
Abstract
Clinical and radiographic data were analyzed for 49 surgical interventions of painful heel syndrome with a mean follow-up of 4 years and 7 months. In all patients the surgical procedure consisted of a triangular shaped resection of the posterosuperior portion of the calcaneus. The clinical evaluation showed disappointing results with complete relief of complaints in only 34 procedures (69.4%), and 7 patients (14.3%) with even a worsening of their symptoms. The time course of rehabilitation was long with an average of 6 months of functionally significant pain after surgery, reducing the willingness to undergo this operation again. Formerly published angular thresholds of radiographic calcaneal angles could not be confirmed to be predictors for the preoperative symptoms or the postoperative outcome. There was no accumulation of pathologic clinical foot shapes, only a slight increased calcaneal pitch in patients with isolated pain on the posterosuperior lateral part of the calcaneus. According to Haglund's description of painful heel syndrome, the clinical picture of our patients included affections of bone, tendon, peritendon, bursae, soft tissue and skin in different combinations.
Based on this evaluation, we advise to be cautious to indicate the operation. All possibilities of conservative treatment should be performed prior to surgery.
INTRODUCTION
During preoperative decision making for surgery of Haglund's syndrome, patients normally consider this operation as a minor intervention. Reviewing the literature, postoperative results range from excellent 5,7,10 to disappointing. 11,14
Various clinical and radiographic measurements have been introduced to detect functional and anatomic risk factors producing painful heel syndrome. 1,2,3,5,8,12,13 Radiographic measurements have been published to determine the optimum angle of resection of the posterosuperior portion of the calcaneus. 12 This type of operation - the resection of one triangular shaped bony wedge down to the insertion of the achilles tendon - was introduced by Spitzy in 1933 and first published by Aberle in 1937, 1 while Haglund himself 4 proposed only to smoothen the upper posterior ridge of the calcaneus. Other techniques, like the “closing-wedge-technique” first published by Zadek 15 did not gain wider propagation.
The aim of this study was to analyze the pre- and postoperative clinical and radiographic data to find out any predisposing factors influencing outcome after surgery. We tried to verify formerly published clinical risk factors and radiographic angular thresholds. Additionally, the time course of rehabilitation was analyzed to obtain data for better decision-making and preoperative advice for the patient.
MATERIAL AND METHODS
49 operations (25 left and 24 right calcanei) in 36 patients (23 female, 13 male) were reviewed clinically and radiographically in a retrospective evaluation with a minimum follow-up of 1 year (mean 4 years and 7 months, range 1 year −11 years). 12 patients were operated bilaterally, 9 of them simultaneously on both sides. The average age at time of surgery was 54.5 years (range14.9–70.3 years).
Surgery was carried out under general anaesthesia in a prone position using a pneumatic tourniquet. One centimeter anterior to the lateral border of the achilles tendon, a vertical incision was made to expose the retrocalcaneal bursa and the posterosuperior lateral portion of the calcaneus. The posterior surface of the os calcis was removed extending the osteotomy down to the insertion of the achilles tendon. The remaining lateral ridge was carefully smoothed using an osteotome. If present, a bony spur in the insertion of the tendon was exposed and removed which normally required a release of a portion of the achilles tendon. After irrigation and insertion of a drain the wound was closed. Pain free patients were mobilized fully weight-bearing, all other patients were mobilized partially weight-bearing using 2 forearm crutches for the duration of major postoperative pain. Only in cases of a release of the achilles tendon was a short leg cast applied for 3 weeks.
