
Abstract
Mixed epithelial and stromal tumor (MEST) of the seminal vesicle is a rare biphasic neoplasm whose stromal component, while morphologically diverse, has not previously been reported to exhibit pseudoangiomatous stromal hyperplasia (PASH)-like change. We report a low-grade seminal vesicle MEST in a 70-year-old man in whom transrectal needle biopsy demonstrated prominent interanastomosing slit-like spaces within keloid-like collagen lined by bland spindle cells, without intraluminal erythrocytes—a pattern that raised concern for a vascular or sarcomatous neoplasm before the biphasic architecture was fully appreciated on the resection specimen. Immunohistochemically, the spindle cells showed a CD34+/CD31−/ERG− phenotype, supporting a myofibroblastic pseudovascular process rather than true endothelial differentiation. The patient remained recurrence-free for 19 years after complete excision. This observation expands the morphologic spectrum of seminal vesicle MEST and highlights a practical diagnostic challenge in biopsy interpretation. Recognition of PASH-like change, supported by targeted immunohistochemical evaluation, can help resolve the differential diagnosis and avoid overgrading in biopsy-limited settings.
Keywords
Introduction
Mixed epithelial and stromal tumor (MEST) of the seminal vesicle is a rare biphasic neoplasm that has historically been described under a variety of terms, including “phyllodes tumor” 1 and “Müllerian adenosarcoma-like tumor”. 2 In the current WHO classification, these lesions are recognized as a distinct entity, and their biologic potential is assessed mainly on the basis of stromal features, including atypia, mitotic figures, pleomorphism, and necrosis. 3 Reikie et al proposed a low-, intermediate-, and high-grade terminology for seminal vesicle MEST, while emphasizing that the precise distinction and nomenclature remain unsettled. 3 In that proposed framework, low-grade MEST lacks worrisome stromal features, including significant atypia, mitotic figures, and necrosis, with nuclear pleomorphism absent or at most focal and mild. 3 Even within this low-grade category, however, the stromal component may show variable morphologic patterns, including focal hypercellularity or myofibroblastic differentiation.3,4 Such variation may complicate interpretation, particularly in limited biopsy specimens in which the defining biphasic architecture is not fully represented.
Pseudoangiomatous stromal hyperplasia (PASH) is a benign myofibroblastic proliferation classically described in the breast and characterized by interanastomosing slit-like spaces that may mimic vascular channels. While PASH is uncommon outside the breast, rare instances have been documented in the anogenital region involving mammary-like glands and in the prostate.5,6 Furthermore, PASH-like stromal change is a recognized feature within breast fibroepithelial lesions, including fibroadenoma and phyllodes tumor. Against this background, it is plausible that a similar stromal pattern may occur in seminal vesicle MEST, another biphasic tumor with stromal differentiation, although such an association has not been documented to our knowledge.
Here, we report a seminal vesicle MEST with prominent PASH-like stromal change. This observation expands the morphologic spectrum of this rare tumor and illustrates a potential diagnostic challenge on needle biopsy, where pseudovascular stromal spaces may distract from the underlying biphasic nature of the lesion and raise consideration of a vascular or sarcomatous neoplasm. The 19-year recurrence-free follow-up further indicates that this unusual stromal pattern is compatible with indolent clinical behavior after complete excision. This manuscript was prepared in accordance with the CARE reporting guideline. 7
Patient Presentation
A 70-year-old man presented with general malaise. Imaging incidentally revealed a well-demarcated mass in the right seminal vesicle. He had no significant past medical history, and serum prostate-specific antigen was within the reference range (<4.0 ng/mL). Transrectal needle biopsy revealed glandular structures with slit-like lumina embedded in hyalinized to densely collagenous stroma accompanied by spindle cell proliferation. Focally, the stroma showed a cellular area and complex interanastomosing empty spaces within keloid-like collagen. These spaces lacked erythrocytes and were lined in part by bland spindle cells, imparting a pseudovascular appearance (Figure 1). Although no marked cytologic atypia or mitotic figures was identified, the limited sample precluded definitive classification and raised concern for a low-grade sarcoma, prompting radical cystoprostatectomy with seminal vesiculectomy.
