
Abstract
The incidence of calcaneal fracture has been slowly increasing; however, the ideal treatment for displaced intra-articular fracture is not available yet, even though the fracture brings frequent complication and disability. Between April 1991 and March 1998, we treated 103 displaced intra-articular calcaneal fractures of 92 patients surgically with limited posterior incision, modified Gallie approach. There were thirty-seven tongue-type fractures, fifteen tongue-type fractures with moderate comminution, nineteen joint-depression fractures, twenty-nine joint-depression fractures with moderate comminution, and three extensively comminuted fractures. The fracture fragments were fixed mainly with partly threaded small cancellous screws or Steinmann pins without any bone graft. Ankle and subtalar motion was permitted immediately if fixation were stable enough. Otherwise, a short period of cast immobilization was utilized. With a mean follow-up of 28 months (range, 12 to 66 months), eighty six percent of feet had no pain or only occasional pain not requiring medication. Using American Orthopedic Foot and Ankle Society hindfoot score system for assessment, ninety percent of feet rated as good to excellent. We used “Circle draw test” for evaluation of subtalar motion during follow-up visitation and found eight-seven percent of feet showed good to excellent correlation with the functional recovery. We recommend a limited posterior incision for reduction and internal fixation of displaced intra-articular calcaneal fractures. For displaced intra-articular fractures with three or four large fragments without further comminution and without a displaced fracture of the calcaneal cuboid joint, this method is particularly useful. We also recommend a Circle draw test for evaluation of subtalar joint motion as well as an indicator of functional recovery after displaced calcaneal fractures.
INTRODUCTION
The calcaneus is a complex bone that acts as a major part of the platform for walking and standing and as a fulcrum that allows the calf musculature to propel the body forward. 18,26 Numerous controversies have surrounded the management of patients who have a calcaneal fracture. 16,20 The primary source of disagreement has been the issue of whether better results are achieved with operative or non-operative treatment. Non-operative treatment has also varied and may include early motion, closed reduction, immobilization in a cast, and non weight-bearing. 14,17,22,23 These closed methods have not been successful in restoring congruity of the subtalar joint or in producing a painless functional foot after the fracture has healed. 27
Operative methods have included open reduction and internal fixation, 1,4,5,15,21,24,25 primary arthrodesis, 8,9,19 and percutaneous reduction. 7,12 Satisfactory results have varied from 46% to 86% and criteria for these results have not been standardized. 15 Proponents of open reduction correctly insist that direct manipulation of the articular fragments is the only means of achieving reduction of the posterior facet — an essential first step in restoring function of the subtalar joint. Open reduction and internal fixation has been performed most commonly through a medial, 4,5 lateral, 1,15,21,24 or combined medial and lateral approach. 25 Although it is hoped that open reduction and internal fixation will improve the outcome of calcaneus fractures, the ideal treatment is not clearly established yet.
In 1943, Gallie 8 described a posterior approach to the subtalar joint for subtalar fusion. Authors have used posterior approach for open reduction and internal fixation of displaced intra-articular calcaneal fracture with some modification of the Gallie approach.
The purpose of this paper is to describe the limited posterior incision and to report on the results in 103 intra-articular fractures that were treated by this method.
MATERIAL AND METHODS
Between April 1991 and March 1998, 103 displaced fractures of the calcaneus in 92 patients were treated surgically. These were treated with open reduction and internal fixation through a limited posterior incision. The indications for the surgical treatment included displacement of either the fragment of the tuberosity or the posterior facet, and incongruity or angulation of the articular surfaces of the posterior facet. All of the procedures were performed by one of us (Park, I.H.).
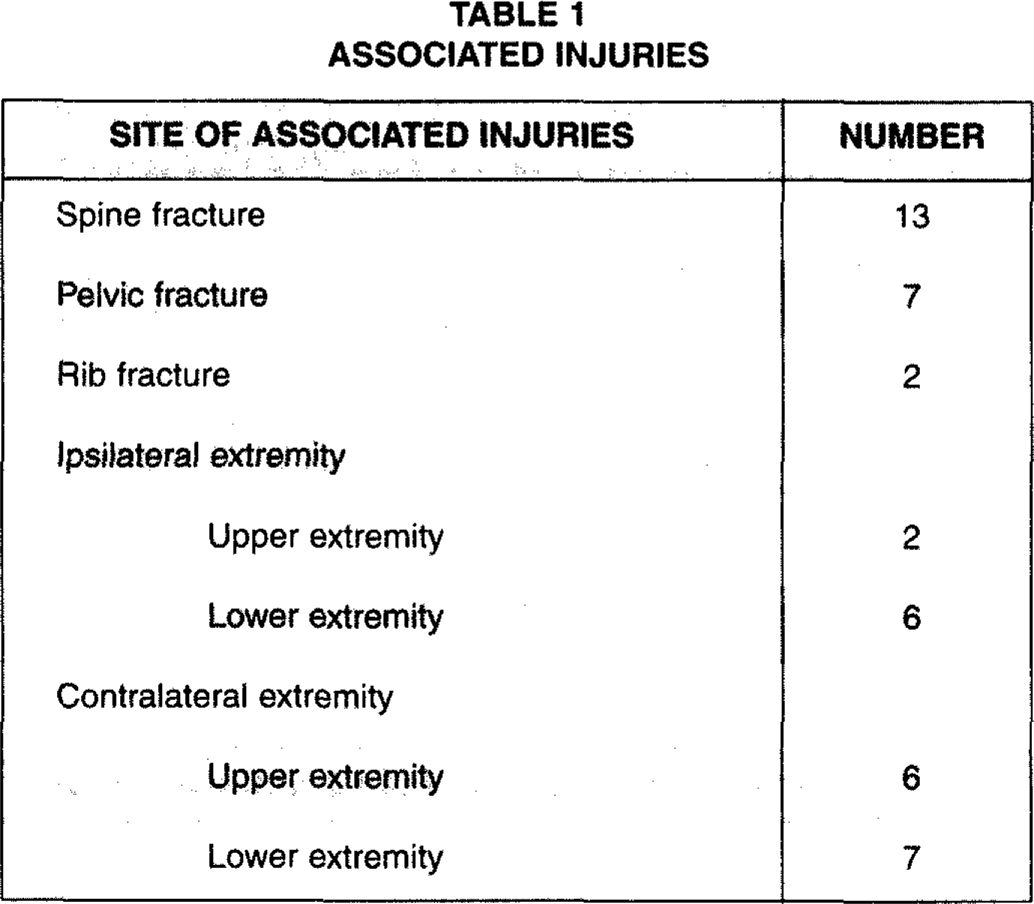
The average age of the patients was 39 years (range, 16 to 69 years). Seventy-seven percent of patients were between the ages of twenty and fifty. Seventy-three patients were males and nineteen were females. Fifty-nine of the fractures were on the left and forty-four were on the right side. Eleven patients had bilateral calcaneal fractures. The mechanism of injury was a fall from a height in eighty-three patients and motor-vehicle accident in nine. Associated injuries are listed in Table 1.
