
Abstract
Malignant adenomyoepithelioma is an adenomyoepithelioma in which the epithelial or myoepithelial components may undergo malignant transformation. Malignant adenomyoepithelioma of the breast is a rare tumor and often affects elderly women. We report an 85-year-old female patient who presented with 5.5 cm mass in the outer quadrant of the left breast. Biopsy of the mass showed metaplastic spindle cell carcinoma. The patient then underwent a total mastectomy. The final pathology found malignant adenomyoepithelioma and in addition, coexisted with well-differentiated invasive ductal carcinoma. The findings raised an interesting discussion of potential pathogenesis, the implications in clinical management and emphasized the importance of extensive tissue sampling in large breast tumors.
Introduction
Malignant adenomyoepithelioma is a rare breast neoplasm characterized by the malignant transformation of the luminal epithelial and/or myoepithelial components of a pre-existing adenomyoepithelioma. 1 It predominantly affects elderly women, with an average age of around 60 years. 2 Clinically, it often presents as a solitary, palpable mass ranging from 1 cm to 17 cm. 3 When malignant transformation involves the epithelial component, it may resemble invasive carcinoma of no special type or, rarely, metaplastic carcinoma. 4 To the best of our knowledge, this is the first report of a malignant adenomyoepithelioma coexisting with a well-differentiated invasive ductal carcinoma within a single tumor mass. This report aims to analyze the distinct histological and immunohistochemical features of these two components, discuss the differential diagnosis, and explore potential insights into the pathogenesis of epithelial-myoepithelial tumors.
Case Report
An 85-year-old female patient with advanced dementia and a history of Stage IV non-Hodgkin lymphoma (treated more than 20 years ago) presented with a left breast mass, and it measured approximately 7 × 5 cm by ultrasound. A core needle biopsy revealed an infiltrative spindle cell lesion with eosinophilic cytoplasm, moderate to severe nuclear atypia, and frequent mitotic figures. Immunohistochemistry showed the spindle cells were positive for P63 (weakly) but negative for keratins (AE1/AE3, CAM 5.2, 5/6). Estrogen receptor (ER), progesterone receptor (PR), and HER2 were negative.
The patient underwent a left simple mastectomy without a sentinel lymph node biopsy given patient's age and comorbidities. Gross examination of the specimen revealed a 5.5 × 5 × 4.5 cm firm, tan-white, fibrous mass. Microscopically, the tumor was predominantly composed of malignant spindle cells focally admixed with a biphasic papillary neoplasm (measuring 15 mm) exhibiting necrosis and microcalcifications, consistent with malignant adenomyoepithelioma (Figures 1–3). The malignant spindle cells measured 55 mm and infiltrated the adjacent skeletal muscle. Incidentally, a 3 mm focus of well-differentiated invasive ductal carcinoma was identified approximately 3.5 mm adjacent to the malignant spindle cell component (Figures 4 and 5), along with a 3 mm focus of ductal carcinoma in situ (Figure 6).
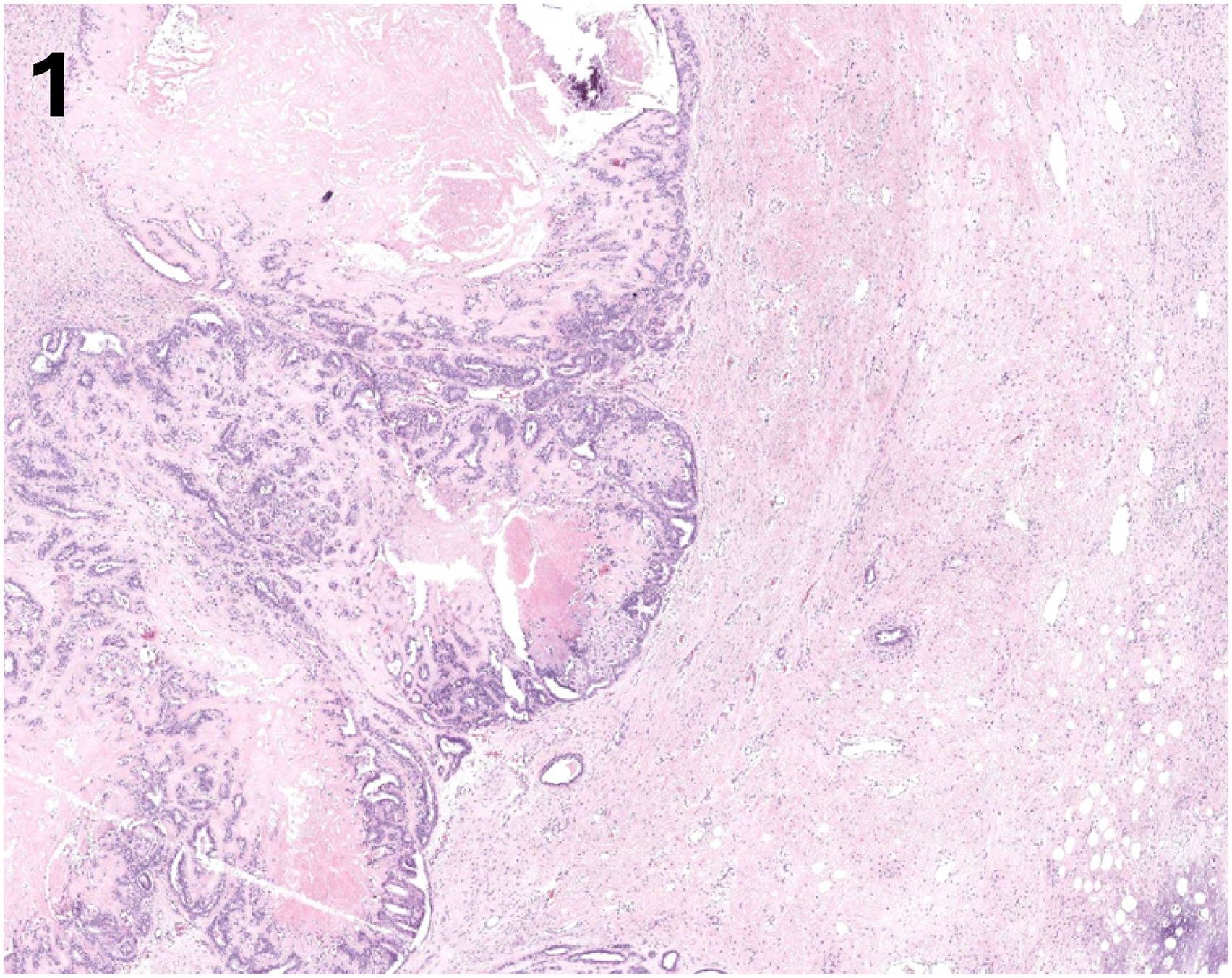
Low power (H&E, x20). It shows biphasic papillary neoplasm with necrosis and calcification.