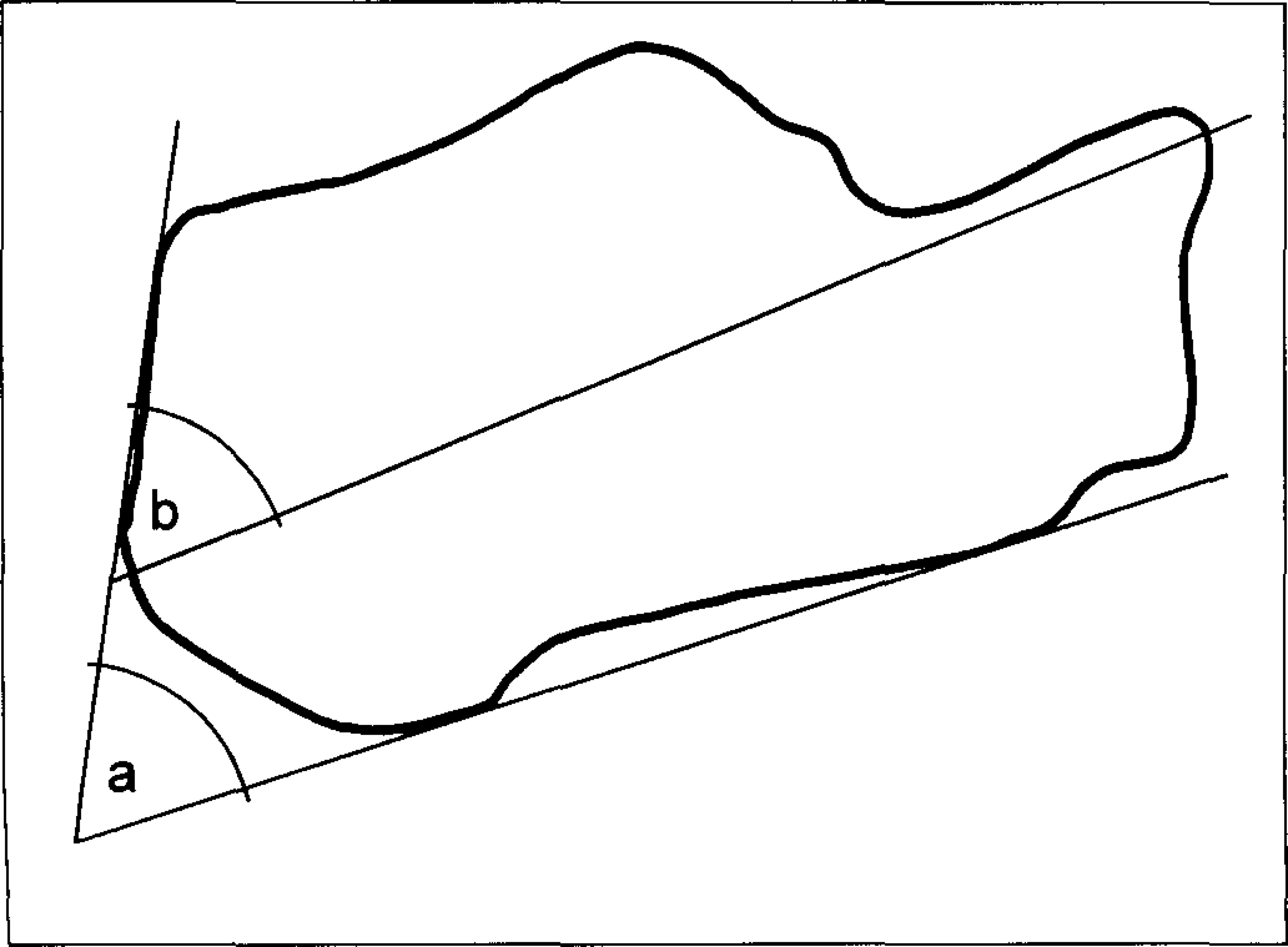
Radiographic measurement of angles independent of the ground, as drawn on plain lateral radiographs. Fowler-Philip's angle = “a”. Steffensen's angle = “b”.
For all patients the Ankle-Hindfoot-Score according to the American Orthopaedic Foot and Ankle Society 6 was calculated. This score evaluates pain, activity limitations, requirement of support, maximum walking distance, problems on different walking surfaces (uneven terrain, stairs, inclines and ladders), gait abnormality, sagittal motion (flexion and extension of the tibiotalar articulation), hindfoot motion (inversion and eversion of the talocalcaneal articulation), ankle-hindfoot stability and ankle-hindfoot alignment. The time course from the onset of complaints until surgery was documented as well as the preoperative conservative treatment. The time course following surgery until the ability to wear conventional shoes, return to full work duties, full sporting activities as well as total duration of complaints. There was also documented overall satisfaction with surgery, location of pain, tenderness, swelling, local condition of the surgical scar including sensory disturbances, the shape of the foot and the heel-rise test were all recorded.