Radiographic examination included AP, lateral, and oblique views of the foot, as well as an axial and Broden's views of the calcaneus. The AP and oblique allow visualization of the calcaneocuboid joint. The axial view shows the amount of displacement along the primary fracture line and the amount of widening. Broden's views were made of the fractured calcaneus for diagnosis, classification, and planning for surgery. Broden's radiographs were used in an effort to determine the congruity of the surfaces of the entire posterior facet. The posterior portion of the surface of the joint is shown on the 10-degree radiograph: the anterior portion, on the 40-degree radiograph; and the intermediate surfaces, on the 20 and 30-degree radiographs. 3,4 CT scanning was not routinely used.
ASSOCIATED INJURIES
RADIOGRAPHIC RESULTS a
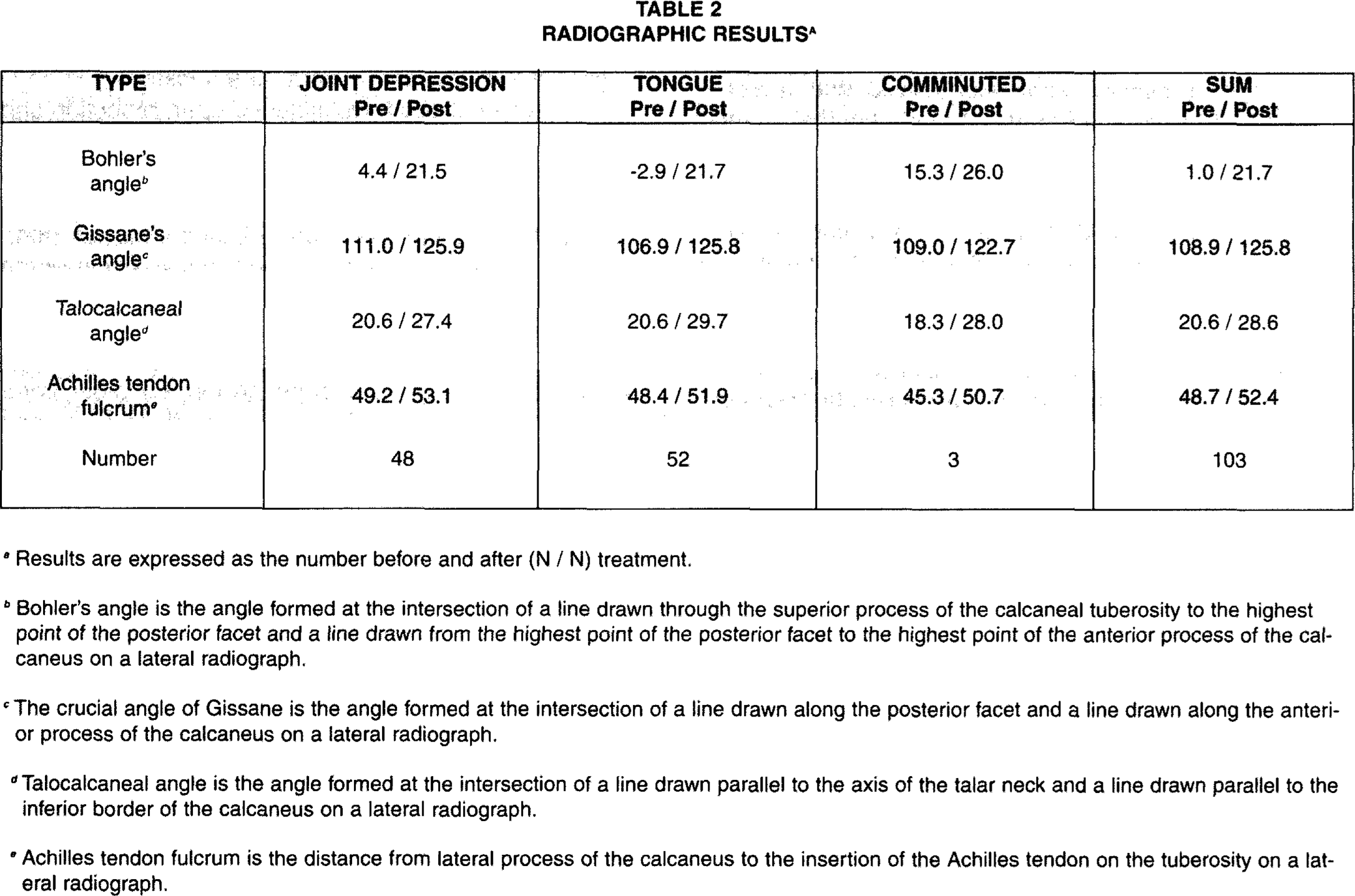
Results are expressed as the number before and after (N / N) treatment.
