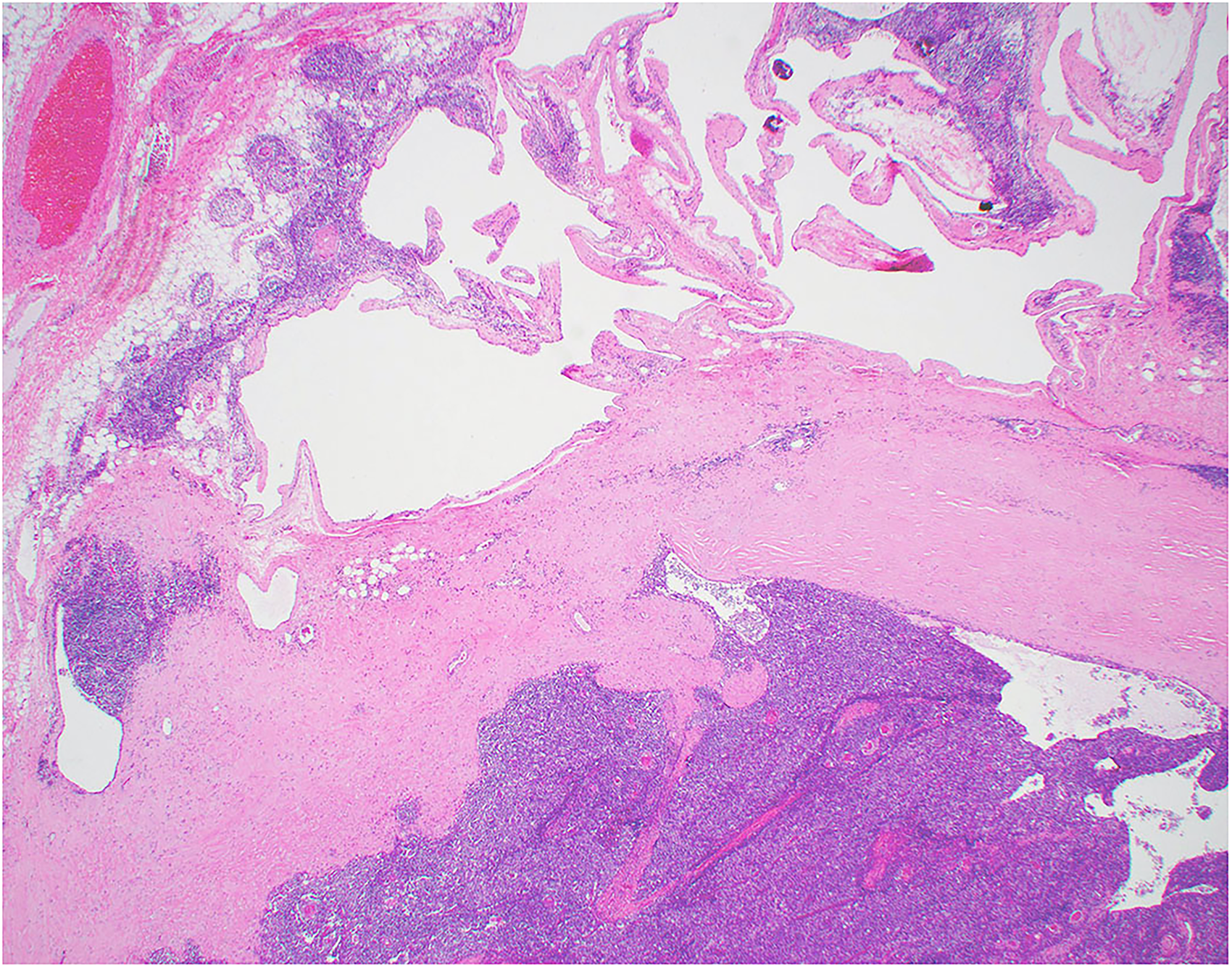
Low power view of a thymoma (lower half) associated with a multilocular thymic cyst (upper half). The cystic component consists of multiple cystic spaces lined by benign squamous or respiratory epithelium. The cyst walls often show reactive inflammatory changes characterized by chronic inflammation, lymphoid follicles with germinal centers, fibrotic changes and cholesterol clefts (H&E x2).