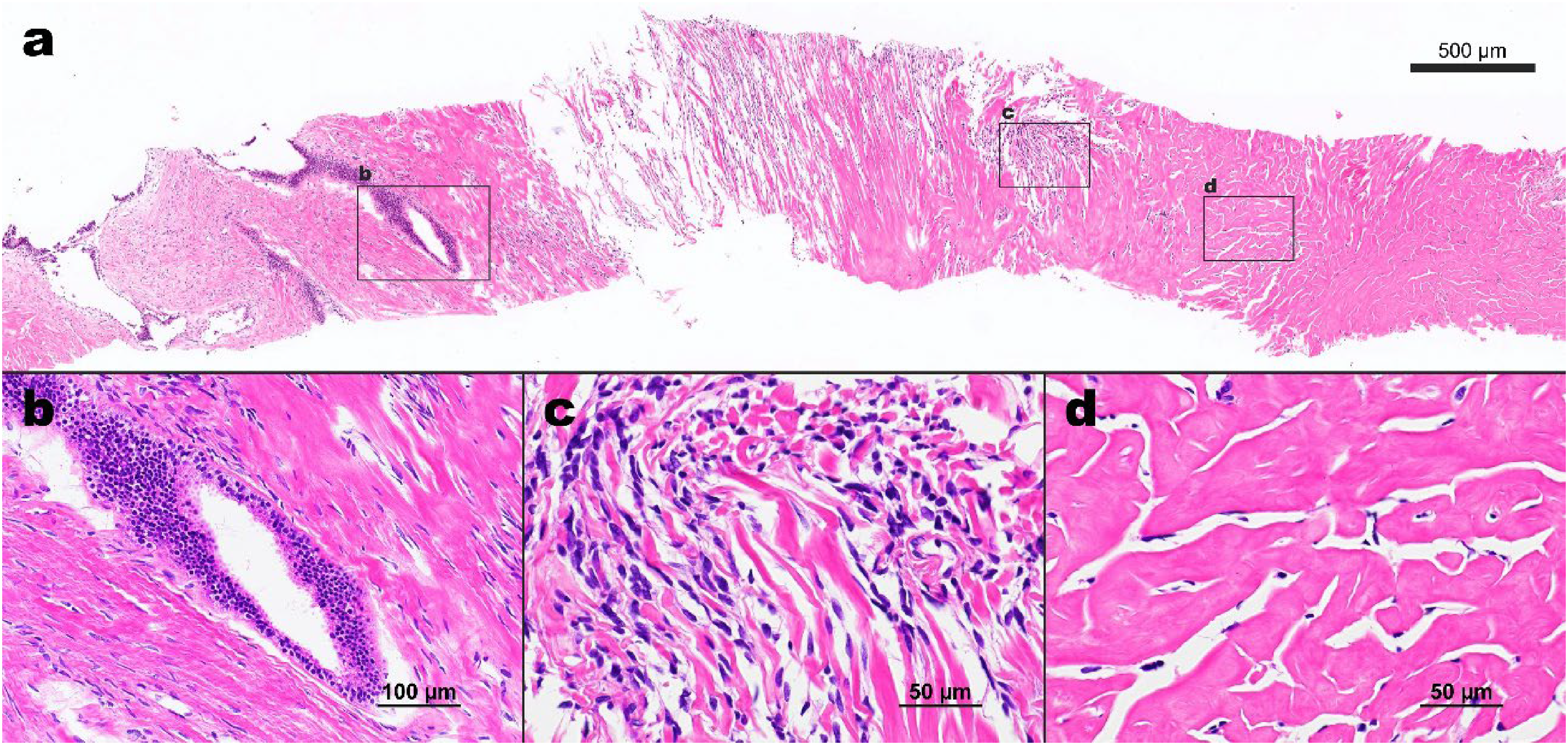
(a) Low-power view of the biopsy specimen, with boxed areas indicating the corresponding higher-power fields shown in (b–d) (hematoxylin and eosin stain; scale bar = 500 μm). (b) Higher-power view showing glandular structures with slit-like lumina accompanied by surrounding spindle cell proliferation (original magnification ×200; scale bar = 100 μm). (c) Cellular area composed of densely proliferating spindle cells without significant cytologic atypia or mitotic figures. (d) Complex interanastomosing empty spaces within dense collagenous, keloid-like stroma, some of which are lined by spindle-shaped myofibroblasts, mimicking endothelial lining. No erythrocytes are present within these spaces (c and d, original magnification ×400; scale bar = 50 μm).