Bohler's angle is the angle formed at the intersection of a line drawn through the superior process of the calcaneal tuberosity to the highest point of the posterior facet and a line drawn from the highest point of the posterior facet to the highest point of the anterior process of the calcaneus on a lateral radiograph.
The crucial angle of Gissane is the angle formed at the intersection of a line drawn along the posterior facet and a line drawn along the anterior process of the calcaneus on a lateral radiograph.
Talocalcaneal angle is the angle formed at the intersection of a line drawn parallel to the axis of the talar neck and a line drawn parallel to the inferior border of the calcaneus on a lateral radiograph.
Achilles tendon fulcrum is the distance from lateral process of the calcaneus to the insertion of the Achilles tendon on the tuberosity on a lateral radiograph.

Left, Straight incision is made along the lateral side of the tendo Achilles, down to the calcaneus. Right, this dissection deepens while protecting the sural nerve which is lateral and anterior to the incision.
From the radiographs, the type of fracture was determined. 6 This classification is based upon a modification of the fracture classifications of Essex-Lopresti, Soeur and Remy, and Burdeaux. 4,5,7,20,24,25 The posterior secondary fracture line may exit behind the subtalar joint or at the posterior cortex of the tuberosity and is classified as the joint depression or tongue type, according to Essex-Lopresti. Moderate comminution of a fracture was defined as the presence of more than one posterior and one anterior secondary fracture line on the lateral and Broden's radiographs. Joint depression and tongue-type fractures were subdivided according to the degree of comminution. When there was such extensive comminution that the fracture could not be classified as a joint depression or tongue type, it was classified as extensively comminuted. 20 There were thirty-seven tongue-type fractures, fifteen tongue-type fractures with moderate comminution, nineteen joint-depression fractures, twenty-nine joint-depression fractures with moderate comminution, and three extensively comminuted fractures.
Left, After dissecting deep tissues, the articular cartilages are exposed. Displaced tongue or depressed posterior facet fragments of the fractured calcaneus can be seen well at this time and can be reduced or elevated to restore the joint. Right, The tongue- or joint depression-type fragments must be derotated and elevated to restore the articular surface of the posterior facet. This is accomplished under direct vision.
Surgery was usually performed as soon as possible after injury if the patient's general and local status permitted, but usually was done 3 to 7 days later when swelling and skin condition were stabilized.

The posterior facet is realigned with a periosteal elevator placed in the fracture site. The alignment of the tuberosity is generally maintained by K-wires directed into the sustentaculum tali while the rest of the reduction is completed.
Surgical Technique
Under adequate anesthesia with the patient in prone position and the ankle and feet hanging over the end of the operating table in order to allow full mobility of the foot and ankle, a tourniquet is inflated after 2 minutes elevation of the leg. 7 A three inch longitudinal incision is made along the lateral border of the Achilles tendon (Fig. 1, Left). This skin incision begins about an inch proximal and posterior to the tip of the fibula, and extends distally to the calcaneus. 8 The deeper dissection is carried through the superficial and deep fascia to the posterior subtalar joint. 9 Any branches of the sural nerve are protected. After clearing fat and hematoma the posterior subtalar joint is reached. The capsule and synovial membrane of this joint are then incised transversely, and the articular cartilage is exposed 11 (Fig. 1, right). It is then possible to visualize the entire posterior facet of the calcaneus. 10,11 (Fig. 2, left). Displaced tongue or joint fragments of the fractured calcaneus can be seen well at this time and can be reduced 11 (Fig. 2, right).
To reduce these fractured fragments, the tongue or depressed fragments must be derotated or elevated to restore the articular surface of the posterior facet with direct vision of the articular surfaces. A narrow periosteal elevator is passed through the fracture gap usually located in the posterolateral area of the calcaneus and advanced under the depressed articular fragments while elevating them into anatomical position and in continuity with the sustentacular fragment. Similarly a tongue fragment is restored anatomically using the periosteal elevator under direct vision of the articular surface 11 (Fig. 3). It is often necessary to pull the tuberosity fragment distally and posteriorly using a bone hook to make room for the fractured fragments and to restore the height of the fractured calcaneus. In addition, the use of a compression device to reduce the width of the fractured calcaneus by compressing the medial and lateral wall is helpful 11,12 (Fig. 4a and 4b). After reduction of the joint depression or tongue type fragment toward the sustentacular fragment, which usually stays in anatomical position, these fragments are fixed with one or two small Kirschner wires. The fractures tend to be stable after reduction due to mechanical interlocking of the irregular cancellous bone surfaces of the sustentacular and tuberosity fragments. The fragments are also forced together by the tension developed in the soft tissue sleeve of skin and subcutaneous tissue by increasing the length and height of the calcaneus. 4 Intraoperative radiographs using C-arm image intensifier are performed to determine if the bone is reduced before definitive fixation is performed. 13 Roentgenograms should be obtained at this time to assure that the fragments are satisfactorily reduced. 30 and 40 degree Broden's views must be obtained at this point to assess joint reduction.