For the radiographic analysis the following angles were drawn on plain weight-bearing lateral radiographs (Fig. 1 and 2): the angle between the plantar aspect and the posterior surface of the calcaneus, first published by Fowler and Philip in 1945 2 (angle a); the angle between the longitudinal axis of the calcaneus and the posterior surface according to Steffensen and Evensen (1958) 13 (angle b); the calcaneal inclination angle between the ground and the plantar aspect of the calcaneus, introduced by Ruch in 1974 9 (angle c); the angle between the ground and the posterior surface of the calcaneus according to Ruch (1974) 9 (angle d); the angle between the ground and the postoperatively remaining posterior surface, as published by Sella in 1998 12 (angle e); the angle between the ground and the longitudinal axis of the calcaneus (angle f); the angle between the preoperative posterior surface and the postoperatively remaining posterior surface (angle g).
The following linear measurements were taken of the posterior surface of the calcaneus and the area of resection (Fig. 3): the length of the posterior surface preoperatively (distance x); the two-dimensional amount of resection in millimeter (distance y); the length of the postoperatively remaining posterior surface in millimeter (distance z); the amount of resection in relation to the entire posterior surface in percent.
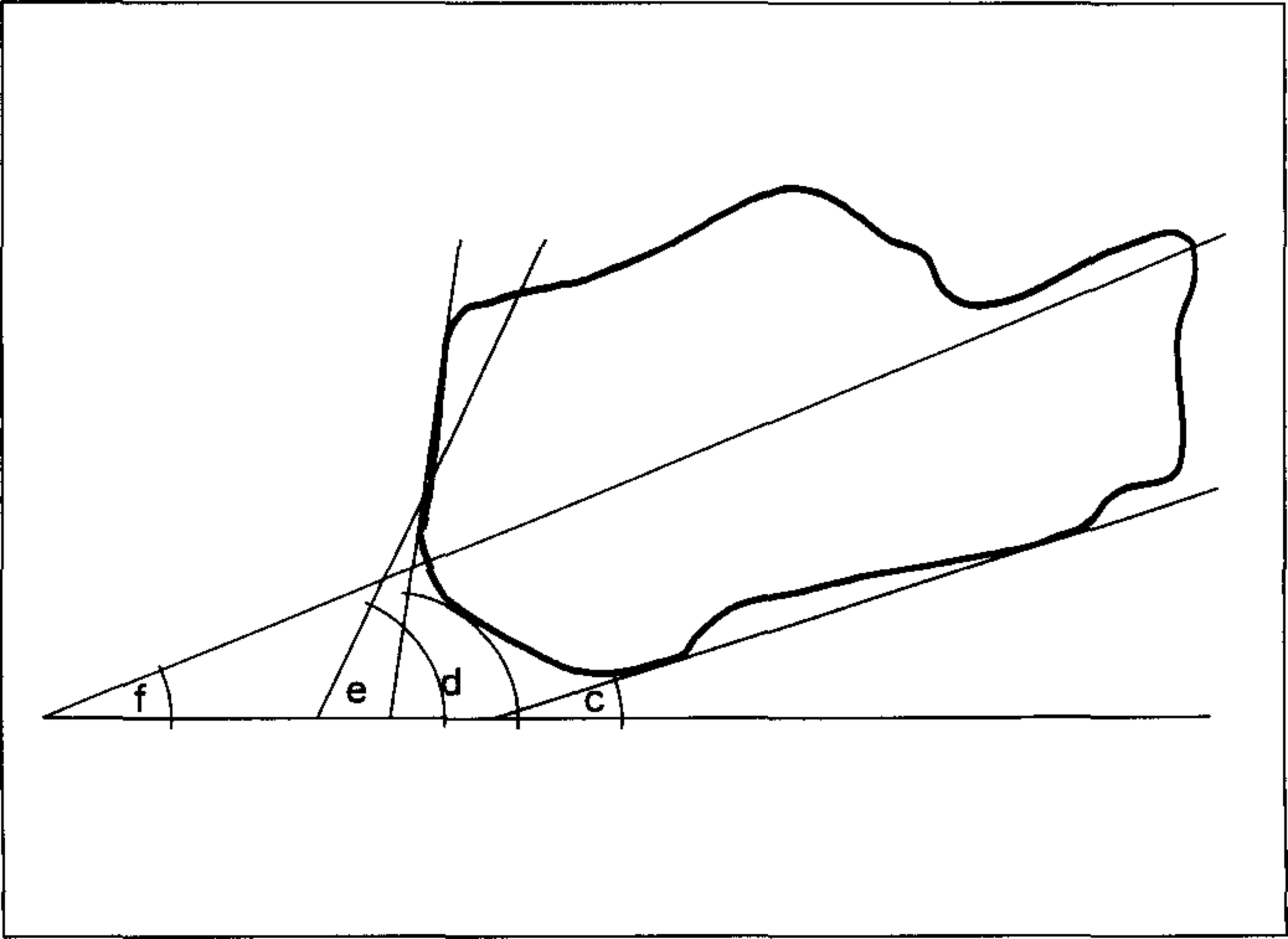
Radiographic angles using the ground as reference, drawn on weight-bearing lateral radiographs. For explanation see Materials and Methods.