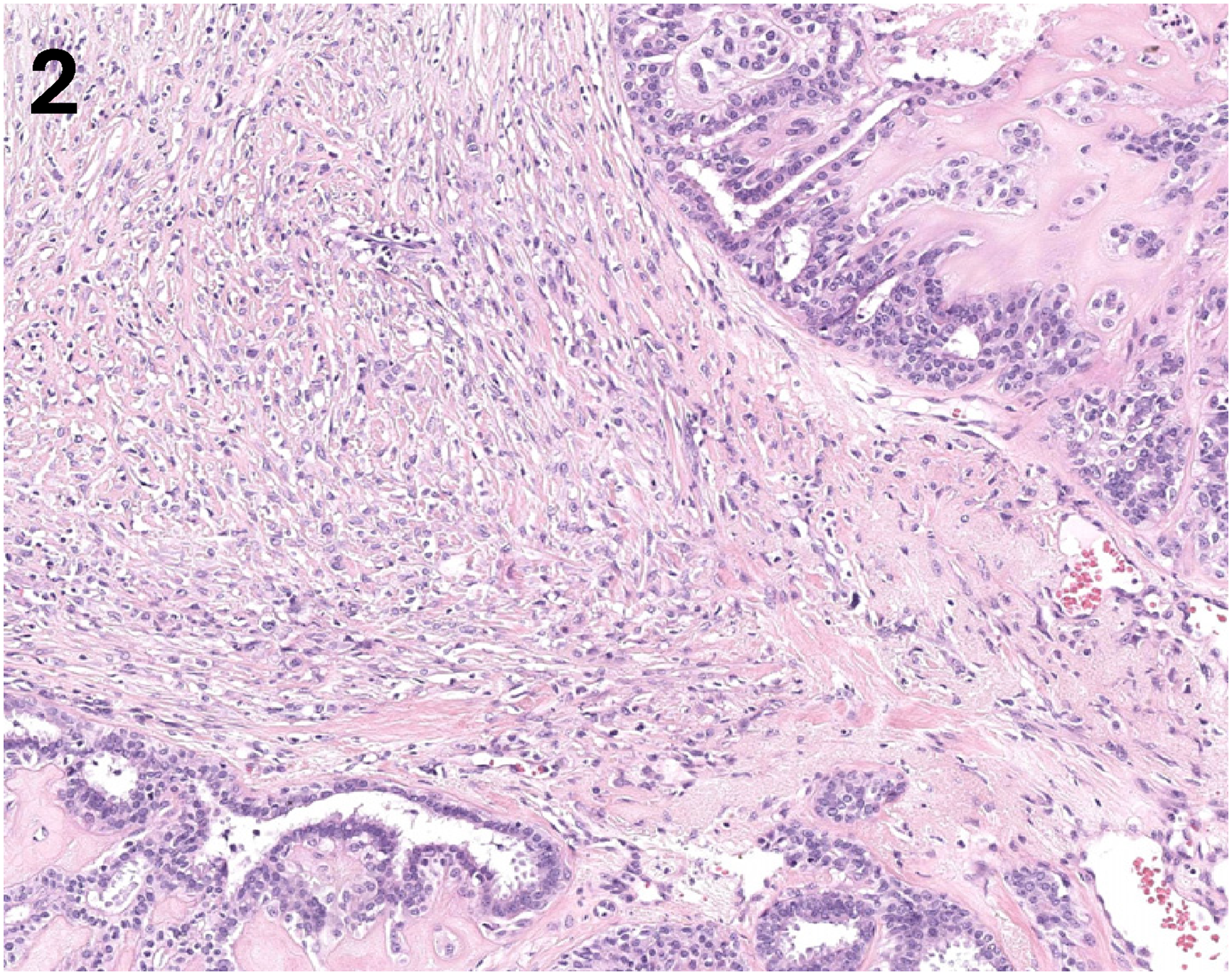
High power (H&E, x100) shows transition from biphasic papillary neoplasm to malignant spindle cell lesion.
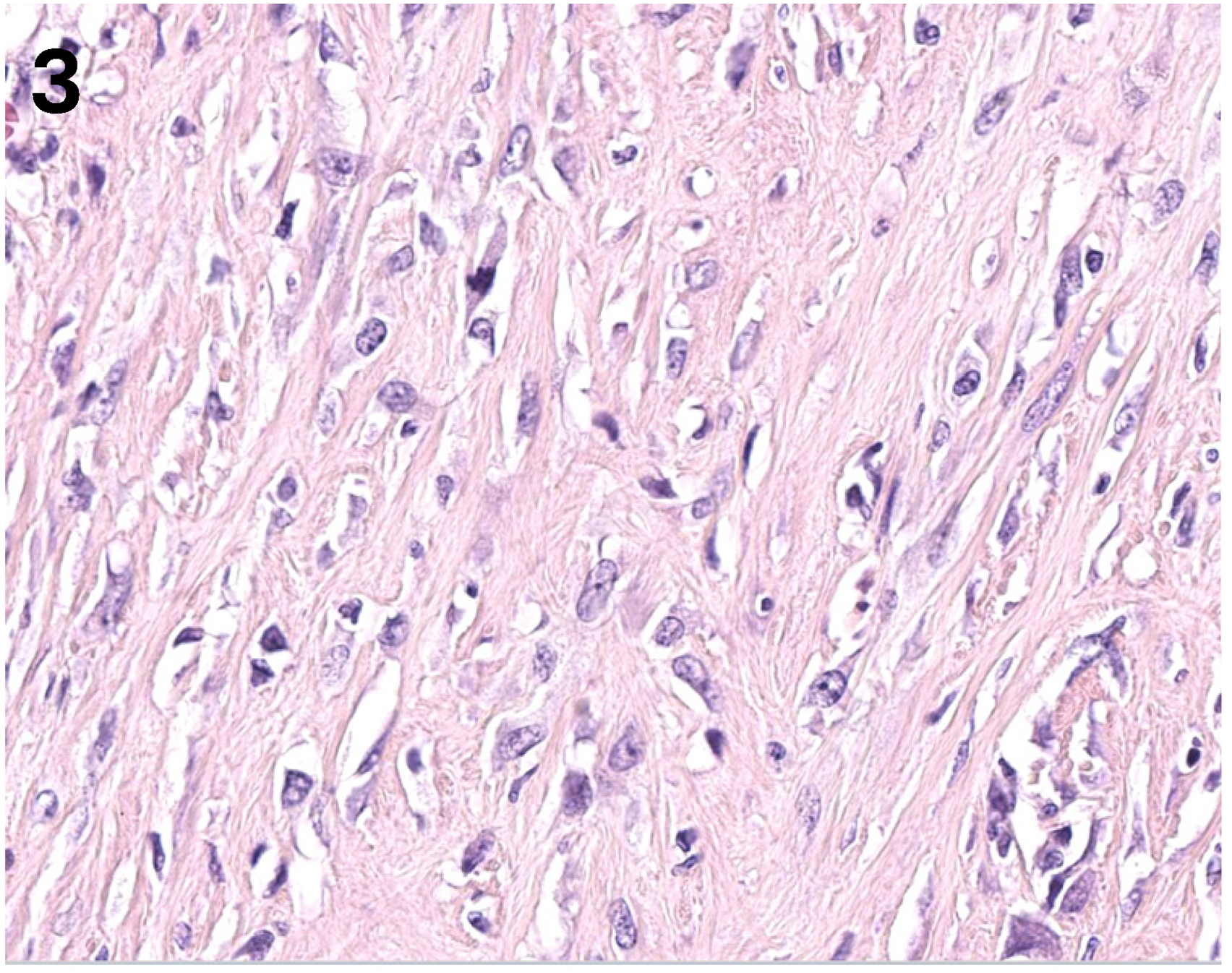
High power (H&E, x400) view of the malignant spindle cell component showing marked nuclear atypia and mitotic figures.