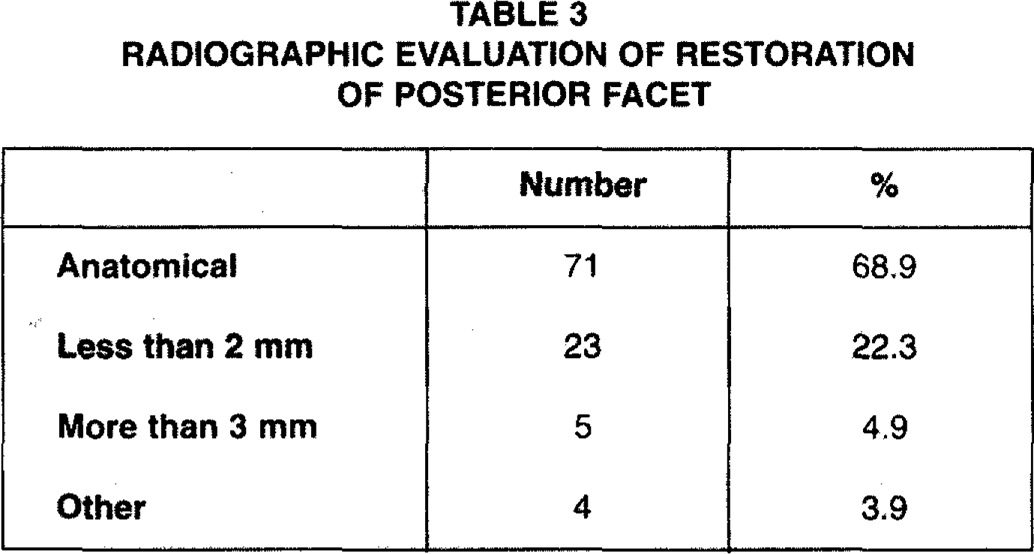
RADIOGRAPHIC EVALUATION OF RESTORATION OF POSTERIOR FACET
Secure the fixation by placing a partially threaded small fragment screw roughly paralleling the Kirschner wire(s). The screw should traverse subchondral bone and secure the posterior facet fragment(s) to the sustentacular fragment (Fig. 5). 11 Similar screw fixation secures the tongue and tuberosity fragments when necessary. 14 A pin may be drilled into the talus through the tuberosity fragment for additional temporary fixation.
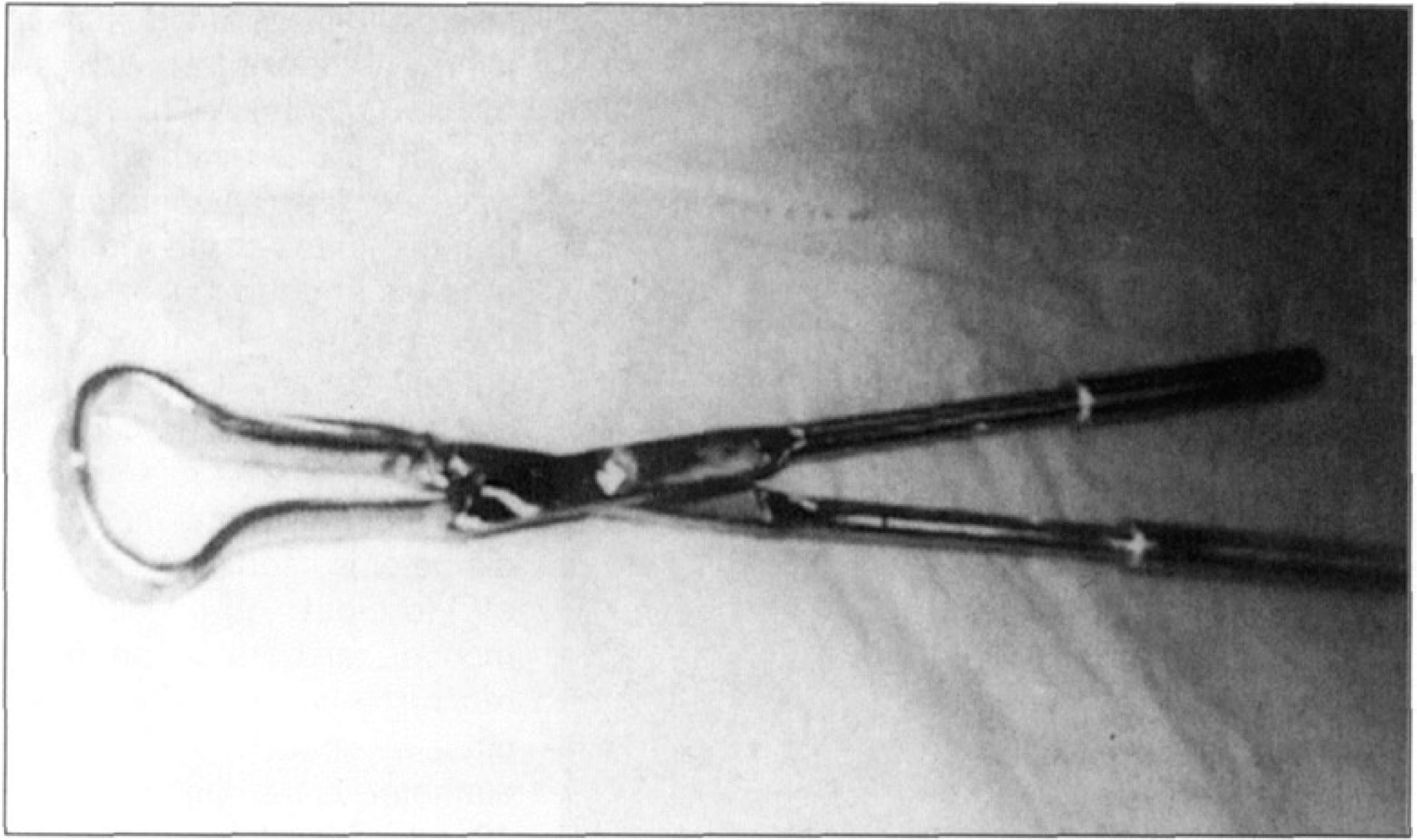
A compression device for reduction of the width of the fractured calcaneus.
After these main intra-articular fragments are fixed, the lateral wall is pushed medially to avoid fibular impingement. When necessary the lateral wall is reduced by squeezing both sides of the calcaneus using the previously mentioned compression device (Fig. 4). K-wire(s) can be used to hold the lateral wall in place.