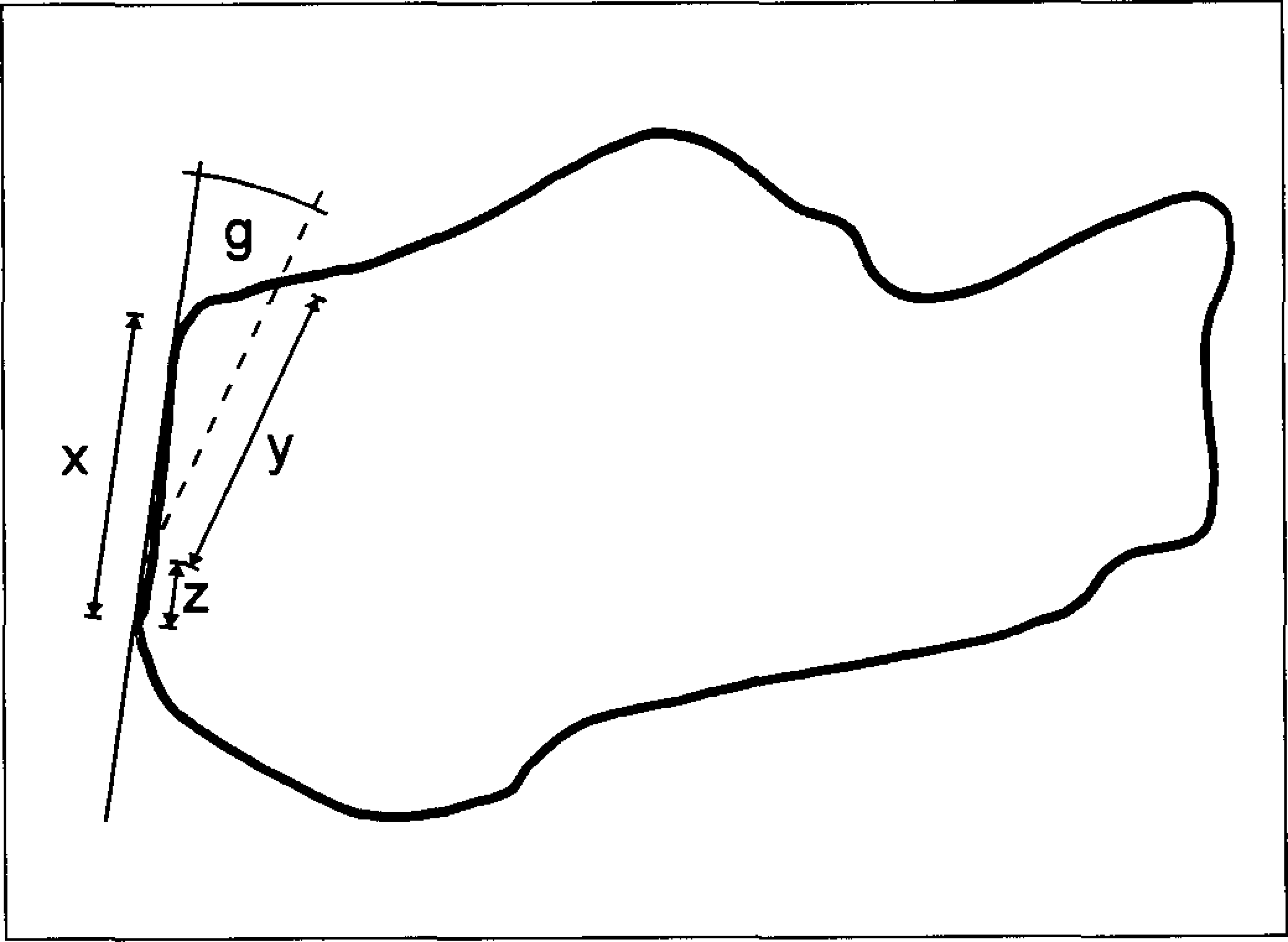
Radiographic measurement at the area of resection. The percentage resection is calculated as (z/x*100).