Gross examination revealed a 4-cm, well-circumscribed lesion confined to the right seminal vesicle. The lesion formed an intracystic polypoid mass arising within a fibrous-walled cyst, and the cystic lumen was largely effaced. No gross extension into adjacent tissues was identified (Figure 2a).

(a) Horizontal cut surface of the resected specimen. The left seminal vesicle is indicated by an asterisk and the prostatic urethra by an arrowhead. The boxed area corresponds to the low-power view shown in (b) (scale bar = 1 mm). (b) Low-power view showing a mass filling the cystic lumen with a phyllodes-like surface configuration (scale bar = 2.5 mm). (c) Higher-power view of the tumor surface, demonstrating the phyllodes-like architecture. (d–g) High-power views of the same area showing bland bilayered epithelium and subjacent stromal hypercellularity. Basal cells are clearly highlighted by p63 (e), and the epithelial component is positive for PAX8 (f) and keratin 7 (g). (h–j) Another area showing transition from a hypercellular spindle cell proliferation in the upper left to a PASH-like area with dense keloid-like collagen in the lower right. The spindle cells are positive for CD34 (i) and negative for CD31 (j). (k–m) Higher-power views of the PASH-like area. Spindle-shaped myofibroblasts line empty slit-like spaces within dense collagenous stroma (k). These cells are positive for CD34 (l) and negative for ERG (m), whereas true capillaries serve as an internal positive control for ERG. (b–d, h, k), hematoxylin and eosin stain; (e), p63; (f), PAX8; (g), keratin 7; (i, l), CD34; (j), CD31; (m), ERG. Original magnification: (c, h–j), ×100; (d–g), ×600; (k–m), ×400.
Histologically, the tumor showed a biphasic architecture with polypoid, phyllodes-like epithelial projections into cystic spaces. The epithelium was bland and bilayered, consisting of luminal columnar cells and a p63-positive basal cell layer; the epithelial cells were positive for PAX8, keratin 7, and MUC6 and negative for AMACR (Figure 2d–g; Table 1). Beneath the epithelium, the stroma showed conspicuous subepithelial condensation with increased cellularity, merging into areas of dense collagenous, keloid-like stroma containing interanastomosing slit-like spaces. These spaces were lined by bland spindle cells with myofibroblastic morphology and lacked intraluminal erythrocytes. No significant cytologic atypia, mitotic figures, or tumor necrosis was identified (Figure 2b–d, h, k).
Immunohistochemical Findings and Antibody Details in the Epithelial and Stromal Components.