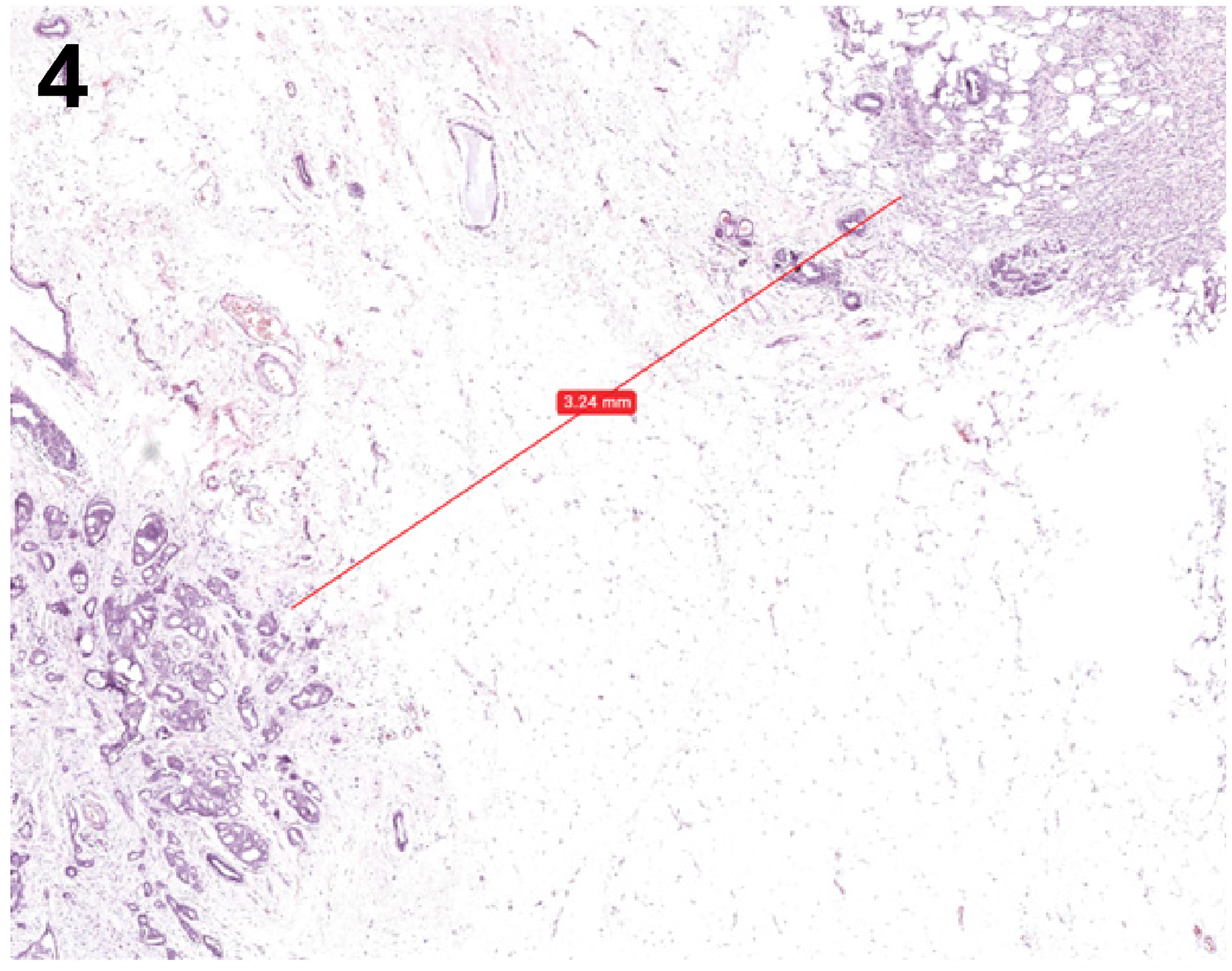
Low power (H&E, x20): the separate focus of well-differentiated invasive ductal carcinoma located approximately 3 mm from spindle cell carcinoma.
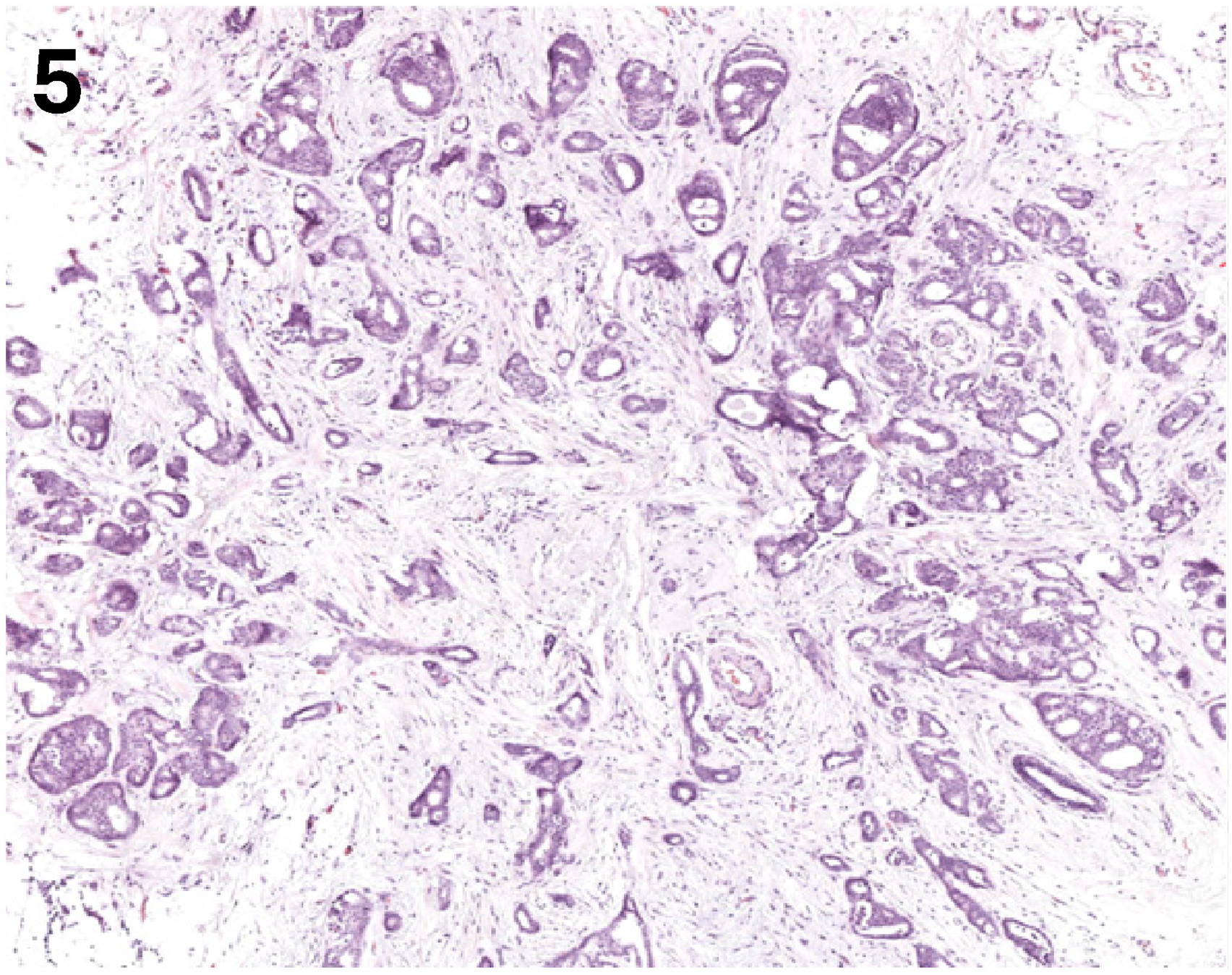
Low power (H&E, x40): the separate focus of well-differentiated invasive ductal carcinoma measures 3 mm.