Wilcoxon's signed rank test (two-tailed) was used to evaluate the magnitude of differences between subgroups.
RESULTS
The mean interval from the begin of complaints until the first medical consultation was 1 year and 10 months (range 1 week–12 years); until the surgical intervention it was 3 years and 7 months (range 4 weeks–28 years). Preoperative conservative treatment was tried in 26 cases (53.1%). The postoperative AOFAS-Ankle-Hindfoot-Score ranged 65–100 points (mean 93.9 points).
13 patients were post operatively able to be mobilized fully weight-bearing; for the remaining 36 patients the post operative immobilization (using two elbow crutches) ranged from 1 week to 12 weeks (mean 4 weeks). In 10 cases a short-leg cast was applied for a mean of 5.7 weeks (range 3–12 weeks).
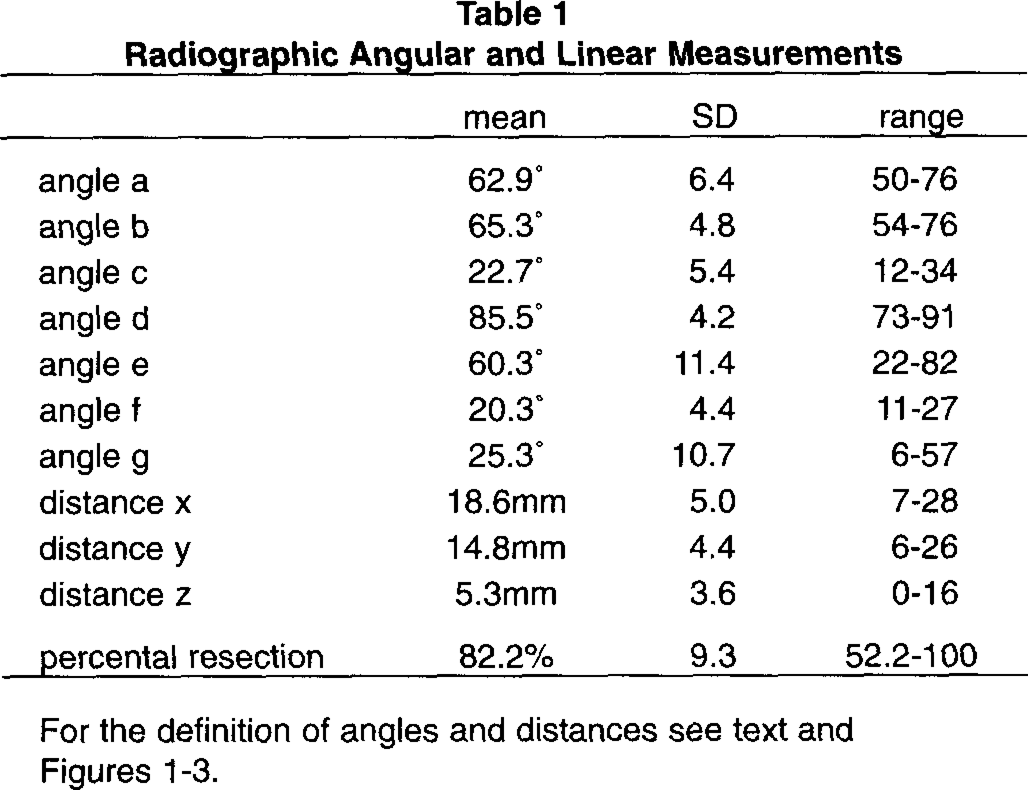
Radiographic Angular and Linear Measurements
The patients returned to work after a mean interval of 7.5 weeks (3–25 weeks). They were able to wear conventional shoes after 8.0 weeks (1 week–30 weeks). Returning to preoperative sporting activities was possible after a mean of 20.3 weeks (range 4–52 weeks). The subjective overall postoperative complaints lasted 24.3 weeks (4–160 weeks).
