
Abstract
Primary middle ear meningiomas are exceptionally rare extracranial tumors, often misdiagnosed due to their nonspecific clinical and radiological features. Accurate diagnosis requires histopathological and immunohistochemical confirmation to distinguish them from common middle ear pathologies. We present a 59-year-old male patient with a 2-year history of intermittent right ear otorrhea and conductive hearing loss. Imaging revealed middle ear opacification with ossicular erosion, prompting surgical excision. Histopathology confirmed primary meningioma, and postoperative follow-up showed no recurrence. Literature review of relevant studies was conducted to summarize clinical and histopathological characteristics of primary middle ear meningioma.
Keywords
Introduction
Meningiomas are benign, slow-growing tumors that originate from the meningothelial cells of the meninges, accounting for 18% of primary intracranial tumors. 1 While most meningiomas are intracranial, rare examples have been reported in ectopic locations such as the paranasal sinuses, parotid gland, skin, and even extracranially, where they represent only 2% of all meningiomas. Among these, involvement of the middle ear is extremely uncommon. 2 Intracranial meningiomas can extend into the middle ear via structures such as the tegmen tympani, posterior fossa plate, internal auditory canal, or jugular foramen. Historically, many tumors initially believed to be primary middle ear meningiomas were later found to have intracranial origins, particularly before the widespread availability of gadolinium-enhanced magnetic resonance imaging (MRI).3–5