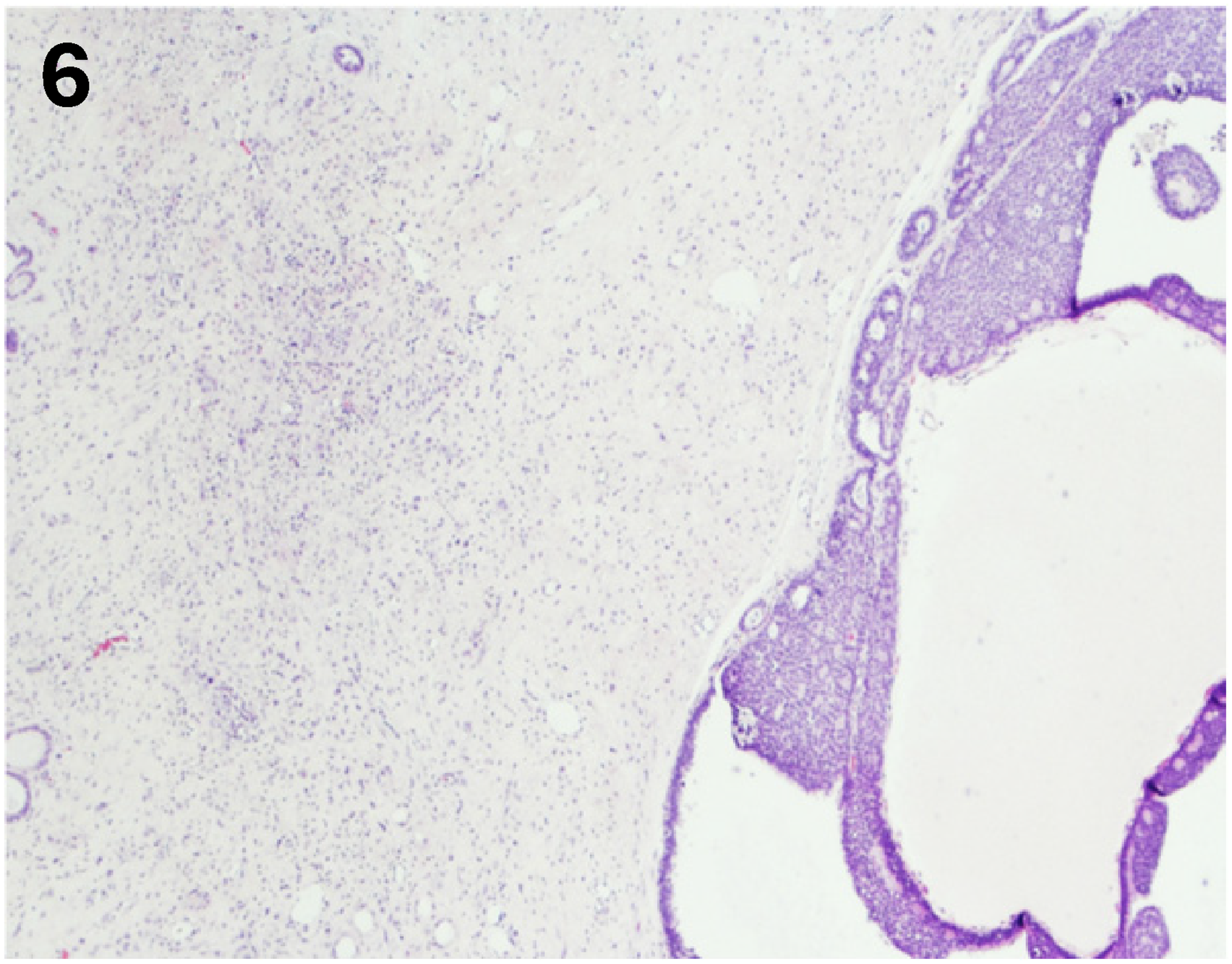
Low power (H&E, x20): a focus of ductal carcinoma in situ (DCIS) located next to spindle cell carcinoma.
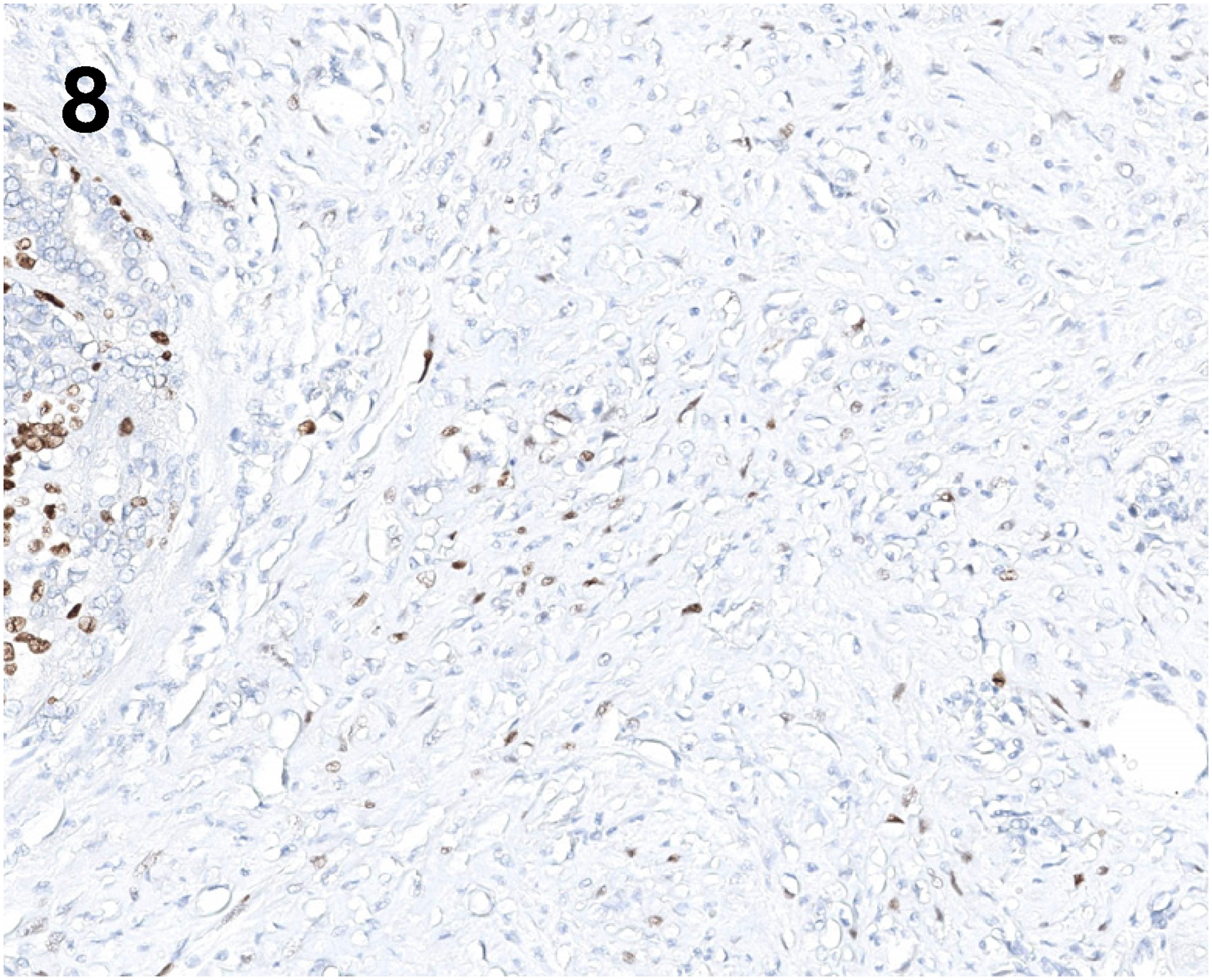
Immunohistochemical stains on the mastectomy specimen confirmed that the spindle cell (metaplastic) carcinoma component was positive for S100 and P63 (weak), while negative for SOX10, CD10, and keratins (AE1/AE3, CAM 5.2, 5/6) (Figures 7–12). Repeat biomarker testing on the spindle cell (metaplastic) carcinoma component confirmed it was negative for ER, PR, and HER. In contrast, the separate focus of well-differentiated invasive ductal carcinoma was strongly positive for ER (>90%), strongly positive for PR (>90%) (Figure 13), and negative for HER2. Immunostain for p53 was performed, and the malignant spindle cell and adenomyoepithelioma showed wild-type staining pattern (Figure 14). Given the patient's comorbidities, no further adjuvant treatment was administered.