Thymoma Classification as per World Health Organization 2021. 15

The thymoma component in these combined lesions can be of any subtype, with reported components ranging from type A to type B3 thymomas,12,15 while thymic carcinoma subtypes included squamous cell carcinoma, basaloid carcinoma, sarcomatoid carcinoma, papillary adenocarcinoma and lymphoepithelial carcinoma.12,13
Surgical resection is the treatment of choice and may be accompanied by radiotherapy or chemotherapy depending on the extent of invasion into adjacent structures. Curiously, the clinical behavior of thymomas and thymic carcinomas with an associated multilocular thymic cyst appears to be superior to thymic epithelial neoplasms without such association, although this impression ideally needs to be confirmed in larger series.12,13,15
Combined Thymoma and Thymic Carcinoma
The finding of areas of thymoma and thymic carcinoma in the same tumor mass is uncommon. The largest series describing this phenomenon was published by Suster and Moran recording 22 such tumors. 17 Reference to this particular type of combined tumor is also made in a number of other publications on thymoma or thymic carcinoma, amounting to a total of around 35 additional tumors.6,18–23
The clinical presentation and radiologic findings are indistinguishable from those elicited by pure tumors and the combined nature is usually only recognized once surgically resected. In this context, the age of presentation of patients with combined tumors ranges from 23 to 86 years with a mean age in the sixth decade. Interestingly, these tumors seem to be more common in men, with a male to female ratio of 3:1. Chest pain is the most common symptom although patients can remain entirely asymptomatic.6,17–23 Grossly, tumors may be encapsulated or infiltrative lesions with a size ranging from 4.5 cm to 20 cm. The cut surface usually has a variegated appearance with firm rubbery areas alternating with soft, necrotic or hemorrhagic zones. On a microscopic level, the thymomatous component often outweighs the carcinomatous one. Any type of thymoma may be seen in this context. Among the carcinomas, squamous cell carcinoma is the most common subtype encountered, but other types, such as clear cell carcinoma, lymphoepithelial carcinoma, papillary adenocarcinoma, sarcomatoid carcinoma and anaplastic carcinoma have also been recognized in this context.6,17–23 The most common combination, however, appears to be a type B thymoma alongside squamous cell carcinoma. 17 The majority of these combined tumors will demonstrate areas of gradual transition although lesions with more abrupt transition have also been documented 17 (Figure 3a and b). The value of immunohistochemical studies to divide thymoma from carcinoma are of limited value in this context as both tumors share a similar immunophenotype. Thymic epithelial cells are universally positive for pankeratin, keratin 5/6, p40, and PAX8 (polyclonal) while thymocytes are immature T cells that express TDT, CD1a and CD99; in addition, the tumor cells of thymic carcinomas, but not thymomas, have been found to be reactive for CD5 and KIT (CD117). 6 Most tumors, however, can be diagnosed by light microscopy alone based on the characteristic tumor morphology, obviating the need for ancillary analysis.