We report an exceptionally rare occurrence of an isolated, primary middle ear meningioma confirmed by MRI. This highlights the importance of advanced imaging techniques in accurately diagnosing and distinguishing primary extracranial meningiomas. A review of relevant literature highlights the unique features, diagnostic challenges, and treatment considerations associated with these tumors.
Patient Presentation
A 59-year-old male patient, known to have diabetes mellitus, dyslipidemia, hypertension, mild non-obstructive coronary artery disease, and mild aortic stenosis, presented with a 2-year history of intermittent right ear otorrhea. The patient denied associated ear pain, hearing loss, dizziness, or ear fullness, nor did he have history of previous ear surgeries. Examination of the left ear revealed an intact external auditory canal and tympanic membrane, while the right ear exhibited two polyps obstructing the external auditory canal, obscuring visualization of the tympanic membrane (Figure 1). Audiological assessment and tympanometry were conducted as part of the work up (Figure 2).
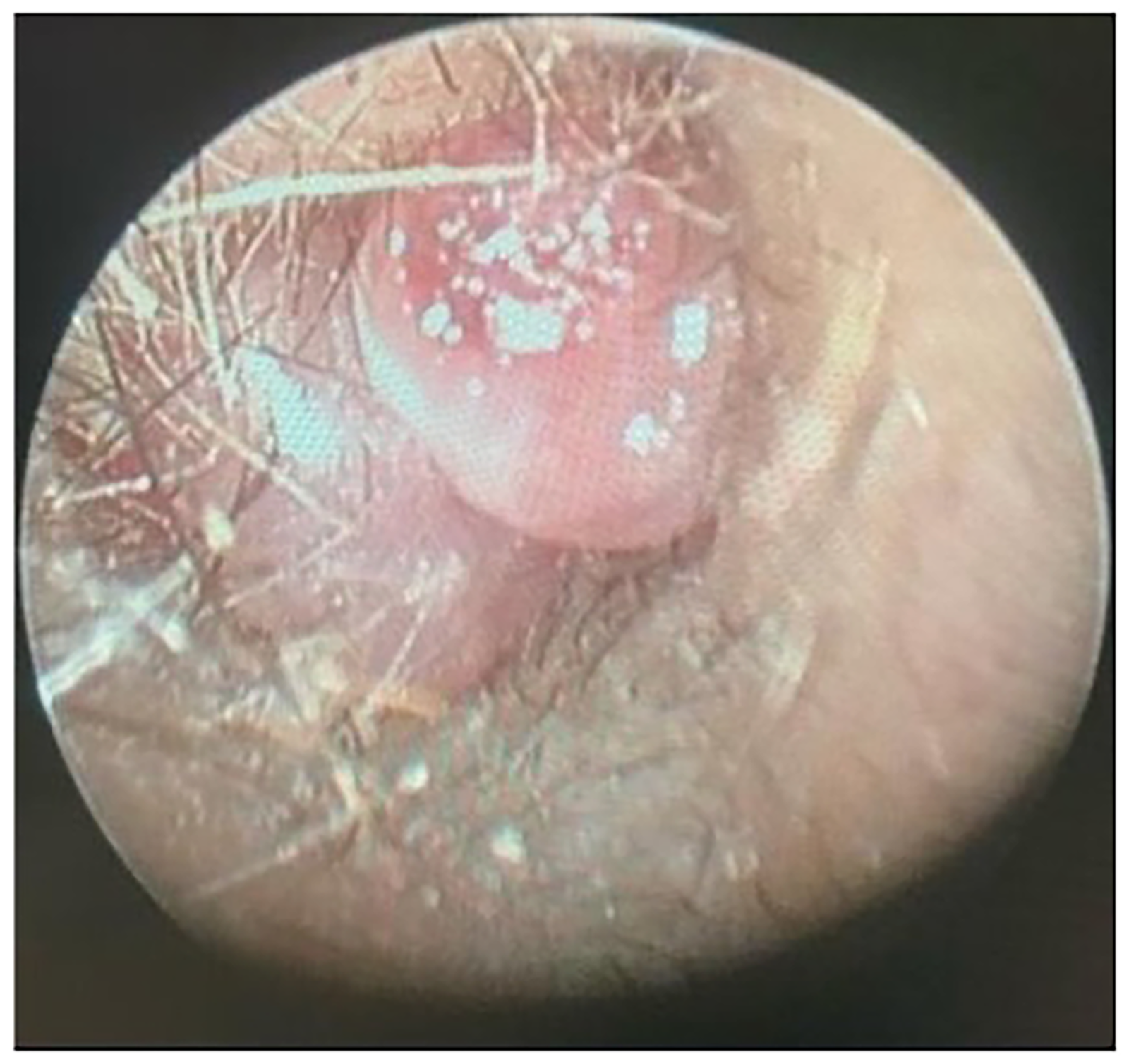
Endoscopic picture of the right ear showing 2 aural polyps obstructing the external auditory canal, obscuring visualization of the tympanic membrane.
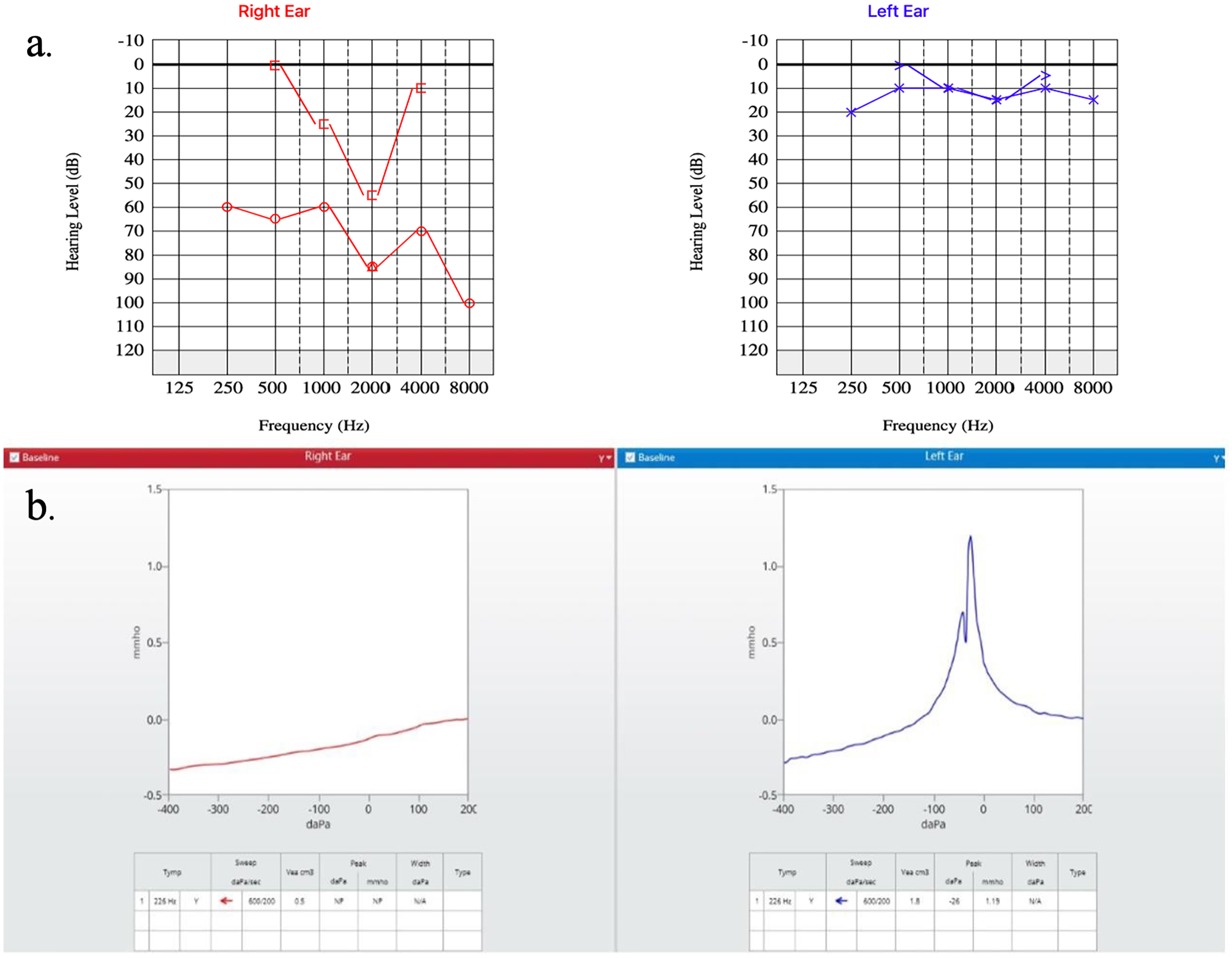
(a) Patient's audiogram showing conductive hearing loss in the right ear. (b) Type B curve in the right ear on tympanogram.