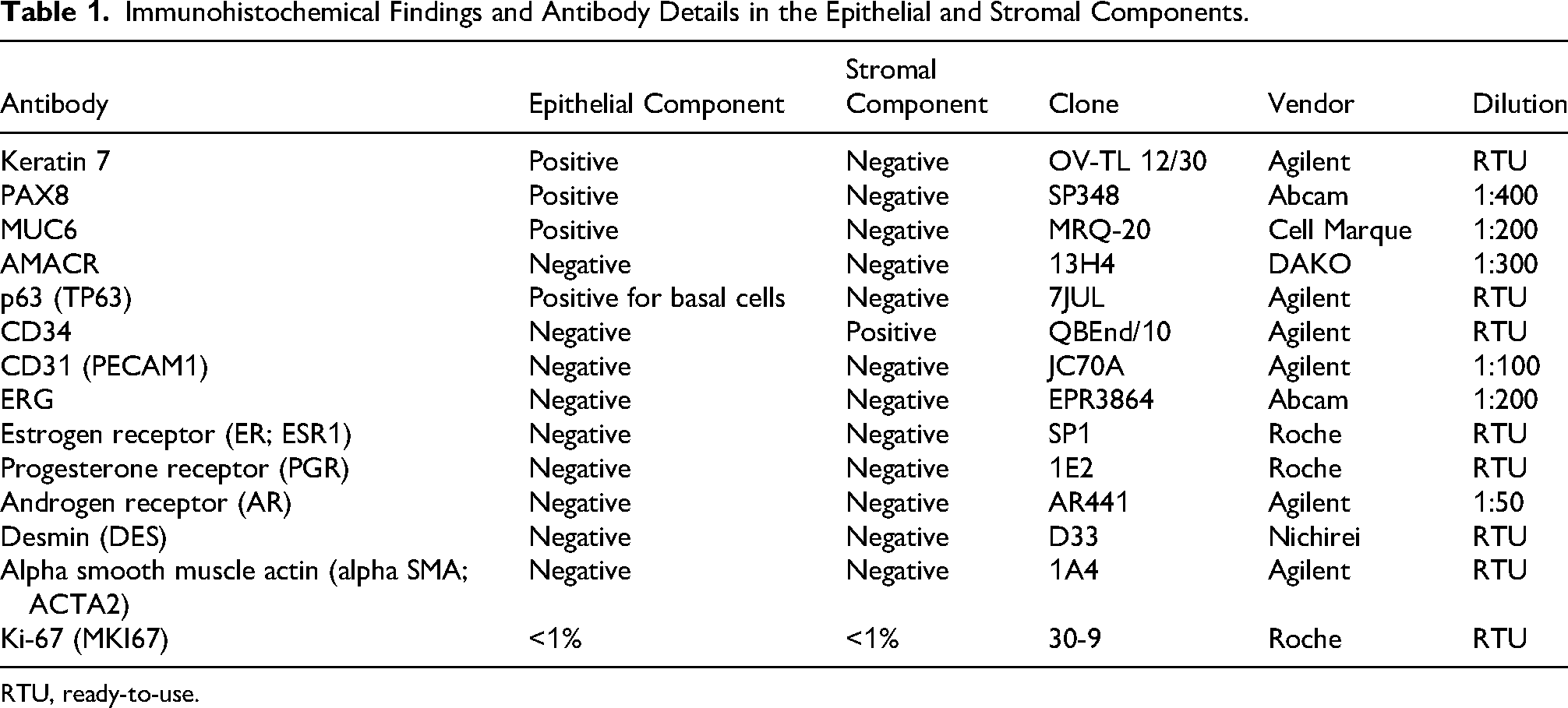
RTU, ready-to-use.
Immunohistochemically, the spindle cells lining the slit-like spaces were positive for CD34 and negative for CD31 and ERG, supporting a pseudoangiomatous rather than true vascular nature (Figure 2i, j, l, m; Table 1). The stromal cells were also negative for estrogen receptor (ER; ESR1), progesterone receptor (PGR), androgen receptor (AR), desmin, and alpha smooth muscle actin (alpha SMA) (Table 1). Surgical margins were negative. Given the absence of significant stromal atypia, mitotic figures, and tumor necrosis, the lesion was diagnosed as low-grade MEST of the seminal vesicle with prominent PASH-like change, according to the proposed criteria. 3
The postoperative course was uneventful. The patient underwent periodic follow-up for 19 years without evidence of local recurrence or distant metastasis, eventually dying of an unrelated cause.