Early complications were seen in 4 cases (3 extensive haematomas, 1 superficial infection), in three cases late complications needed revision surgery (1 recurrent bony spur, 1 foreign-body reaction following the use of bone wax, 1 painful ossification between the calcaneus and the achilles tendon).
34 patients reported a complete relief of pain and 7 patients noted some improvement; 1 patient described no change and 7 patients complained of worsening of their symptoms. The overall satisfaction showed a mean of 1.75 on a scale from 1 (very satisfied) to 5 (completely unsatisfied). 43 patients would undergo this operation again and 7 patients would not.
The main location of preoperative complaints was the posterosuperior lateral portion of the os calcis in 44 cases, the respective medial portion in 21 cases and the region of the retrocalcaneal bursa in 19 cases. Other anatomical structures like the calf, the achilles tendon and the peritendon as well as the posterior surface of the calcaneus were affected in a minor percentage which is shown in Figure 4.
40 feet were shaped normally, one cavus foot and 8 feet with diminished longitudinal arch. No flatfeet were seen. The rearfoot orientation showed a mean of 0.9° heel valgus (SD ±2.3°, range 5° varus–10° valgus); for the forefoot a mean of 0.7° forefoot varus (SD ±3.1°, range 10° varus–10° valgus) was calculated.
Postoperatively the complaints were reported most frequently in the posterosuperior lateral portion of the calcaneus in 13 cases, the peritendon in 7 cases and the postero-superior medial portion of the os calcis in 6 cases (Fig. 4). Sensory disturbances around the scar were seen in 10 cases, one of these was highly suspect for a postoperative neuroma of the sural nerve - but the patient refused revision surgery.
The radiographic results of pre- and postoperative calcaneal angles and distances are shown in Table 1. Based on our data various subgroups according to different clinical or radiographic values were established. By that we evaluated the following statistically significant differences: Patients with preoperative pain exclusively on the posterosuperior lateral portion of the calcaneus had a higher angle d of 87.6° comparing to 84.5° in patients with disseminated and diffuse pain (p = 0.005). This difference was also seen for angle a with 64.7° for the group with isolated pain localization contrasting with only 62.0° for the group with diffuse pain (p = 0.03).
A comparison of patients who had surgery unilaterally or bilaterally showed that the time interval until resumption of full sporting activities was longer for those after bilateral operation (6 months and 1 week) comparing to 3 months and 2 weeks after unilateral operation (p=0.008).
Analyzing the data forming subgroups according to radiographic angular thresholds published in former evaluations, 2,9,12,13 no statistical differences between these subgroups were found.
No statistical influence on the postoperative result was detected in relation to the two-dimensional measurements at the resection area (distances x, y and z), the percentage of two-dimensional resection or the angle g between the posterior surface and the line of resection.
DISCUSSION
In the patients' opinion the surgical treatment of “painful heel syndrome” is a minor intervention. They expect to undergo an operation with negligible postoperative pain and fast rehabilitation. Even most orthopedic surgeons would classify the operation of a Haglund exostosis as a short surgical procedure without major problems for the patient. The aim of this study was to evaluate the time course of rehabilitation after surgery as well as the patients' satisfaction with surgery.