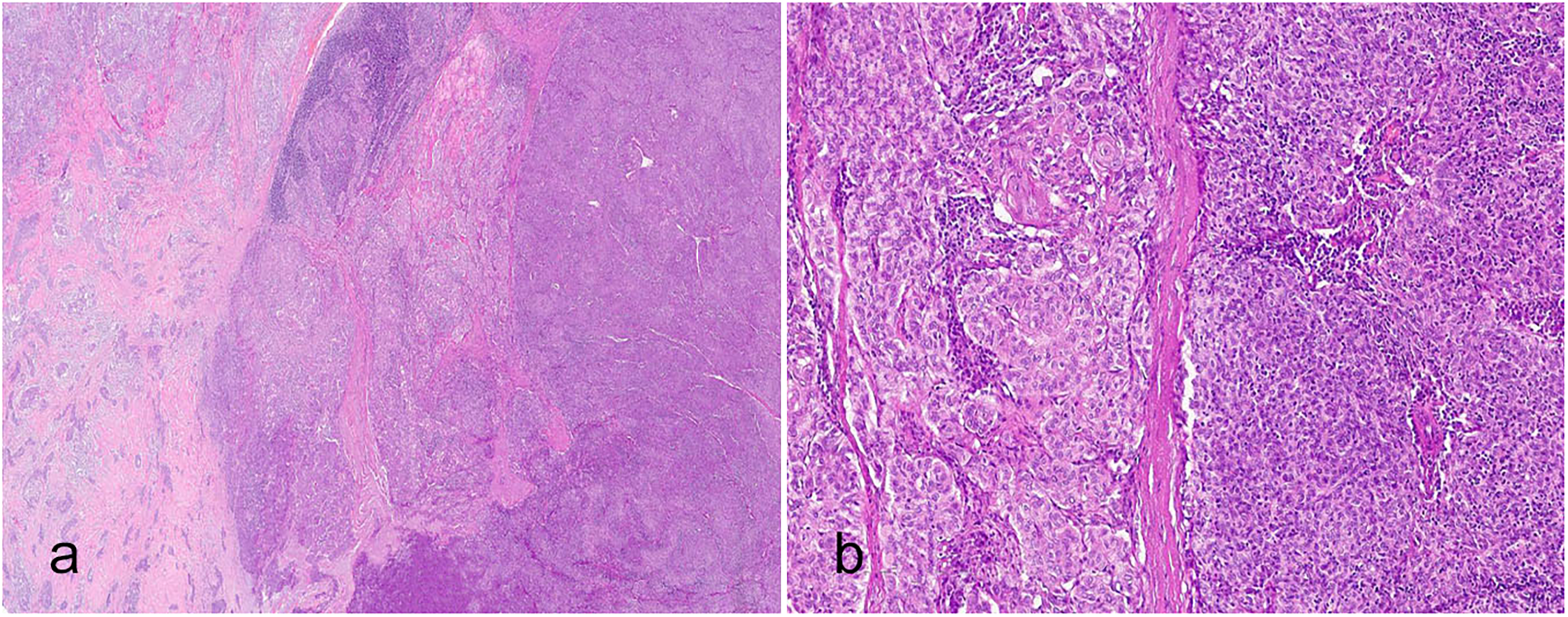
(a) A combined thymoma (right) and thymic carcinoma (left) with abrupt transition between the two components (H&E x2); (b) on higher power, the cytologic features of the two components becomes evident: the thymic carcinoma shows an overtly malignant tumor characterized by sheets of tumor cells with vesicular nuclei and cytologic atypia while the thymoma shows bland tumor cells infiltrated by thymocytes (H&E x4).
The treatment of choice includes complete surgical resection, supplemented by chemotherapy or radiation depending on the extent of invasion. The prognosis is primarily determined by the more aggressive, ie carcinomatous component. 17
Thymic Epithelial Neoplasms and Neuroendocrine Neoplasms
Thymomas and thymic carcinomas have also occasionally been reported to present as composite tumors with neuroendocrine neoplasms.24–29 In one of the first descriptions, Snover et al 25 documented three patients with thymic squamous cell carcinoma whose tumors were intimately admixed with components of small cell carcinoma. Further reports described combined tumors consisting of thymoma (A, AB and B types) and carcinoid tumor (typical and atypical types) or large cell neuroendocrine carcinoma24–29 (Table 2).
Reported Cases of Combined Thymic Epithelial and Neuroendocrine Neoplasms.
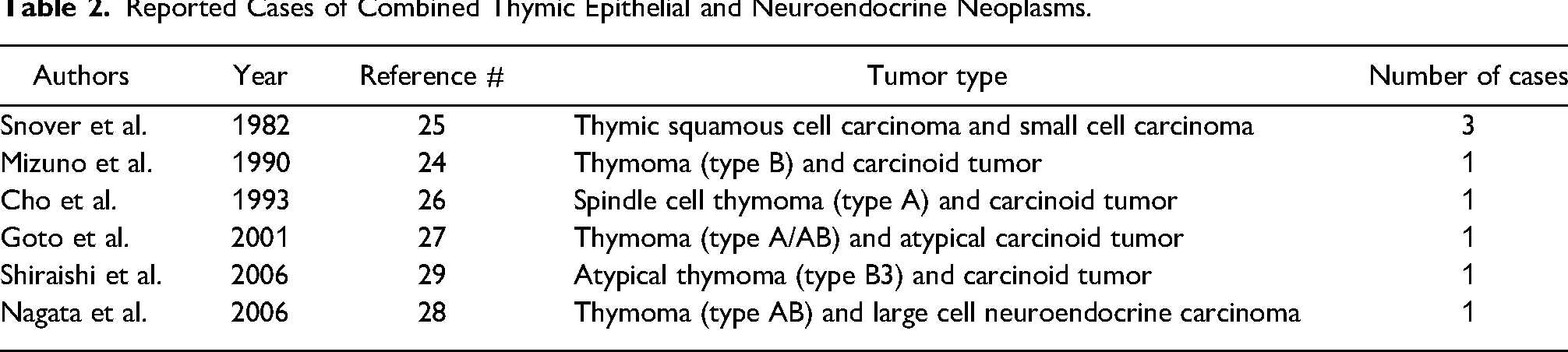
From a clinical perspective, the patient age at presentation ranged from 29 to 70 years and symptoms, if any, included chest pain, myasthenia gravis-related signs, or dyspnea. Males and females were equally affected. Gross examination revealed large (5-20 cm), heterogeneous, cystic or solid masses with variable invasion into adjacent structures. Histologically, the thymoma component ranged from spindle cell (type A) to epithelioid cell type (type B3) with focal or abrupt transition to the neuroendocrine elements. The latter consisted of scattered foci or larger areas with the typical morphology of neuroendocrine neoplasms, ie organoid growth pattern, including peripheral palisading, rosettes, and trabecular growth. Distinction into the various subtypes (carcinoid tumor, atypical carcinoid tumor, large cell carcinoma or small cell carcinoma) is achieved by attention to nuclear detail, degree of mitotic activity and presence or absence of necrosis. 30 Neuroendocrine differentiation was confirmed by immunohistochemical expression of neuroendocrine markers, including synaptophysin, chromogranin A, CD56 and neuron-specific enolase.28,29
Like with other combined tumors, surgical resection is the mainstay of therapy. Adjuvant radiotherapy and chemotherapy either before or after surgery are additional treatment options. Survival appears to depend on the histologic subtype of the tumors. Two of the patients with composite thymic squamous cell carcinoma/small cell carcinoma died of the disease within 5 years while the third patient was alive with metastases 1 year after diagnosis. 25 All other reported patients with clinical information were alive and well with a follow up period from 7 months to 4 years, including the patient with the large cell neuroendocrine carcinoma component.24,26–29