A biopsy of the right ear lesion taken the previous year suggested an inflammatory otic polyp. Subsequent temporal bone computed tomography (CT) demonstrated complete opacification of the right mastoid air cells, antrum, and middle ear cavity, with a polypoid density extending to the outer ear (Figure 3). The findings were associated with ossicular and scutum erosion and bony wall involvement of the external auditory canal, raising concerns for cholesteatoma, polypoid lesions, or a primary epithelial neoplasm. The patient subsequently underwent surgical excision of the mass.
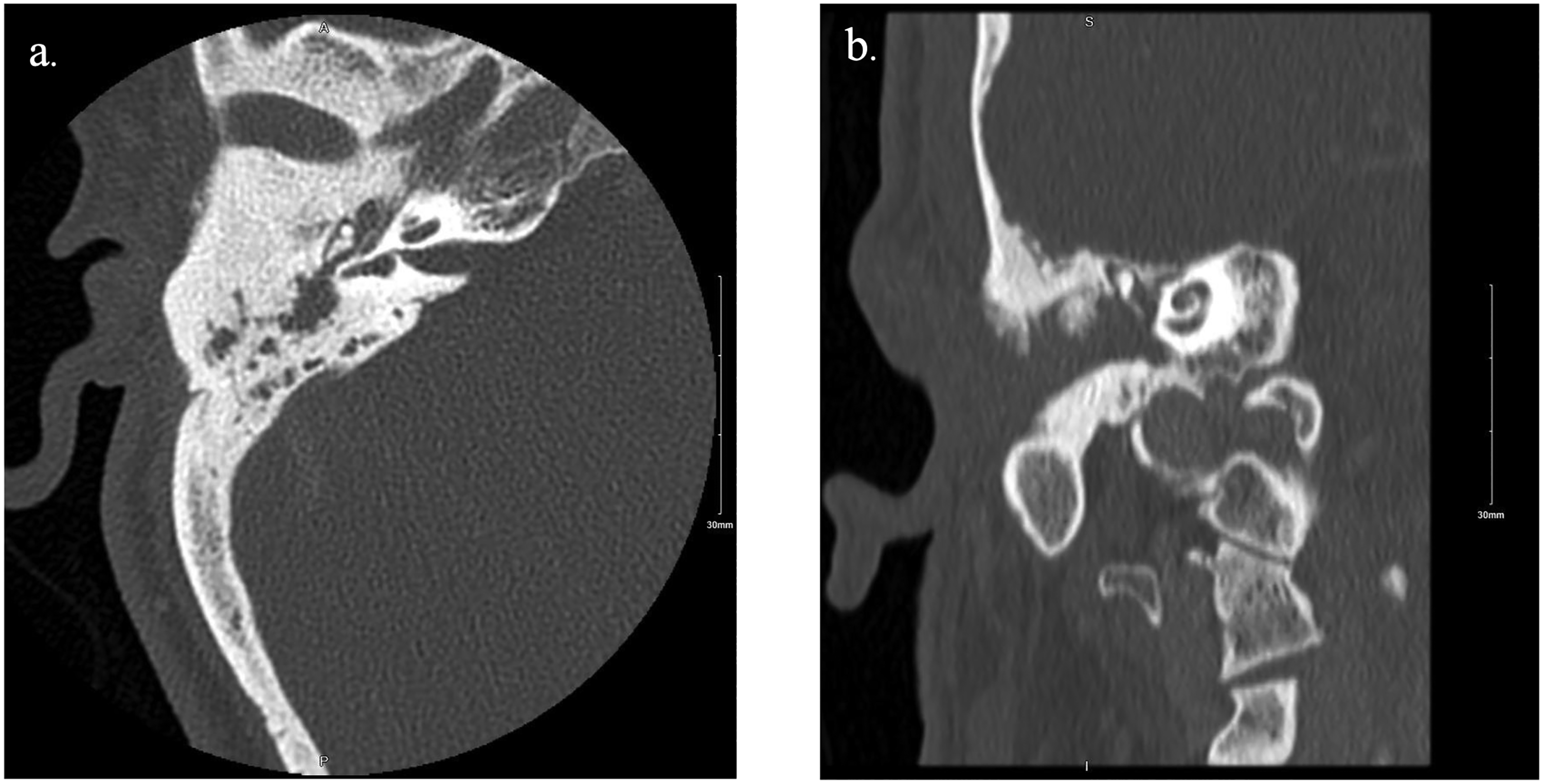
(a) Showing complete opacification of the right mastoid air cells, antrum, and middle ear cavity. (b) Complete opacification of the external auditory canal along with ossicular and scutum erosion.