Our data show only 73.5% of satisfied patients, which is not acceptable for a surgical intervention that is considered “quick and easy” by most patients. Corresponding to this dissatisfaction the willingness to undergo this operation again was low (14.3% of our patients would refuse this operation under the same circumstances). This unsatisfactory outcome correlates with poor results of Taylor 14 (36% of patients dissatisfied with the outcome of surgery), Schepsis and Leach 11 (29% unsatisfactory results, despite a small selected group of highly motivated athletes) but contrasts with the good results of Pauker et al, 7 (89.5% good and fair results), Sammarco and Taylor 10 (97% excellent and good results) and Jones and James 5 (100% successful). Between these good and poor results there are data of Fuglsang and Torup, 3 stating that the results obtained in their conservatively treated and surgically treated groups are quite uniform and the disease presumably tends towards spontaneous healing.
Analyzing the details of our study, the main reason for the patients' dissatisfaction may be the long time course of rehabilitation - a mean of 2 months until the patients were able to wear normal shoes again, nearly 6 months after surgery with postoperative pain and 5 months to resume full sporting activities. A comparison of patients who had surgery unilaterally or bilaterally showed that the interval until resumption of full sporting activities was longer for those after bilateral operation. Nevertheless, most of the bilaterally operated patients did not regret the bilateral intervention as they saved time by only one rehabilitation period. No differences were found in these intervals regarding shoe wear, duration of postoperative pain and full fitness for work. Comparing groups with and without postoperative immobilization, no statistical significant differences were detected.
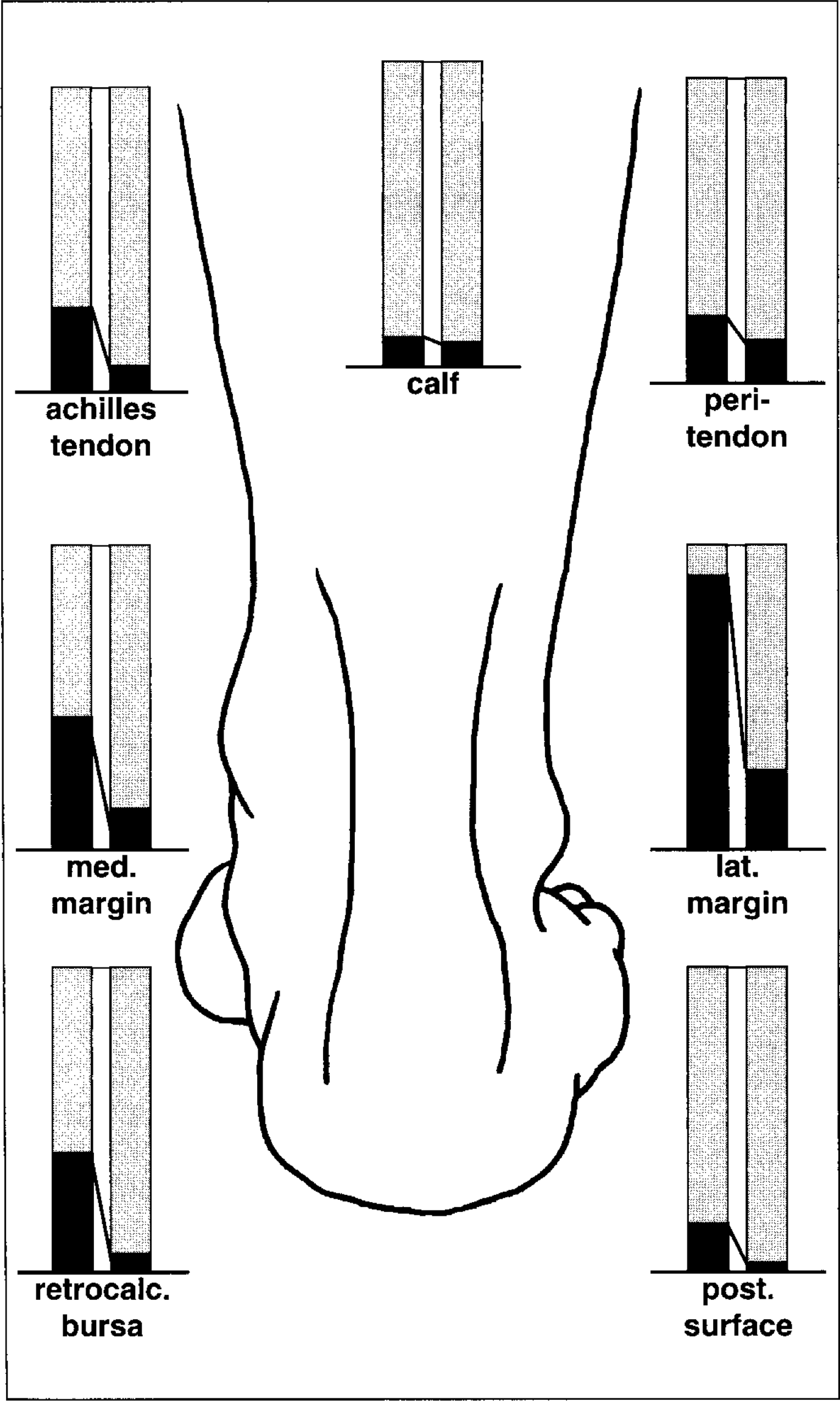
Percentage distribution of pre- and postoperative pain location (left bars - preoperative; right bars - postoperative)
A second reason for the dissatisfaction was persisting pain. The expectation of complete pain relief was fulfilled in only two thirds of the patients. All patients who would not have the surgery again still have at least moderate pain.