Thymic Epithelial Neoplasms and Lymphomas
Although several patients with concurrent lymphoma and thymoma have been described, very few articles report the coexistence of thymoma and lymphoma within the same tumor mass31–34 (Table 3).
Reported Cases of Combined Thymic Epithelial Neoplasms and Lymphoma.

All but one of these patients were men in the seventh decade of life who were asymptomatic or complained of fever and chest pain. On imaging, anterior mediastinal masses were identified but no significant lymphadenopathy, splenomegaly or hepatomegaly was noted. Grossly, the tumors were large, ranging from 5 cm to 12 cm in greatest diameter and were variably encapsulated. Infiltration into surrounding structures was noted in one tumor. 32 The cut surface of the tumors was characterized by multiple tan nodules with a firm, rubbery consistence, partially replaced by fibrosis and necrosis and with or without small cystic areas.31–33 Microscopically, the tumors appeared closely intermingled; sheets of epithelial cells of either spindled or epithelioid morphology representing the thymoma component were intimately admixed with atypical lymphocytes. In most tumors, the lymphoma component consisted of medium-sized cells with convoluted nuclei with condensed chromatin and high mitotic activity. Immunohistochemically, these were positive for TDT, CD1a, CD99, CD5, and CD3 and negative for CD20, consistent with T cell lymphoblastic leukemia/lymphoma.31,32,34 Clonal rearrangement of the T cell receptor ß chain gene in the lymphocytic tumor component was identified in one patient 32 while in the other two, lymph node 34 and skin involvement 31 eventually revealed the malignant nature of the lymphoid components. Interestingly, in Macon et al's patient, 34 malignant transformation of the lymphoid component occurred in a tumor recurrence, 5 years after initial thymoma resection and following chemotherapy and irradiation. In the fourth tumor, the two tumor components appeared more separated. 33 The thymic epithelial cells formed nests of spindled cells with bland cytologic features. These nests were separated by the lymphocytic cells which were composed of small, uniform lymphocytes with scant cytoplasm, round nuclei and condensed chromatin. Several proliferation centers (pseudofollicles) containing increased prolymphocytes and paraimmunoblasts were also identified. By immunohistochemistry, the neoplastic lymphocytes were positive for CD5 (dim) and CD20 while negative for CD3 and CD21, consistent with chronic lymphocytic leukemia/small lymphocytic lymphoma. Characteristically, extension of the lymphoid component into the surrounding perithymic tissue or adjacent structures, such as lung or hilar lymph nodes was present to various degrees in all lesions (Figure 4a to e).