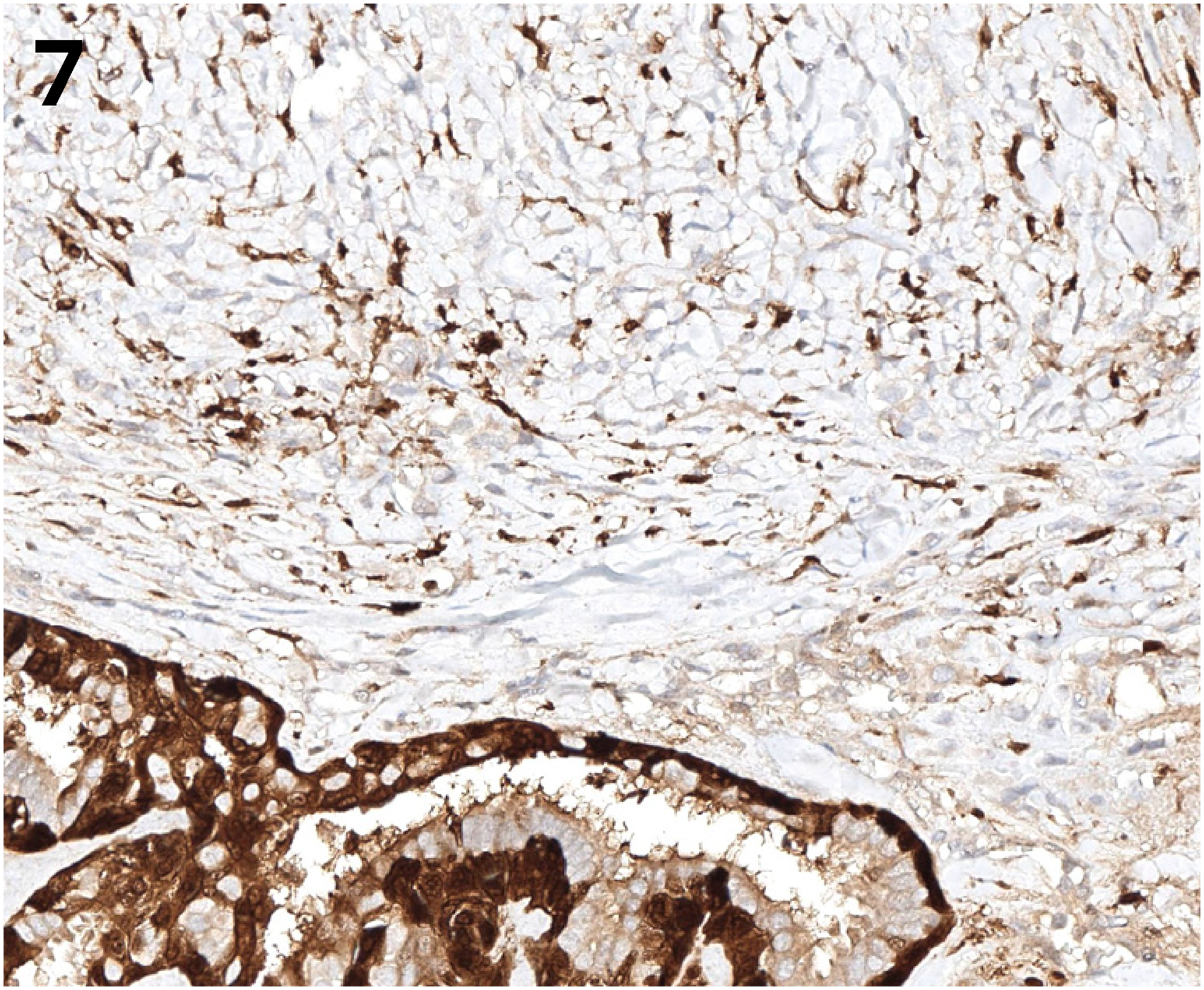
Immunochemical for S100 staining (x 200) in the malignant spindle cell component. The myoepithelial component in adenomyoepithelioma is also highlighted.
Immunochemical for P63 staining (x 200) in the malignant spindle cell component. The myoepithelial component in adenomyoepithelioma is also highlighted.
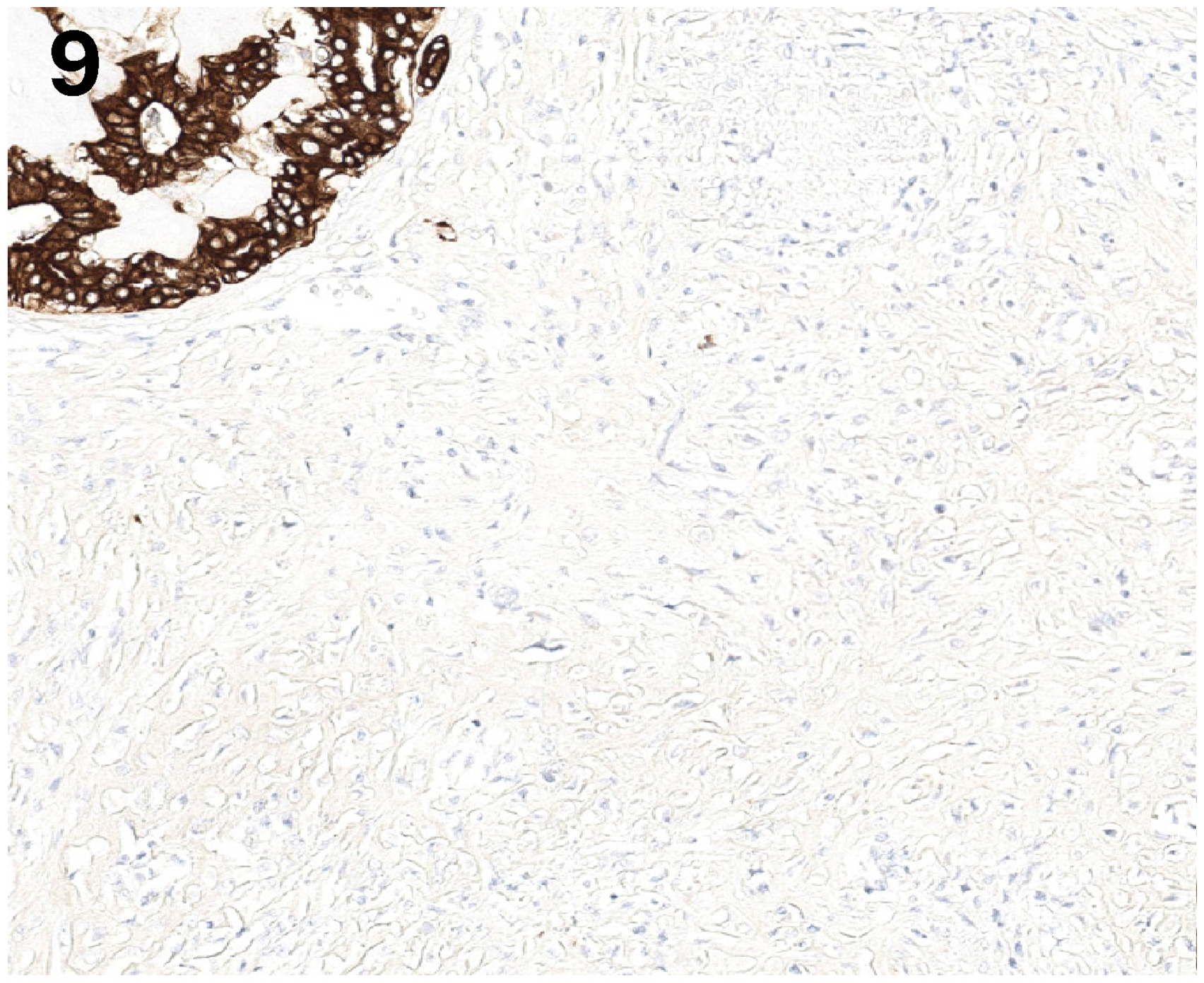
Immunochemical for keratin AE1/AE3 staining (x 200) is negative in the malignant spindle cell component.