Before the wound is closed, radiographs are made to document the status of the reduction and internal fixation. If satisfactory, the tourniquet is released and hemostasis obtained. The wound is closed loosely to allow drainage and a short leg splint, or a short leg cast is applied with the foot at a right angle.
If the fixation is stable, the patient can be placed in a removable posterior splint or compression dressing with elastic bandage and motion begun on the second postoperative day. 15 The patient is encouraged to perform supervised exercises of the toes, ankle and subtalar joints as the pain subsides. Ambulating without weight-bearing is permitted as the swelling subsides. Patients learn to draw the alphabet with the hallux of the injured limb, or make progressively larger circles with their forefoot. Weight-bearing is kept to a minimum for 6 weeks and is gradually increased up to full weight 6 to 12 weeks postoperatively.

The lateral wall bulge is reduced by applying pressure on both sides of the calcaneus using the compression instrument.
For unreliable patients or patients with unstable fracture fixation, cast immobilization is necessary. The initial cast and pin are removed at 4 weeks. After removal of the cast, the patient is encouraged to carry out exercises as above and very gradual weight-bearing.
RESULTS
The average follow-up on this group of patients was 28 months (12 months to 66 months). Patients had their surgery an average of 5.0 days (range, 2 to 14 days) after their injury. Table 2 lists the Essex-Lopresti classification and the number of patients with each type.
By inserting partly threaded screw(s) of proper length, interfragmentary compression is possible.
Thirty-four of the fractures were fixed with Steinmann pins, fifty-three with half-threaded cancellous screws, and sixteen fractures with both pins and screws. The pins were removed at 4 to 7 weeks (average, 5.8 weeks). Partial weight-bearing with crutches was allowed after 4 to 9 weeks (average, 7.2 weeks), full weight-bearing was permitted 7 to 12 weeks after the operation (average, 9.6 weeks).
Preoperative and postoperative Bohler's angle, crucial angle of Gissane, talocalcaneal angle, and the Achilles tendon fulcrum distance were measured and are listed in Table 2. Considering all 103 fractures, the average preoperative Bohler's angle was 1.0 degrees (range, −40 to +21 degrees) and the average angle at follow-up was 21.7 degrees (range, +10 to +35 degrees). The crucial angle of Gissane increased an average of 16.9 degree. The talocalcaneal angle increased an average of 8.0 degrees and the Achilles tendon fulcrum distance increased an average of 3.7 mm.
Broden's views were used to assess reduction of the posterior facet (Fig. 6b). Seventy-one of the fractures were anatomically reduced (68.9 percent), twenty-three had less than 2 mm of displacement (22.3 percent) and five fractures were more than 2 mm displaced. Four fractures were angulated and collapsed at the fracture site (Table 3).
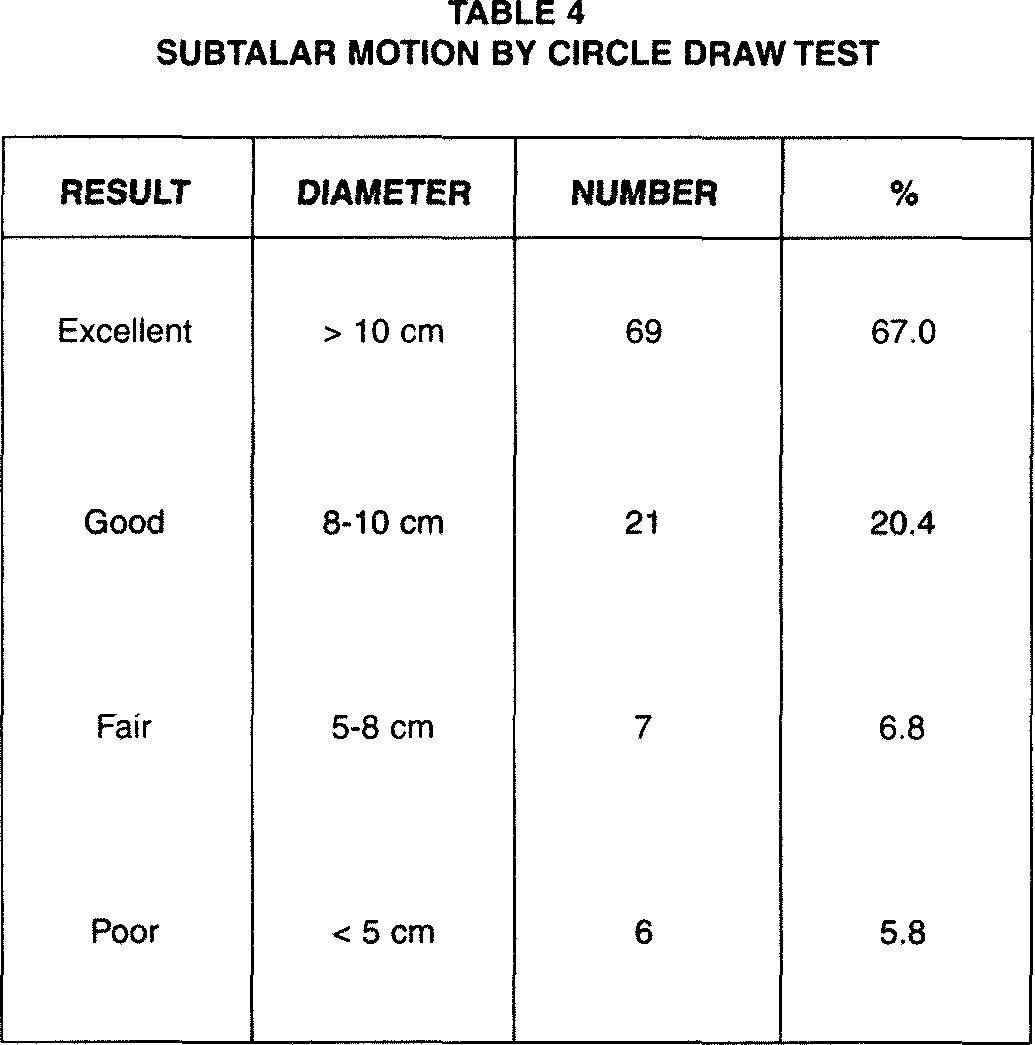
The physical examination of the foot and ankle measured the range of dorsiflexion-plantar flexion and inversion-eversion of the ankle, hindfoot, and forefoot. 10 The range of motion of the subtalar joint was assessed with the “Circle draw test”. The patient sits on the examining table with the legs suspended so that the knees are flexed to 90 degrees and the ankles are in the neutral position. The patient actively circumstructs the foot in as large a circle as possible: The circumference of the circle is drawn and its diameter is used as a measure of forefoot and hindfoot motion, realizing some ankle motion will contribute to the circle's circumference. This diameter is normally roughly 10 cm. Therefore, this value (or above) was used to define an excellent result, motion wise. Sixty-nine feet measured more than 10 cm diameter of the circle and had excellent results; twenty-one feet had good results (range, 8 to 10 cm), seven feet fair results (range, 5 to 8 cm), and six feet poor results (less than 5cm). Ninety fractures (87.4%) had excellent and good results (Table 4).