Surgical intervention, including right external auditory canal polyp removal and middle ear exploration (tympanomastoidectomy), was performed. Intraoperatively, extensive polyps filled the external auditory canal, with a posterior tympanic membrane perforation and granulation tissue occupying the middle ear cavity. Minimal keratin was observed in the sinus tympani, facial recess, and posterior otic area. Ossicular examination showed intact and mobile malleus and stapes, but complete erosion of the incus. After meticulous excision of the lesions, temporalis fascia was used for tympanic membrane reconstruction.
Postoperative recovery was uneventful, with no complications. The patient remained stable and reported resolution of otorrhea in subsequent follow-up visits.
In the laboratory, the specimen consisted of a polypoid, tan, soft tissue fragment. Microscopic examination showed fibrous stroma lined by squamous epithelium and containing a neoplasm composed of nodular aggregates with focal infiltrative areas of cells exhibiting eosinophilic cytoplasm and fairly uniform round to ovoid nuclei, many of which contained intranuclear pseudoinclusions (Figures 4, 5, and 6). No mitotic figures or necrosis were identified. On immunohistochemistry, the tumor cells were positive for epithelial membrane antigen (EMA) and progesterone receptor (PR) (Figure 7). The lesional cells were negative for GFAP, desmin, chromogranin A, synaptophysin, CD56, S100, GATA3, pan keratin, CAM5.2, keratin 7, keratin 20, CD31, and ERG. The morphologic and immunohistochemical findings confirmed the diagnosis of meningioma. 6 The lesion was identified in histologic samples from both the middle ear and the external auditory canal.
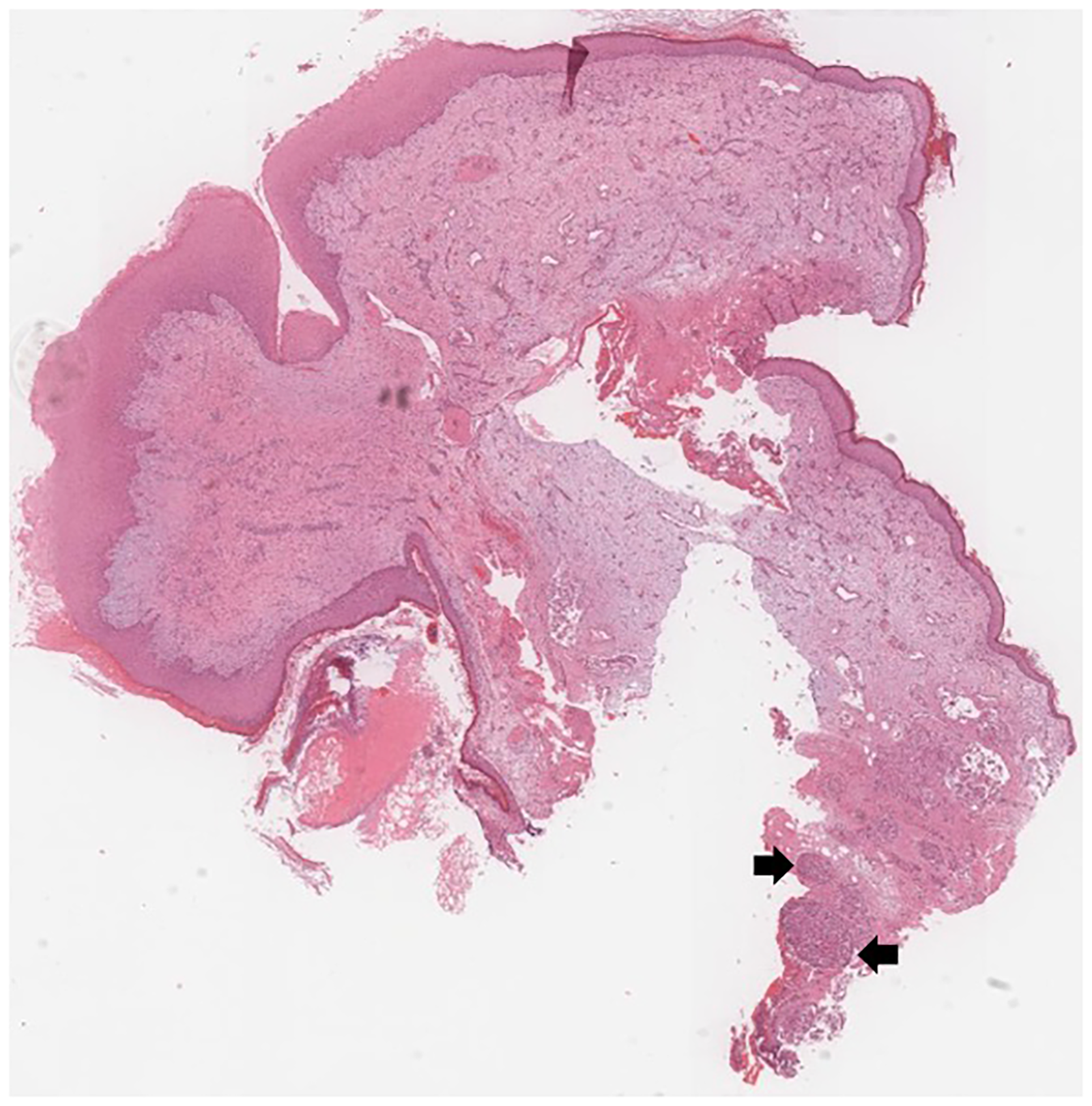
Squamous epithelium-lined polyp showing nodular aggregates of meningioma cells in the deeper part of the stroma (arrow) (hematoxylin and eosin stain, panoramic view).