(a) Low power view of a thymoma (lower half) combined with chronic lymphocytic leukemia/small lymphocytic lymphoma (upper half) (H&E x 2); (b) the thymoma is a micronodular thymoma with lymphoid hyperplasia, consisting of small islands of thymic epithelial cells embedded in a lymphoid stroma (H&E x 10); (c) the lymphoma is composed of monomorphic small lymphocytes with characteristic extension into the perithymic fat (H&E x 4); (c) by immunohistochemistry, the neoplastic thymic epithelial cells are highlighted by pankeratin (x4) while (d) the lymphoma shows diffuse staining for CD20 (x10).
Surgical resection occurred in all patients and ultimately led to the diagnosis. The prognosis for these composite tumors seems to depend on the malignant lymphoid rather than the epithelioid component; two patients with combined thymoma/lymphoma died from disseminated T cell lymphoblastic leukemia/lymphoma 8 months and 24 days after initial diagnosis, respectively,31,34 one after having received chemotherapy for the hematologic component. 31 The other patients with T cell lymphoblastic leukemia/lymphoma are alive and well and in remission after having received similar treatment.32,34 Therapy for the patient with chronic lymphocytic leukemia/small lymphocytic lymphoma component consisted of close clinical follow-up postoperatively and the patient remains alive and well after limited observation. 33
Thymic Epithelial Neoplasms and Germ Cell Tumors
Thymic epithelial tumors combined with germ cell tumors in the same tumor mass are exceedingly rare. Only four such tumors have been reported in the literature35–37 (Table 4).
Reported Cases of Combined Thymic Epithelial Neoplasms and Miscellaneous Tumors.

All of these comprised of a combination of thymoma with seminoma and were diagnosed in young male patients (32 to 46 years of age). Most patients presented with chest pain, shortness of breath or cough; one tumor was detected on routine medical examination (Figure 5). None of the patients had any history of testicular tumor or elevated serum biomarkers. The tumors were large (range: 6 cm to 10 cm) anterior mediastinal masses that on gross examination were circumscribed solid or solid-cystic neoplasms with a gray-red or tan cut surface and areas of hemorrhage and necrosis.35–37 On a microscopic level, the two tumor components may be closely apposed or separate nodules within the same specimen (Figure 6a to f). In addition to the typical features of thymoma, the seminomatous component presented as sheets of epithelioid cells with abundant pale cytoplasm and prominent nucleoli. These cells were percolated by small mature lymphocytes. Immunohistochemically, the seminoma cells were positive for keratin (perinuclear dot-like), KIT (CD117), SALL4, OCT3/4 (POU5F1), placental alkaline phosphatase, and D2-40 while negative for p40 and CD5.35–37 In one tumor, the seminoma component was accompanied by a prominent hyperplastic lymphoid follicular process which is a characteristic morphologic finding in mediastinal seminomas. 38 In another, the seminomatous tumor component was only recognized after re-review of the resection specimen when the patient presented with a pleural effusion. 37 In this particular tumor, the thymoma component had an epithelial appearance (type B3) with scant lymphoid infiltrate and therefore closely resembled the seminomatous areas causing the initial misdiagnosis.