Discussion
The present tumor broadens the morphologic spectrum of MEST of the seminal vesicle by demonstrating that its stromal component may show conspicuous PASH-like change. To our knowledge, such a stromal pattern has not previously been documented in seminal vesicle MEST. The significance of this observation is primarily practical. In a limited biopsy specimen, prominent pseudovascular slit-like spaces may distract from the underlying biphasic nature of the lesion and complicate interpretation, particularly when the diagnostic epithelial component is only scantily represented. At the same time, the 19-year recurrence-free course after complete excision indicates that even florid PASH-like change is compatible with indolent behavior in an otherwise low-grade seminal vesicle MEST.
Although PASH is most familiar as a benign myofibroblastic proliferation of the breast, its occurrence outside the breast is not without precedent. Extramammary PASH has been described predominantly in the anogenital region, where mammary-like glands are present. 5 In organs lacking such structures, however, the pattern appears to be distinctly uncommon. Of particular relevance, a PASH-like lesion has been reported in the prostate, 6 indicating that this morphology can arise in the male genitourinary tract. In addition, PASH-like stromal change is a recognized, albeit uncommon, finding in breast phyllodes tumors, where it may partially obscure the characteristic fibroepithelial architecture and create a pseudovascular impression. 8 Taken together, these observations suggest that PASH-like myofibroblastic change is not restricted to conventional mammary tissue but may emerge in biphasic or fibroepithelial-type tumors across different anatomic sites.
From a developmental perspective, the occurrence of such a pattern in the seminal vesicle is biologically plausible. During male embryonic development, the caudal Müllerian mesenchyme contributes to the formation of the prostate and adjacent periprostatic tissues, resulting in a developmentally heterogeneous stromal milieu.9,10 This background may help explain why lesions arising in the male periprostatic region can occasionally exhibit morphologic features reminiscent of Müllerian or mammary-type stromal proliferations. In the present tumor, therefore, the PASH-like appearance is unusual but not inexplicable, and may be understood as one possible manifestation within the wider morphologic range of stromal differentiation in seminal vesicle MEST.
The absence of stromal hormone receptor expression in the present tumor requires interpretation in two related but distinct contexts: PASH-like stromal change and seminal vesicle MEST. With respect to PASH-like change, this finding does not preclude the diagnosis. Although earlier studies emphasized strong progesterone receptor expression in breast PASH, 11 more recent data indicate that hormone receptor expression is substantially variable, with ER and PGR positivity reported in only 29% and 34% of breast PASH lesions, respectively. 12 With respect to seminal vesicle MEST, however, the absence of ER and PGR is unusual. Previously reported seminal vesicle MESTs with available immunohistochemical data have generally shown stromal ER and PGR expression, supporting the concept of hormone-responsive Müllerian-type stroma in this tumor family.3,13 Nevertheless, hormone receptor expression has not been established as a required diagnostic criterion for seminal vesicle MEST, and even in renal MEST—the setting in which hormone receptor-positive ovarian-type stroma is best characterized—stromal PGR and ER expression is common but not universal, reported in 85% and 73% of tumors, respectively, in the largest series. 14 Accordingly, the ER/PGR/AR-negative phenotype in the present tumor is best regarded as an atypical immunophenotypic finding within an otherwise morphologically characteristic seminal vesicle MEST with PASH-like stromal change, rather than as evidence against either interpretation. Interestingly, the previously reported prostatic PASH-like lesion also lacked PGR expression, 6 suggesting that PASH-like lesions in the male genitourinary tract may not fully reproduce the hormone receptor profile classically associated with breast PASH.