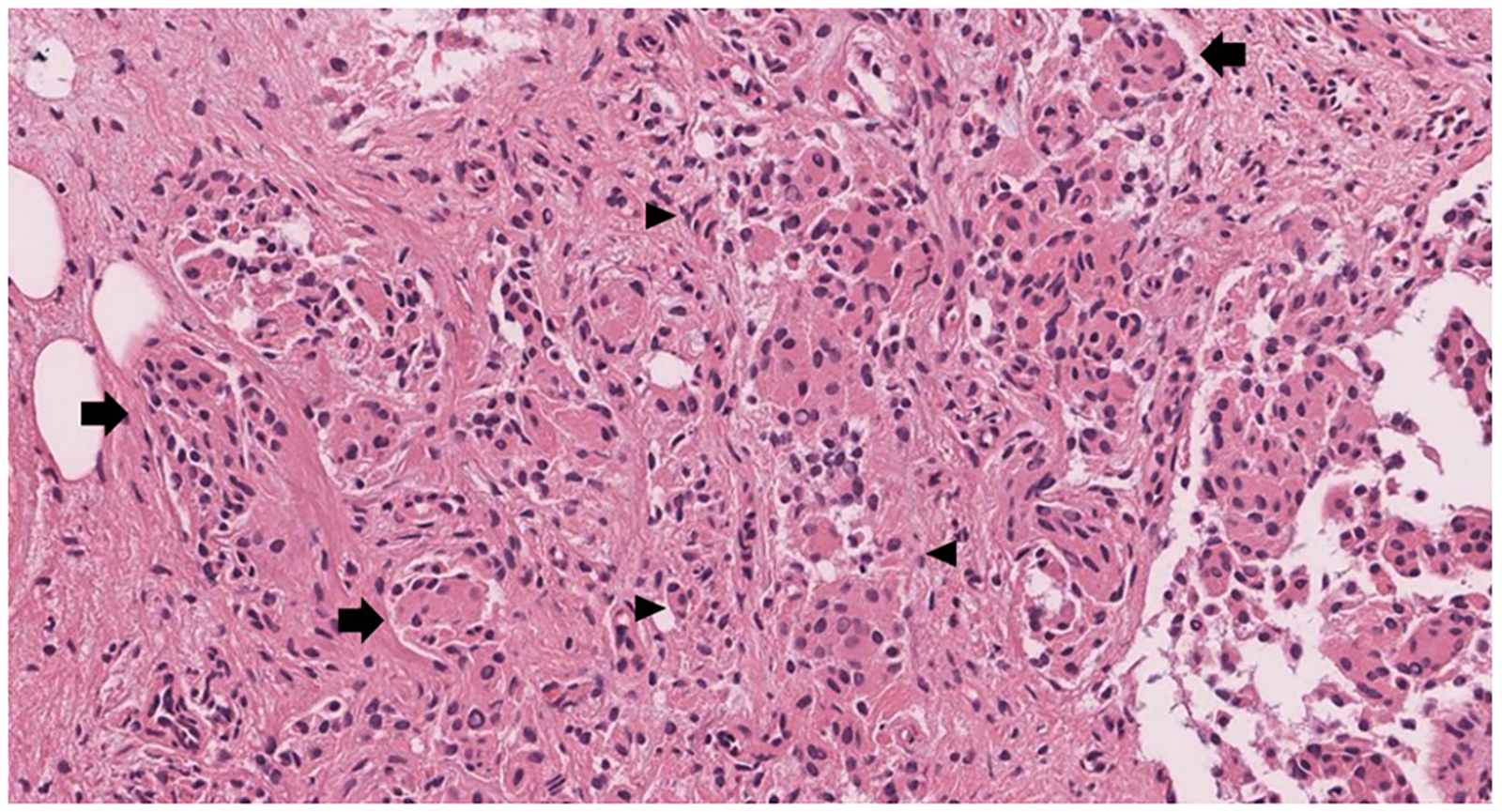
The lesion (meningioma) is formed of nodular aggregates (arrow) and some infiltrative foci (arrowhead) of fairly uniform cells (hematoxylin and eosin stain, ×20).