To find out possible factors influencing the outcome of surgery, formerly published risk factors were analyzed in our data: Regarding the shape of the feet, no accumulation of pathological shapes - especially cavus feet - was observed.
Our data did not show abnormal mean values in the angles reflecting the varus-valgus orientation of forefoot and hindfoot. These data are in contrast to former publications that postulate a higher incidence of cavus feet in patients with painful posterior lesions of the heel. 1,3,5 The hypothesis of compensated rearfoot varus, compensated forefoot valgus, rigidly plantarflexed first ray with abnormal subtalar joint motion being a predisposing factor to Haglund's syndrome 5,8,12 could not be confirmed by our data.
Patients with preoperative pain exclusively on the posterosuperior lateral portion of the calcaneus (the typical isolated “pump-bump”) showed higher angles (a) and (d) than those with more diffuse pain (p = 0.005). This may indicate a more mechanical pathogenesis with influence of the calcaneal pitch in these cases where pain is located only at the posterolateral portion of the calcaneus - the typical “pump-bump” - without presence of a notable exostosis in this region.
Besides this indication of a causative pathogenic factor, it was impossible to crystallize other single entities that showed any correlation to the clinical preoperative situation, the postoperative outcome or any radiographic data. In most cases the clinical picture consisted of a combination of retrocalcaneal bursitis, superficial tendo Achilles bursitis, peritendinitis, tendinitis, retrocalcaneal impingement and tender thickening of subcutaneous tissues. A notable exostosis was not found responsible for the development of retrocalcaneal pain. This absence of a special exostosis in cases of a painful heel syndrome has already been stressed by Haglund himself. 4
Comparing patients with an angle a of 69° or smaller - which was the normal range in Fowler's 2 patients - to those over 69°, no differences were found in preoperative nor postoperative pain intensity or AOFAS-score. Only two of our 49 patients showed a Fowler-Philip angle of 75° or higher (this angle was published by Fowler for cases that become symptomatic due to structural changes in the soft tissues covering the bursal area).
Using the method and angular threshold of Steffensen, 13 no differences were found between patients that should have a predisposition according to Steffensen with an angle b of 63°–65° or over, comparing to the normal range of 60° or under.
Ruch 9 considered an angle d greater that 90° as risk for the development of clinical symptoms. In our study there were only 7 patients with this angle of 90° or greater. These patients did not differ significantly from those under 90° regarding preor postoperative clinical data.
Sella et al. 12 recommended to achieve an angle of around 49° between the osteotomy and the longitudinal axis of the calcaneus (angle e) for best results. Our data did not show any better results in patients that achieved exactly, or came near this angle.
The analysis of the two-dimensional measurements at the area of resection (distance x, y and z; percentage area of resection) as well the angle (g) between the original and the surgically created posterior surface did not show any influence on the clinical success.
These data show that neither typical clinical signs nor radiographic measurements can predict the outcome of operative treatment. As surgical treatment of a painful heel syndrome often results in unsatisfied patients, we advise caution recommending this operation. It is mandatory to inform all patients about the long postoperative rehabilitation. Therefore prolonged conservative treatment should be completed before surgery is entertained.