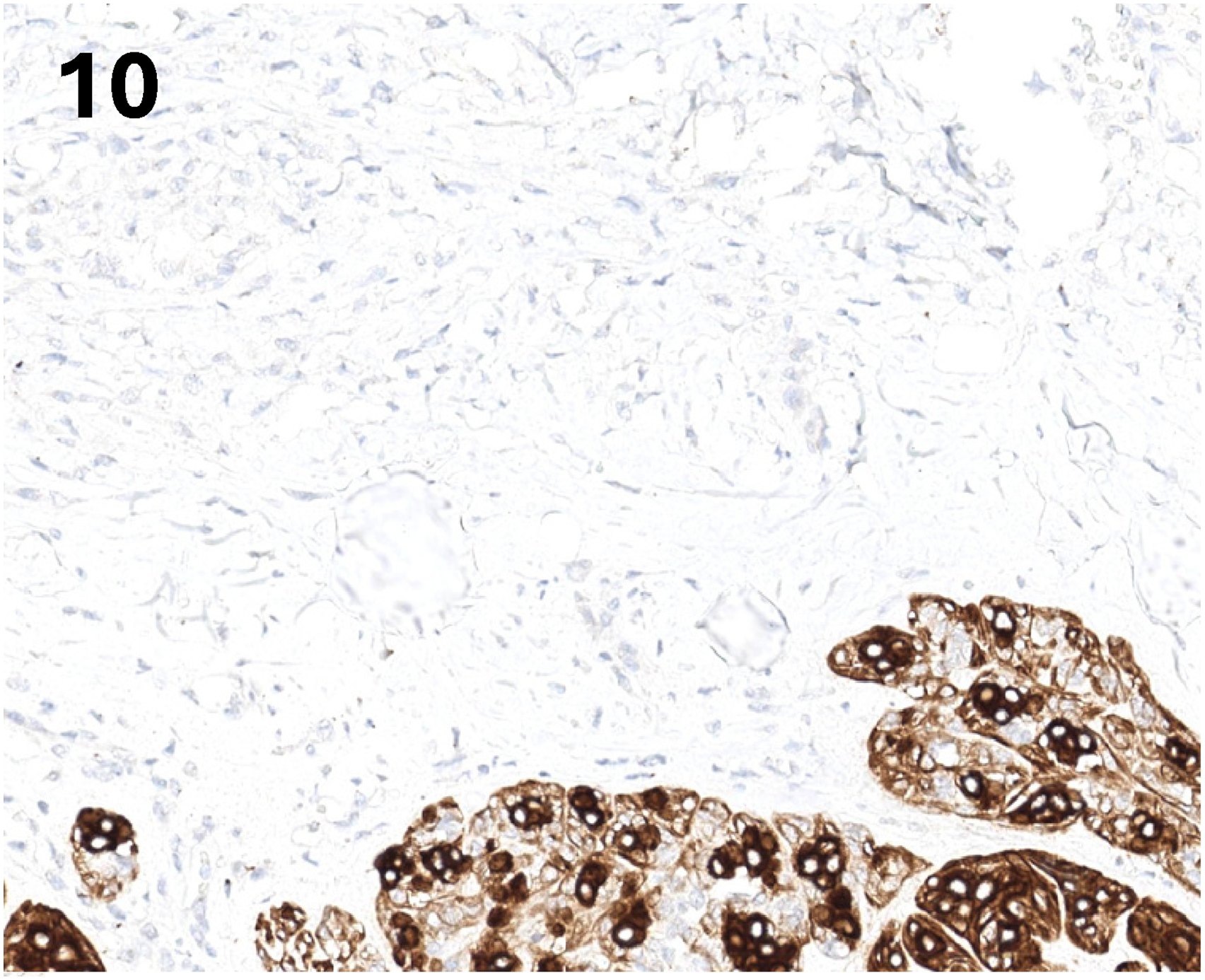
Immunochemical for keratin CK5/6 staining (x 200) is negative in the malignant spindle cell component.
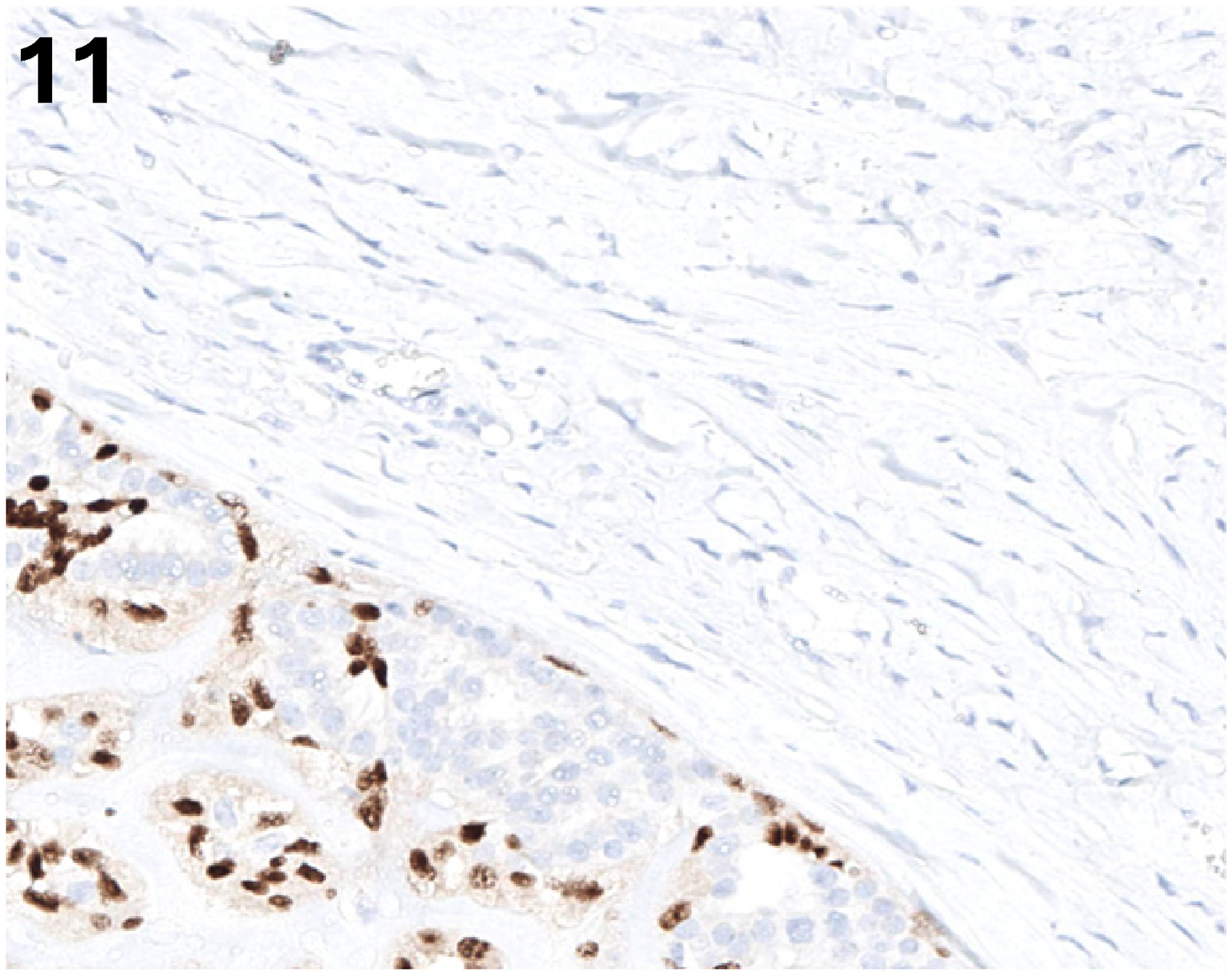
Immunochemical for keratin SOX10 staining (x 200) is negative in the malignant spindle cell component.