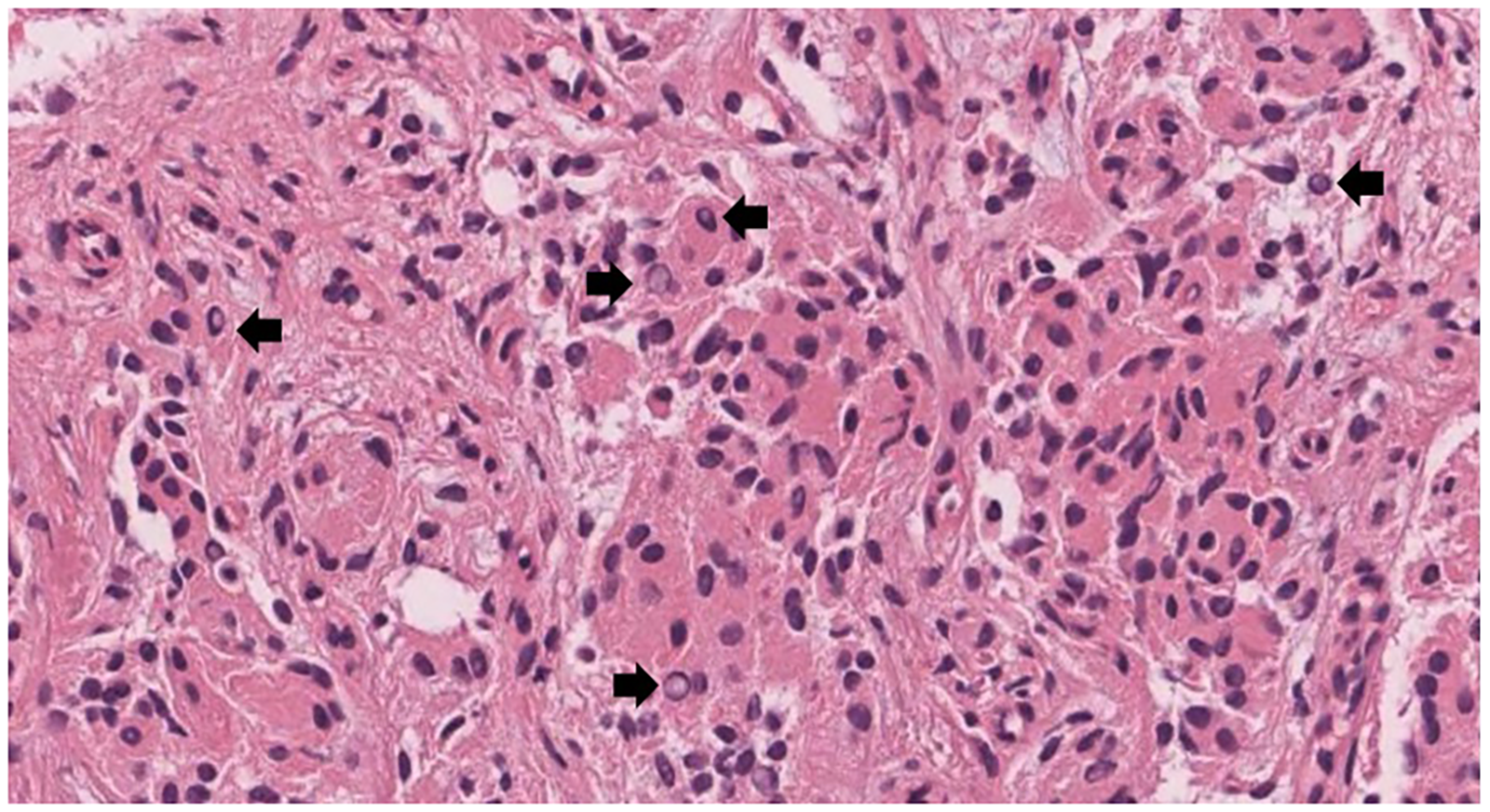
The meningioma cells have eosinophilic cytoplasm and fairly uniform round to ovoid nuclei. Intranuclear pseudoinclusions are seen (arrow) (hematoxylin and eosin stain, ×40).