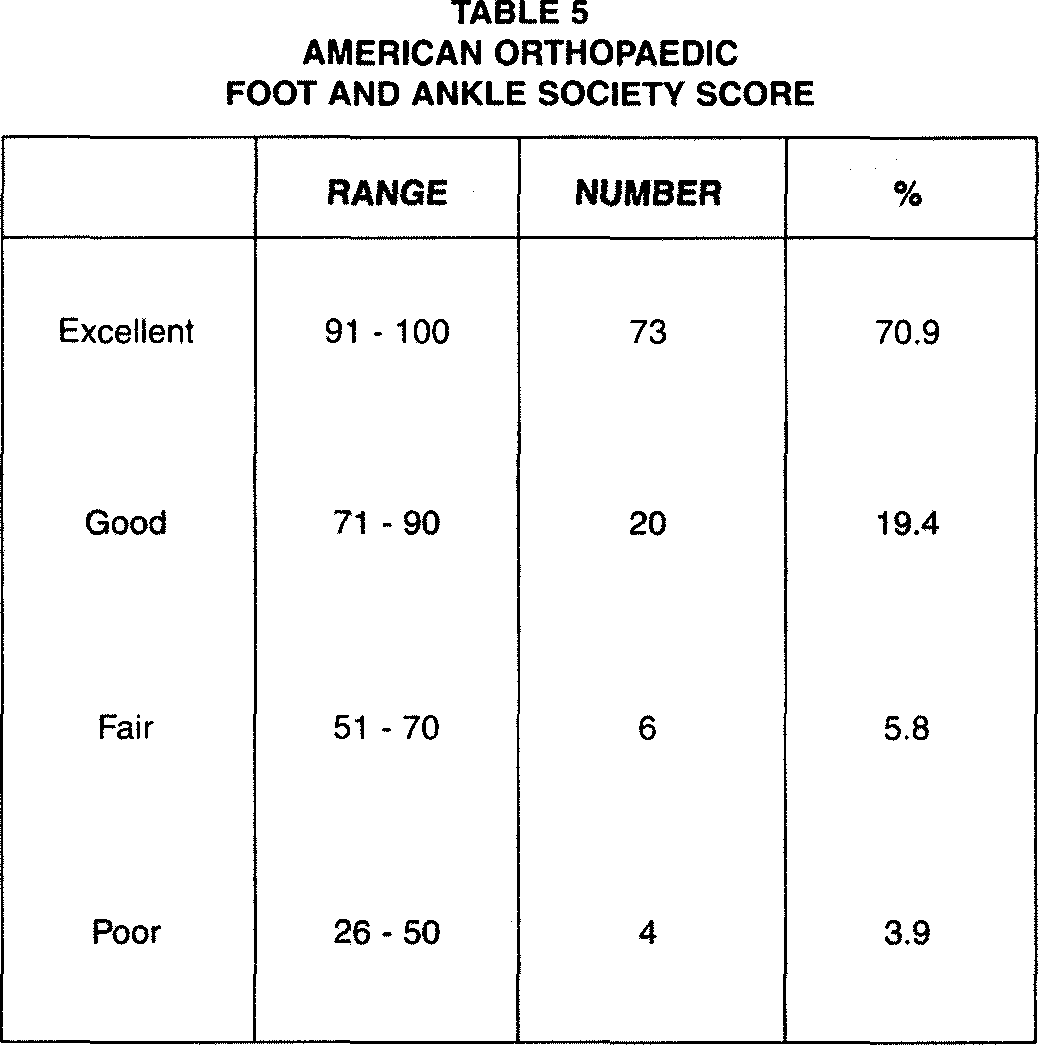
Eighty-nine of the feet have no pain or occasional pain that did not require medication (86.4%). Seventeen feet have persistent swelling. Eighty-eight feet tolerated full weight bearing on the injured extremity. Using the American Orthopaedic Foot and Ankle Society Scoring System for Ankle and Hindfoot, 13 seventy-three of the fractures had excellent results, twenty fractures good, six fractures fair, and four fractures had poor results (Table 5). The result in these patients was classified as poor on the basis of an incomplete anatomical reduction of the posterior facet joint.