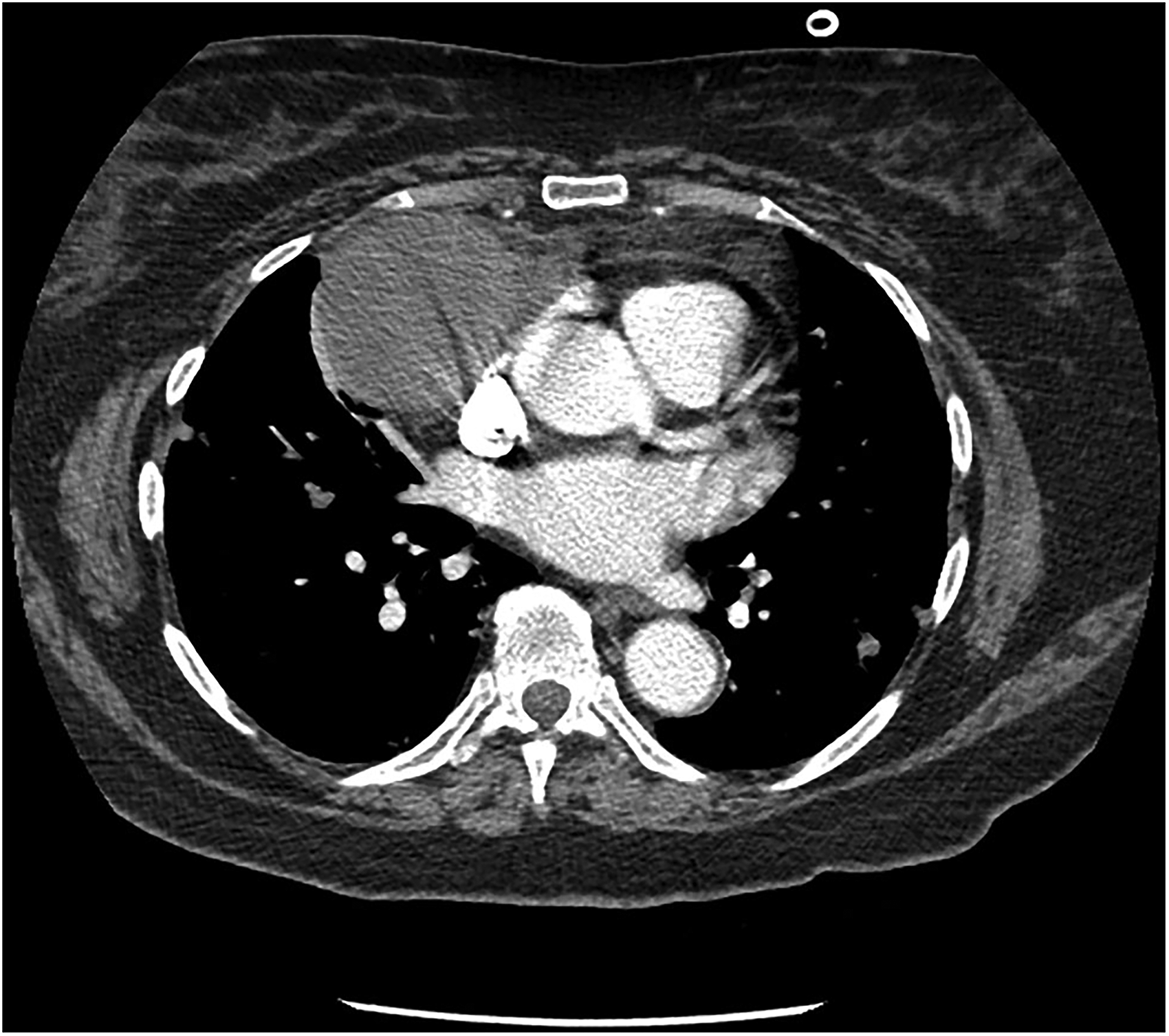
Computed tomography scan of a patient with combined thymic epithelial neoplasm and germ cell tumor. A large tumor mass is apparent in the right anterior mediastinum.