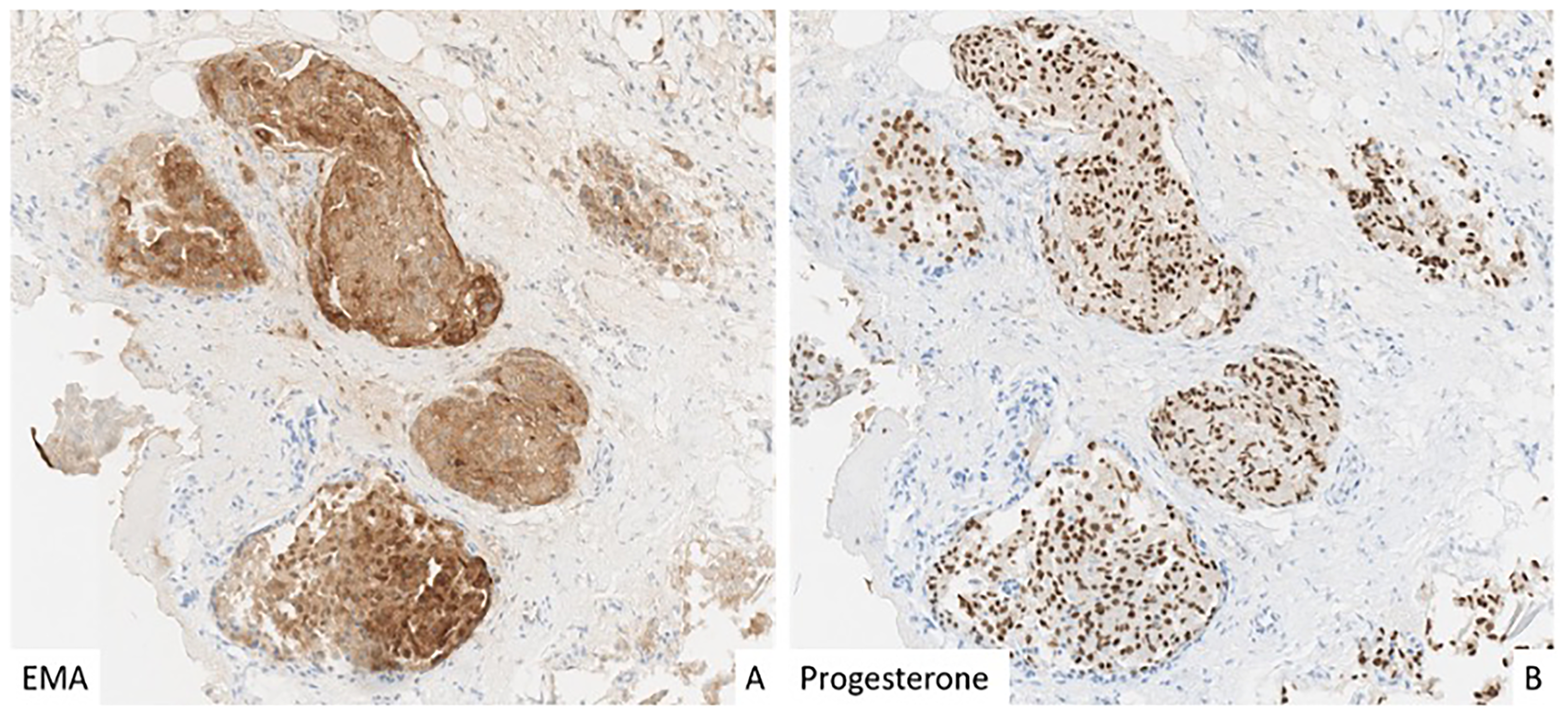
The cells of meningioma are positive for EMA (cytoplasmic, A) and progesterone receptors (nuclear, B) (immunohistochemical stains).
During follow-up, the patient experienced persistent surgical site numbness and mild tympanic membrane perforation, with stenosis in the right external auditory canal. Despite these findings, he continued to report no pain, discharge, dizziness, tinnitus, or aural fullness.
Discussion
Middle ear meningiomas are usually a presentation of primary intracranial meningioma with middle ear involvement. However, primary middle ear meningioma is an exceptionally rare clinical entity, characterized by nonspecific clinical and radiological features, with only a limited number of tumors documented in the literature. These two types can be appreciated in Nager's classification of temporal bone meningiomas. 7 Accurate diagnosis requires histopathological and immunohistochemical analyses to differentiate it from more common middle ear tumors, such as schwannomas and glomus tympanicum. Enhanced awareness among otolaryngologists is critical for identifying this uncommon but well-documented tumor.