Major and minor complications attributable to open reduction and internal fixation through a posterior approach were found in thirteen patients. These complications included minor wound problems, tarsal tunnel syndrome, and calcaneal bony spur. Disruption of the wound margins developed in four feet. All of the wounds healed and none required a graft of skin. 17 One foot with an open and comminuted fracture developed tarsal tunnel syndrome with scar adhesion around the posterior tibial nerve due to the initial open wound. The patient underwent neurolysis of the posterior tibial nerve. Two feet developed a plantar bony excrescence resulting from malunion of the fracture, and were treated by surgical excision of the bone spur. Six fractures had poor results from incomplete anatomical reduction. Four fractures had re-operation with the same technique to restore anatomical alignment. One foot had a subtalar arthrodesis for persistence of pain. The Gallie incision was used again for this arthrodesis.
DISCUSSION
The calcaneus (Os calcis) is the tarsal bone most often fractured. 6 Despite extensive clinical experience with this injury, it is still a major socioeconomic impact in regard to the time lost from work and recreation. In spite of the attention given this fracture for many years by surgeons throughout the world, and recent advances in imaging and operative treatment, often the clinical results following this fracture are poor. This injury virtually always results from an axial load applied to the foot in such a manner that the entire body weight is absorbed by the calcaneus.
The calcaneus initially fractures into two main fragments, with the primary fracture line running from the plantar aspect dorsalward into the posterior facet of the subtalar joint when viewed from the side. On the axial projection, this primary fracture line runs obliquely from plantarmedial to dorsolateral. Two main fracture fragments, an anteromedial and a posterolateral fragment, are produced. 7 The anteromedial (or sustentacular) fragment is rarely comminuted and is of variable size. It remains attached to the talus by the strong deltoid and interosseous talocalcaneal ligaments. The posterolateral (or tuberosity) fragment may be a single, nondisplaced fragment, but, more commonly, it displaces superiorly and laterally, resulting in incongruity of the posterior facet and widening and shortening of the heel. When sufficient force is applied to the heel at impact, comminution of the tuberosity fragment occurs as well. Secondary fracture lines then develop.
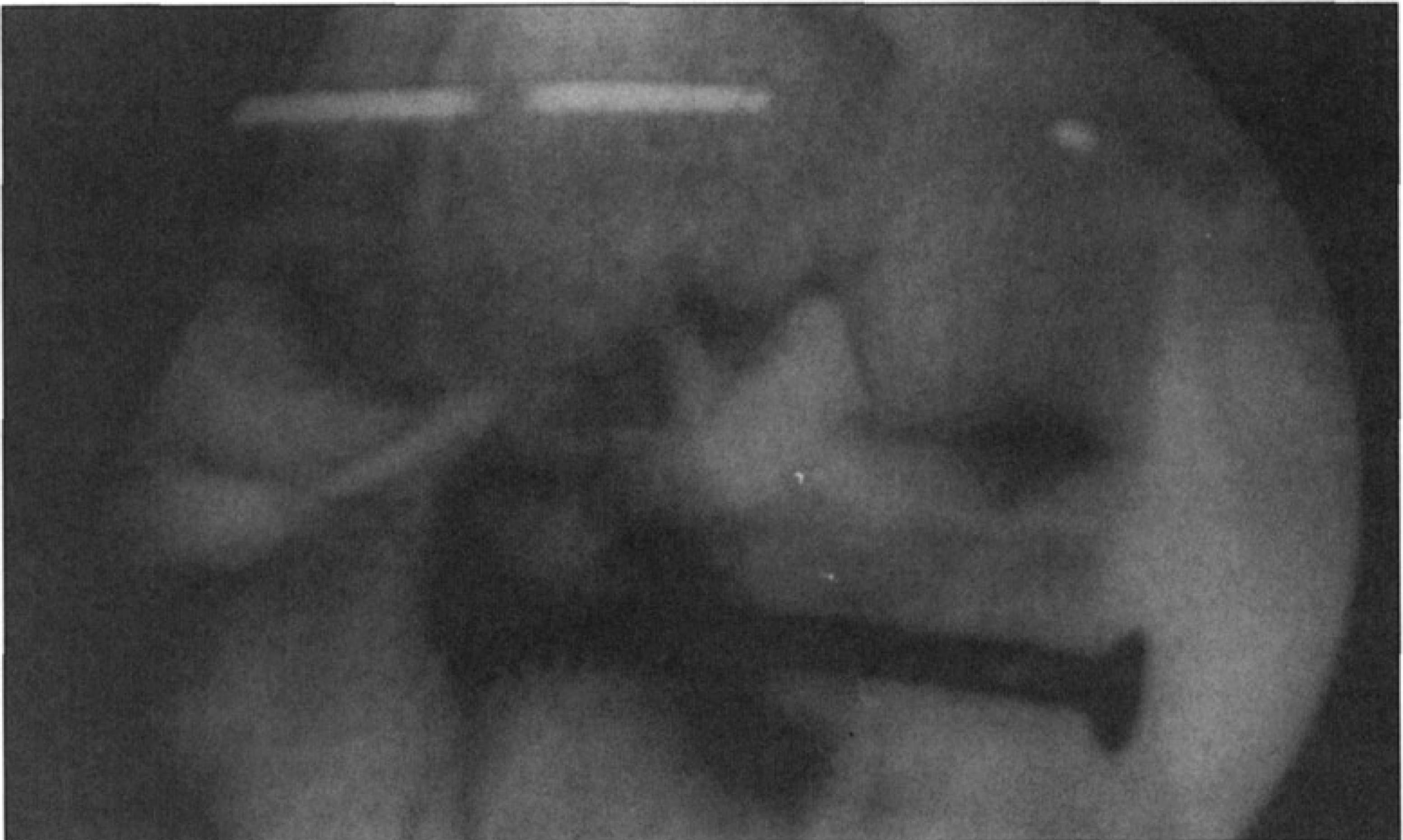
Lateral view shows mildly displaced tongue-type fracture.