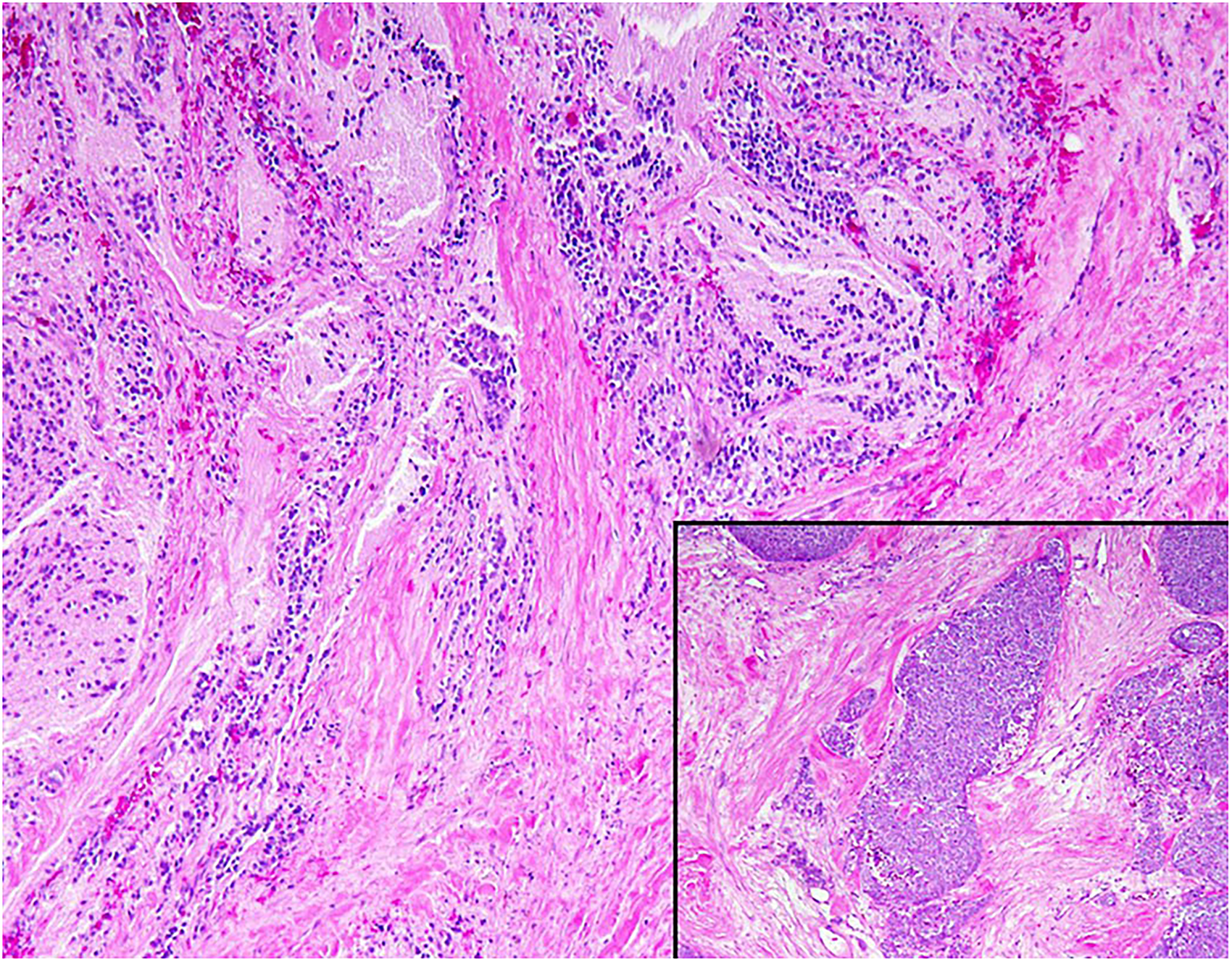
(a) Core biopsy of an anterior mediastinal mass composed of thymic epithelial neoplasm and germ cell tumor (H&E x 10); (b) closer examination shows that the thymic epithelial tumor is a thymoma consisting of bland epithelial cells with lymphocytic infiltrate (H&E x20); (c) the germ cell component is characterized by a mix of trophoblasts and syncytiotrophoblasts, consistent with choriocarcinoma (H&E x20); (d) immunohistochemical expression of keratin 5/6 in the thymoma component (x10) and (e) SALL4 (x10) and (f) beta human chorionic gonadotropin in the choriocarcinoma elements (x20).
Follow-up information available for three of the four patients revealed that two patients were alive and well without any additional treatment at 12 and 18 months, respectively, while the third patient developed tumor recurrence with pleural effusion after having received adjuvant chemotherapy for lymph node metastasis.35,37
Thymic Epithelial Neoplasms and Miscellaneous Tumors
In addition to the tumor categories discussed above, there are few reports of highly unusual composite tumors (Table 4). In one of these, the authors reported a thymic carcinoma closely admixed with neuroblastoma elements. 39 A small (1.2 cm), solid tumor was identified incidentally in the thymic gland of a 60-year-old man who was being investigated for ischemic heart disease. Microscopic examination of the resection specimen demonstrated a thymic carcinoma containing patchy clusters of cells dispersed in a pale pink fibrillary background. These cells had uniform, small, round nuclei with inconspicuous nucleoli and indistinct cytoplasm forming occasional pseudorosettes; mitotic activity and necrosis were absent (Figure 7a and b). Limited immunohistochemical analysis revealed that tumor cells of the thymic carcinoma component were positive for keratin and epithelial membrane antigen while the tumor cells of the second component were only positive for neuron-specific enolase. Together with the results of an electron microscopic study which demonstrated long, slender cytoplasmic processes and numerous membrane-bound, dense core neurosecretory granules in the latter, this tumor component was interpreted to represent neuroblastoma. Clinical follow-up was not provided for this patient, however, it was mentioned that in childhood, the patient had received radiation therapy to the thymic gland for undetermined reasons. 39
Thymic carcinoma with neuroblastoma component. The neuroblastomatous elements consist of clusters of small round blue cells embedded in a fibrillary stroma (H&E x10); the thymic carcinoma component shows nests of malignant thymic epithelial cells in a background of fibrotic stroma (inset) (H&E x 10).