The principal diagnostic issue arose not from the resection specimen, but from the biopsy. The transrectal needle biopsy captured stromal hypercellularity and interanastomosing slit-like spaces within dense collagenous stroma, but did not adequately sample the defining biphasic architecture of MEST. In that setting, a pseudovascular spindle-cell lesion naturally entered the differential diagnosis. Angiosarcoma is the most important consideration because of its potentially serious clinical implications; however, several features argued strongly against that diagnosis, including the absence of intraluminal erythrocytes, the lack of significant cytologic atypia, the absence of mitotic figures, and the CD34+/CD31−/ERG− immunophenotype. Solitary fibrous tumor may also be considered because of its collagenous background and frequent CD34 positivity, but it does not characteristically produce the complex pseudoangiomatous slit-like spaces seen here, and would typically be expected to show nuclear STAT6 expression. Mammary-type myofibroblastoma, another benign CD34-positive spindle-cell neoplasm that may occur in the periprostatic region, likewise lacks the distinctive anastomosing pseudovascular spaces and, crucially, lacks the epithelial component that defines MEST. Thus, the diagnostic problem was not that PASH-like change is intrinsically impossible to recognize, but rather that in a biopsy with incomplete architectural sampling, it may transiently divert attention toward vascular or sarcomatous lesions until the broader biphasic context is established. This point is clinically relevant, because biopsy of seminal vesicle masses is often limited in its ability to permit definitive classification. 15 In the present patient, that preoperative uncertainty likely contributed to the decision to proceed with radical resection.
The long-term outcome of the present patient provides useful clinical perspective. Seminal vesicle MESTs classified as low grade under the proposed framework generally appear to pursue a favorable course after complete excision, although the available data remain limited and recurrence has been documented, particularly in incompletely resected lesions.3,13,15 From a single observation, it would be inappropriate to infer that PASH-like stromal change has independent prognostic significance. Similarly, observations from breast fibroepithelial lesions suggesting that PASH may be associated with less aggressive stromal features cannot be directly extrapolated to seminal vesicle tumors.8,16 Nevertheless, the present patient's clinical course does show that conspicuous PASH-like change, even when florid, does not in itself imply aggressive biologic behavior. In that respect, awareness of this pattern may help avoid overinterpretation of pseudovascular stromal change in limited samples.
This study has several limitations. Molecular analysis could not be performed because the formalin-fixed paraffin-embedded material was more than 20 years old at the time of review. In addition, original digital images were unavailable because of PACS migration. These constraints limit further biologic characterization of this unusual stromal pattern. Even so, the combination of distinctive morphology, a consistent immunophenotypic profile, and an exceptionally long recurrence-free follow-up provides sufficient grounding for the morphologic and clinical conclusions drawn.
In summary, PASH-like stromal change may occur in seminal vesicle MEST and further expands the morphologic spectrum of this rare biphasic tumor. Its greatest relevance lies in biopsy interpretation: when only a limited portion of the lesion is sampled, the pseudovascular stromal pattern may raise consideration of vascular or other spindle-cell neoplasms before the underlying biphasic architecture becomes apparent. Careful morphologic assessment—specifically, the recognition of interanastomosing empty slit-like spaces lined by bland myofibroblasts within keloid-like collagen, without intraluminal erythrocytes—together with a targeted immunohistochemical panel confirming a CD34+/CD31−/ERG− phenotype, is sufficient to resolve this differential diagnosis and avoid diagnostic overgrading. The present patient's long-term clinical course further suggests that this unusual stromal pattern is compatible with indolent clinical behavior after complete excision.
Footnotes
Acknowledgments
The authors thank Emi Shuhara for assistance with locating and retrieving archival paraffin blocks and glass slides from the hospital's basement archives.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and institutional guidelines for case reporting. Ethical approval was waived by the Ethics Committee of Kyoto University Hospital because this is a de-identified case report.
Consent to Participate
Not applicable.
Consent for Publication
The patient was deceased at the time of manuscript preparation, and the next of kin could not be contacted despite reasonable efforts. In accordance with institutional policy, the requirement for informed consent for publication was waived. All clinical information and images were fully de-identified.
Author Contributions
Ayaka Fukui did writing the original draft and investigation. Yuki Teramoto performed conceptualization, visualization, investigation, writing—review and editing, supervision, and project administration. Nanako Izumi and Masahiro Hirata did methodology, Writing—review and editing. Hironori Haga did supervision and writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are not publicly available, as they contain information derived from patients. However, the data are available from the corresponding author upon reasonable request.