Due to the rarity of the disease and the nonspecific clinical presentation, middle ear meningiomas are usually misdiagnosed. Many patients are initially thought to have otitis media with effusion and are mistreated accordingly. 8 Others, like the one presented here, were diagnosed as an epithelial polyp pre-histological confirmation. 9 Patients may or may not also present with hearing loss. If so, conductive or mixed hearing loss have been published in previous studies.10,11
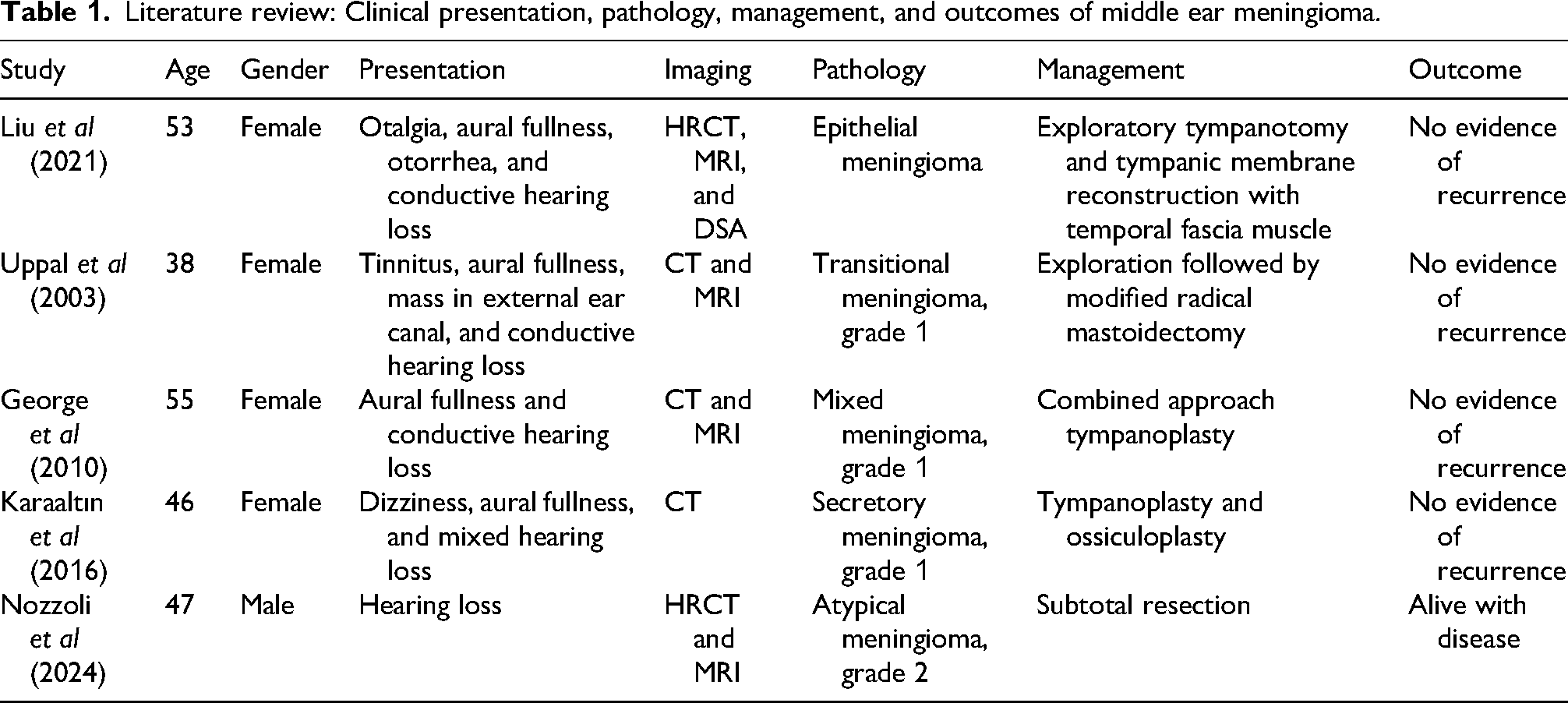
Generally, reported examples in the literature of ectopic middle ear meningioma have been benign (grade 1) and /or with favorable outcomes. However, Nozzoli et al reported an atypical middle ear meningioma, WHO grade 2, with hematoxylin and eosin slides and immunohistochemistry supporting their findings (Table 1). 12
Literature review: Clinical presentation, pathology, management, and outcomes of middle ear meningioma.
Long-term surveillance with gadolinium-enhanced MRI is strongly advised to monitor for potential recurrence, which remains a possibility even after complete surgical excision. Meningiomas are believed to originate from meningothelial cells of neural crest origin. The development of extracranial meningiomas is hypothesized to result from the migration of meningothelial cells through anatomical structures such as the tegmen tympani, posterior fossa plate, and jugular foramen. 13 MRI plays a pivotal role in excluding concurrent intracranial meningiomas, which may coexist with extracranial lesions. 14 Despite advances in understanding, the exact mechanisms underlying tumor formation in ectopic locations remain poorly defined, with current evidence suggesting that ectopic meningiomas may arise from displaced meningothelial cells.
Footnotes
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). According to our institutional policy, Institutional Review Board (IRB) approval is not required for single-patient case reports. Therefore, formal ethical approval was waived.
Authors’ Contribution
Conception and design were done by AAk, AAs, AJAa, MK, YA.
Administrative support was accomplished by MK, YA.
Provision of study materials or patients was done by AAk, AAs, AJAa.
Collection and assembly of data were done by AA, AJAs, MB.
Data analysis and interpretation were done by AJAs, MB, AK, AMA.
Manuscript writing and final approval of manuscript were done by all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.