More recently, a combined thymoma and salivary gland-type tumor (mucoepidermoid carcinoma) was reported. 40 The patient, a 51-year-old male, presented with clinical signs and symptoms of myasthenia gravis and was found to have a solitary, circumscribed anterior mediastinal mass. Preoperative fine needle aspiration of the mass confirmed a diagnosis of thymoma and thymectomy was performed. The gross specimen demonstrated an unencapsulated grey-red nodular mass measuring 5 cm in greatest dimension. Microscopically, two separate tumor components could be observed that showed no obvious areas of transition. While one component displayed the classic tumor morphology of a type B2 thymoma, the second one was composed of a mix of epidermoid cells, mucinous cells and intermediate cells. The latter showed bland cytologic features, no obvious mitotic activity and no necrosis. Immunohistochemically, the epidermoid cells were positive for keratin, keratin 5/6, keratin 7 and p63 while negative for CD5. Mucin-producing cells lacked reactivity for keratin 5/6 and p63. Based on tumor morphology and immunophenotype, this component was determined to represent a low-grade mucoepidermoid carcinoma and an overall diagnosis of combined thymoma-thymic mucoepidermoid carcinoma was rendered. Adjuvant chemotherapy and radiation to the surgical bed were administered and the patient was alive and well 12 months after the initial diagnosis. 40
Histogenesis
The pathogenesis of these combined tumors of the thymic gland remains largely undetermined. Various different pathways have been explored and several explanations have been offered: a) the presence of two distinct, simultaneous occurring tumors, so-called collision tumors; b) progressive loss of differentiation or dedifferentiation of one tumor component and resultant second component; c) emergence of or transformation of tumor components as the result of prior radiation or chemotherapy and d) differentiation of pluripotent thymic stem cells into a diverse tumor cell population.17,25,36,41–44 The latter theory seems to be favored by most investigators since it not only explains the presence of combined tumors of the same tumor cell lineage, such as thymoma and thymic carcinoma, but also the existence of unrelated tumors, for instance thymic epithelial neoplasms and germ cell tumors.
Special deliberations apply to the occurrence of thymic epithelial neoplasms in combination with lymphoma, especially those with T cell lymphoblastic leukemia/lymphoma. Here, malignant transformation of thymocytes is presumed to be a process through which such combined tumors may arise.34,45–47
Lastly, with respect to thymic epithelial neoplasms combined with multiloculated thymic cyst, two main theories exist and relate to the temporal relationship between the two components. In one, a pre-existing multilocular thymic cyst can induce tumor formation due to malignant transformation of its lining epithelium which is often seen in continuity with adjacent tumors. In another, the cystic changes of multiloculated thymic cyst are the result of an exaggerated hyperplastic/inflammatory response of the epithelium to tumor antigens with resultant cystic dilatation of Hassall corpuscles.48–50
Comment
Combined tumors of thymic origin are uncommon lesions. Due to their biphasic composition, the final diagnosis is often delayed until after surgical resection since small biopsies usually fail to sample both tumor components and clinical features are often the same as for pure tumors. Because of these challenges, treatment typically consists of surgical resection after which the combined nature of the tumor becomes apparent. Even more rarely, malignant transformation of one component can occur in a tumor recurrence. The outcome and prognosis of these tumors are difficult to predict due to the lack of sufficient data, however, it appears that survival is likely related to the more aggressive component. Extensive tumor sampling and careful microscopic examination is advised for all thymic neoplasms in order not to miss the presence of more than one tumor component. Once a combined tumor is diagnosed, the proportion of the individual components should be recorded so that any additional treatment can be tailored accordingly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Review article.
Trial Registration
Review article.