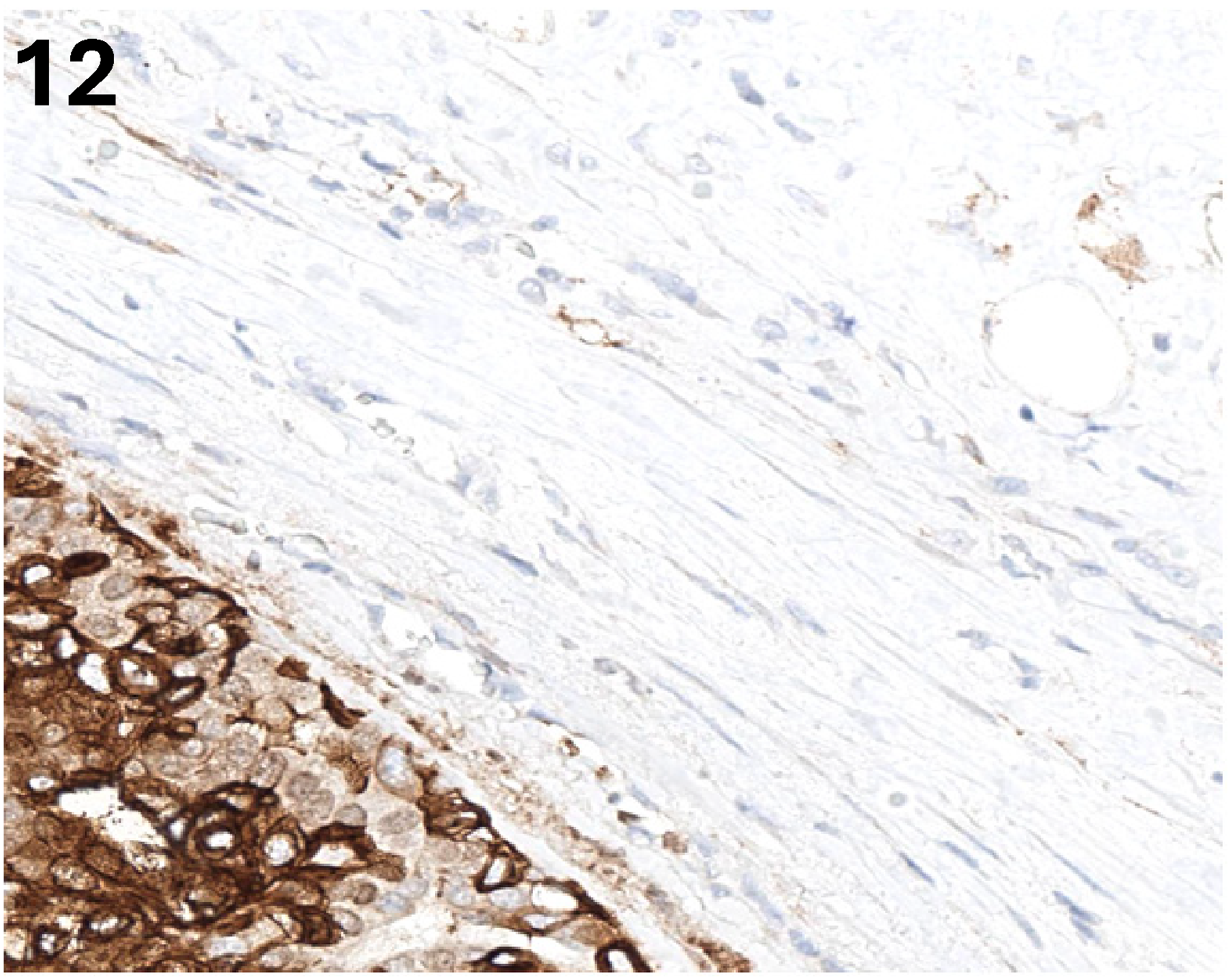
Immunochemical for keratin CD10 staining (x 200) is negative in the malignant spindle cell component.
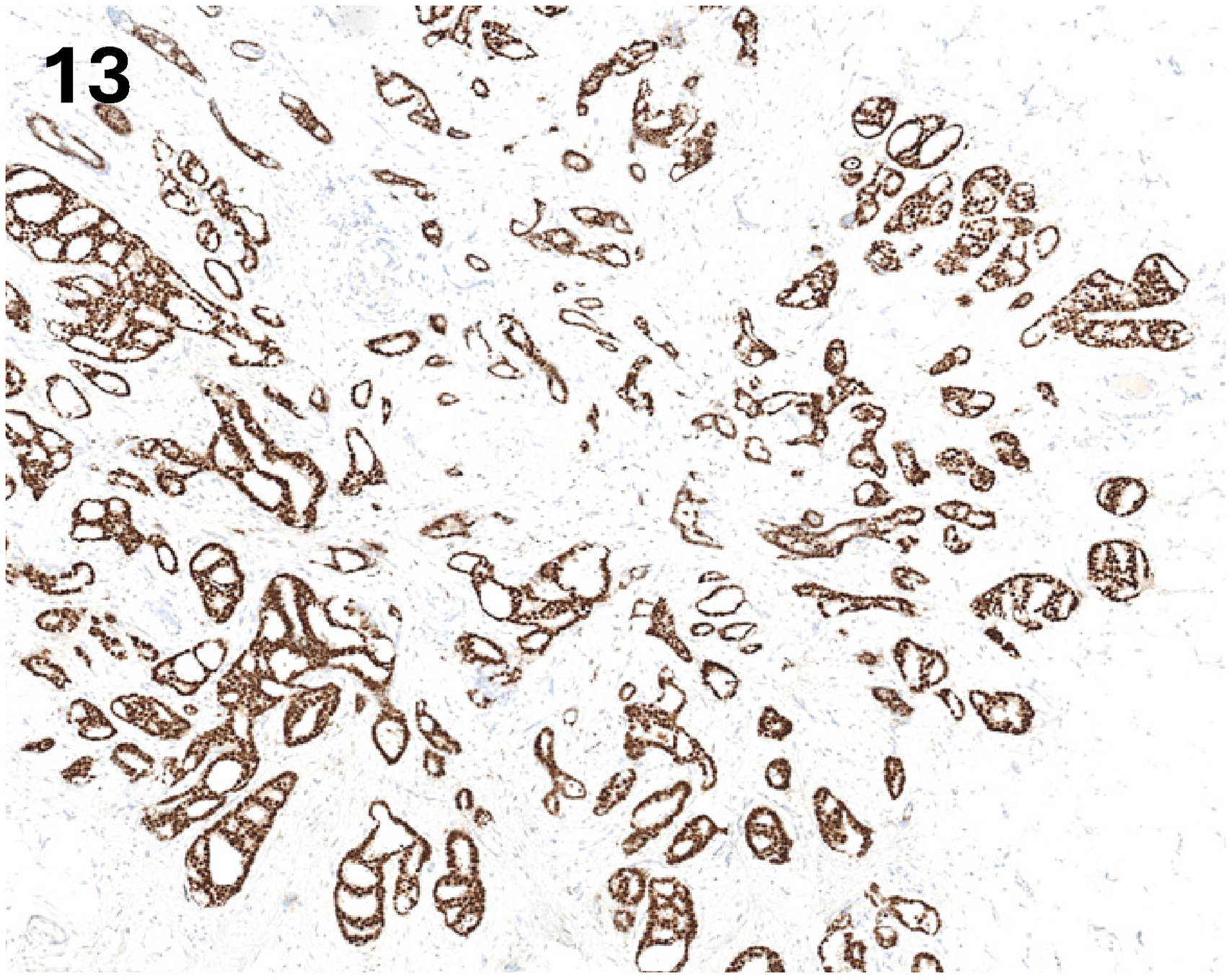
Immunochemical stain for ER staining (x 40) is positive in the well-differentiated ductal carcinoma. ER, estrogen receptor.
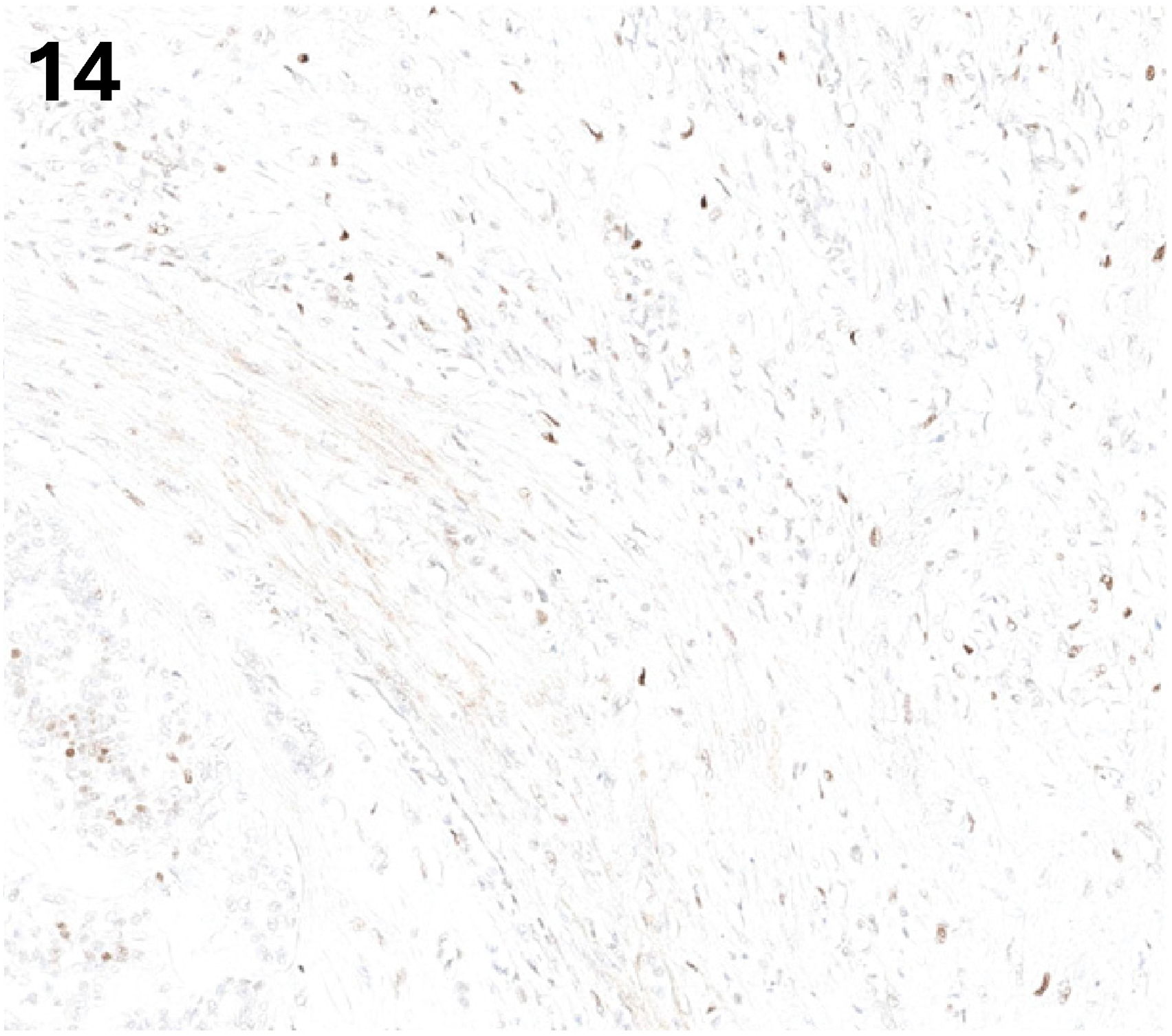
Immunochemical stain for p53 staining (x 100) is wild type in spindle cell carcinoma and adenomyoepithelioma.
Discussion
Breast adenomyoepithelioma is a biphasic tumor, and its malignant counterpart, malignant adenomyoepithelioma, is diagnosed based on features such as infiltrative margins, high mitotic activity, nuclear atypia, and necrosis. 5 The diagnosis relies on comprehensive histopathological examination and immunohistochemistry. In adenomyoepithelioma, the epithelial cells are typically positive for keratins CAM5.2 and keratin 7, while myoepithelial cells express markers like P63, calponin, and SMMHC. 4 However, in malignant adenomyoepithelioma, myoepithelial cells may lose expression of some markers due to dedifferentiation. 6 In our patient, the malignant spindle cells were S100 and P63 positive but negative for keratins, supporting a myoepithelial origin.
The keratin negativity of the spindle cell component initially raised suspicion for other spindle cell lesions of the breast, such as primary breast sarcoma or the spindle cell stromal component of a malignant phyllodes tumor. However, primary breast sarcomas were excluded by the strong P63 positivity in the spindle cells, which is highly characteristic of myoepithelial differentiation and not typically seen in sarcomas. Malignant phyllodes tumor was also excluded as the tumor lacked the classic leaf-like architecture and heterologous stromal differentiation. The presence of a clear transition from a biphasic adenomyoepithelioma, combined with the P63 and S100 positivity in the spindle cells, definitively supported the diagnosis of malignant adenomyoepithelioma with a malignant myoepithelial (spindle cell) component.
Rakha et al proposed a classification for adenomyoepithelioma-related lesions, including adenomyoepithelioma with invasive carcinoma, defined as an invasive carcinoma coexisting with a benign adenomyoepithelioma. 5 The tumor described herein fits this description, as the spindle cell carcinoma demonstrated a clear transition from a biphasic adenomyoepithelioma, while the well-differentiated invasive ductal carcinoma appeared separate. This distinction is strongly supported by the immunohistochemistry findings: the adenomyoepithelioma and its associated spindle cell carcinoma were ER/PR-negative, typical for these lesions,5,7,8 whereas the invasive ductal carcinoma was strongly ER/PR-positive. This suggests that the spindle cell carcinoma may arise from the adenomyoepithelioma, while the invasive ductal carcinoma represents a distinct, coincidental primary malignancy—a “collision tumor,” defined as the presence of two independent and histogenetically distinct neoplasms occurring in the same organ without intermingling, in contrast to a true mixed or composite tumor where components share a common origin or are intimately admixed. In one study, TP53 mutation has been documented in the malignant myoepithelial component of adenomyoepithelioma by laser capture microdissection, with the mutation absent in the benign epithelial component and adjacent normal ductal epithelium, suggesting that TP53 mutation may be a late event contributing to malignant transformation of the myoepithelial compartment, 9 In our study, immunostain for p53 showed weak staining in both spindle cell carcinoma and adenomyoepithelioma, suggesting other pathways for malignant transformation.
The presence of two primary malignancies raises questions about a potential shared molecular pathway versus two independent carcinogenic events. Future molecular profiling of similar tumors could elucidate whether these components share common mutations.
The management of such combined tumors is challenging. The general principle for malignant adenomyoepithelioma is surgical excision with wide, clear margins due to its high local recurrence rate and metastatic potential. 4 The presence of invasive ductal carcinoma necessitates additional considerations, such as endocrine therapy for hormone receptor-positive tumors. Prognosis in such a combined scenario is likely dictated by the more aggressive malignant adenomyoepithelioma component.
In conclusion, we report a unique presentation of malignant adenomyoepithelioma coexisting with a well-differentiated invasive ductal carcinoma. This report underscores the critical role of meticulous histopathology and comprehensive immunohistochemistry for correct diagnosis. It emphasized the importance of extensive sampling in big tumors. The small focus of invasive ductal carcinoma could have been missed without extensive sampling. When this focus of invasive ductal carcinoma was identified microscopically, we submitted 10 more sections on this tumor to make sure there was no other lesion missed. Second, it also helps us understand the implications for patient management in such complex scenarios. If the invasive ductal carcinoma had been, for example, more than 10 mm in size, the management strategy could have changed. Finally, the clear immunohistochemical distinction between these two components provides valuable insight into their independent origins (“collision tumor” phenomenon). Parallel sequencing of the two different tumors will help us to understand the pathogenesis of the lesions and potentially change the current understanding of malignant adenomyoepithelioma.
Footnotes
Ethical Approval
A single case report does not require IRB approval at the authors' institution.
Author Contributions
All authors contributed to the critical revision of the manuscript and have read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.