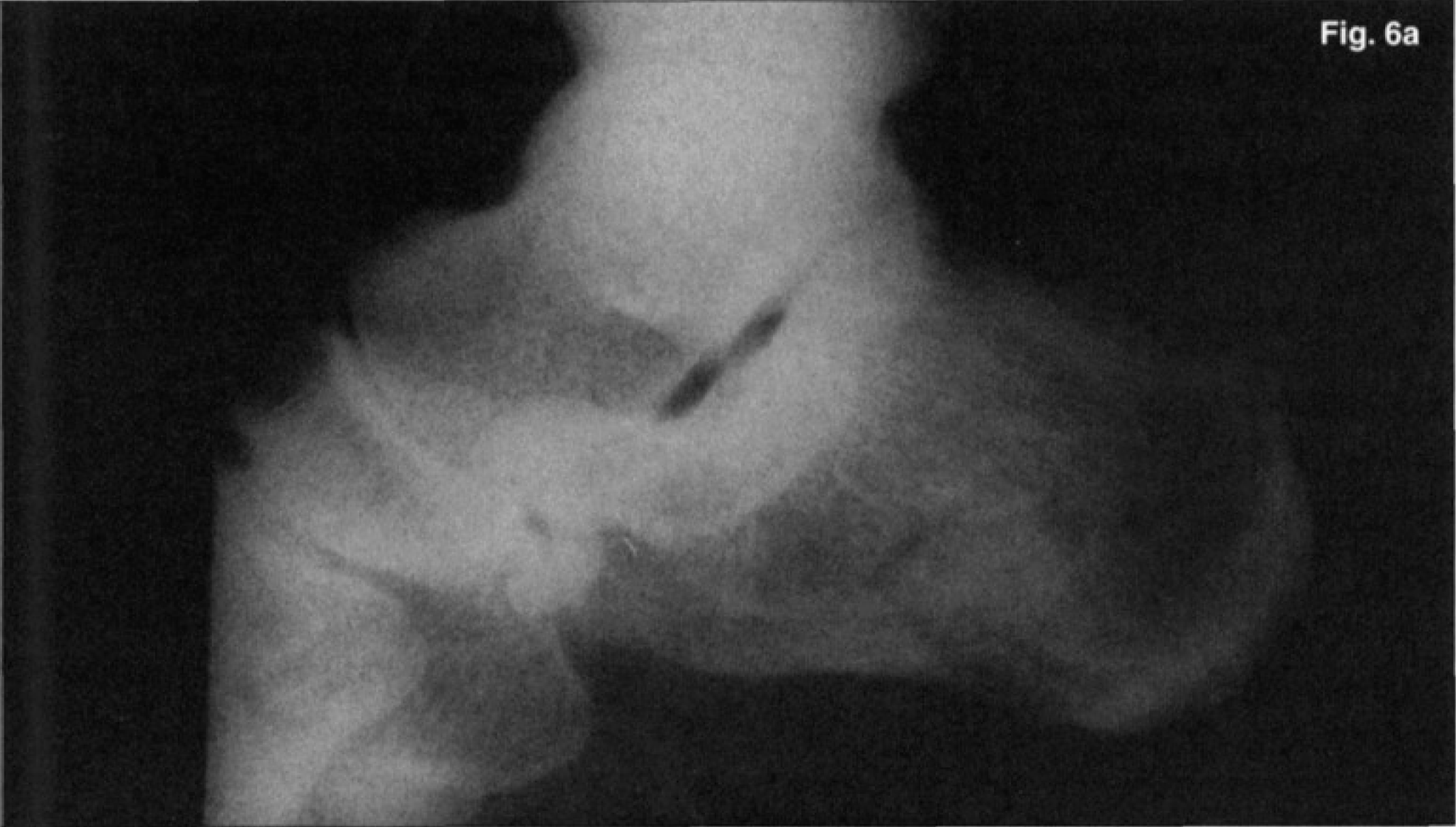
Broden's views show markedly displaced tongue and tuberosity fragments with three main fragments of the calcaneus.
Essex-Lopresti 7 identified two commonly occurring patterns of secondary fracture lines that produce two distinct fracture patterns (the tongue type and the joint depression type). The first, joint depression type involves actual depression of the posterior facet separately from the tuberosity. The second, the so-called tongue type fracture, involves a relative downward rotation of the posterior facet and tuberosity as one fragment.
The major deformities of the fractured calcaneus include (1) loss of height of the calcaneus; (2) increase in width of the calcaneus; (3) decrease in length of the calcaneus; (4) disturbance of the posterior facet; and (5) outward bulge of the lateral wall of the tuberosity fragment. 4 Goals common to all types of treatment of calcaneal fractures are as follow: (1) restoration of congruency of the posterior facet of the subtalar joint, (2) restoration of the height of the calcaneus (the Bohler angle), (3) reduction of the width of the calcaneus, (4) decompression of the subfibular space available for the peroneal tendons, (5) realignment of the tuberosity into a valgus position, and (6) reduction of the calcaneocuboid joint if fractured.
Historically, four general methods of treatment have been proposed: (1) no reduction and early motion; 14,22,23 (2) closed reduction and fixation; 7,12 (3) open reduction and grafting or internal fixation; 1,4,5,15,21,24,25 and (4) primary arthrodesis. 8,9,19 These basic approaches are reviewed to give the reader some perspective on the management of this fracture.
The rationale for non-surgical treatment includes the low incidence of non-union, less scar tissue, less pain, less stiffness, and avoidance of complications of surgical techniques. A soft bulky compressive dressing, elevation, and early range of motion comprise the usual nonsurgical treatment. The results of this treatment regimen can, however, be poor because of loss of subtalar motion, pain, and subfibular tissue impingement. 17,20
Proponents of open reduction correctly insist that direct manipulation of the articular fragments is the only means of achieving reduction of the posterior facet, an essential first step in restoring function of the subtalar joint. Two basic approaches have been used either separately or together.
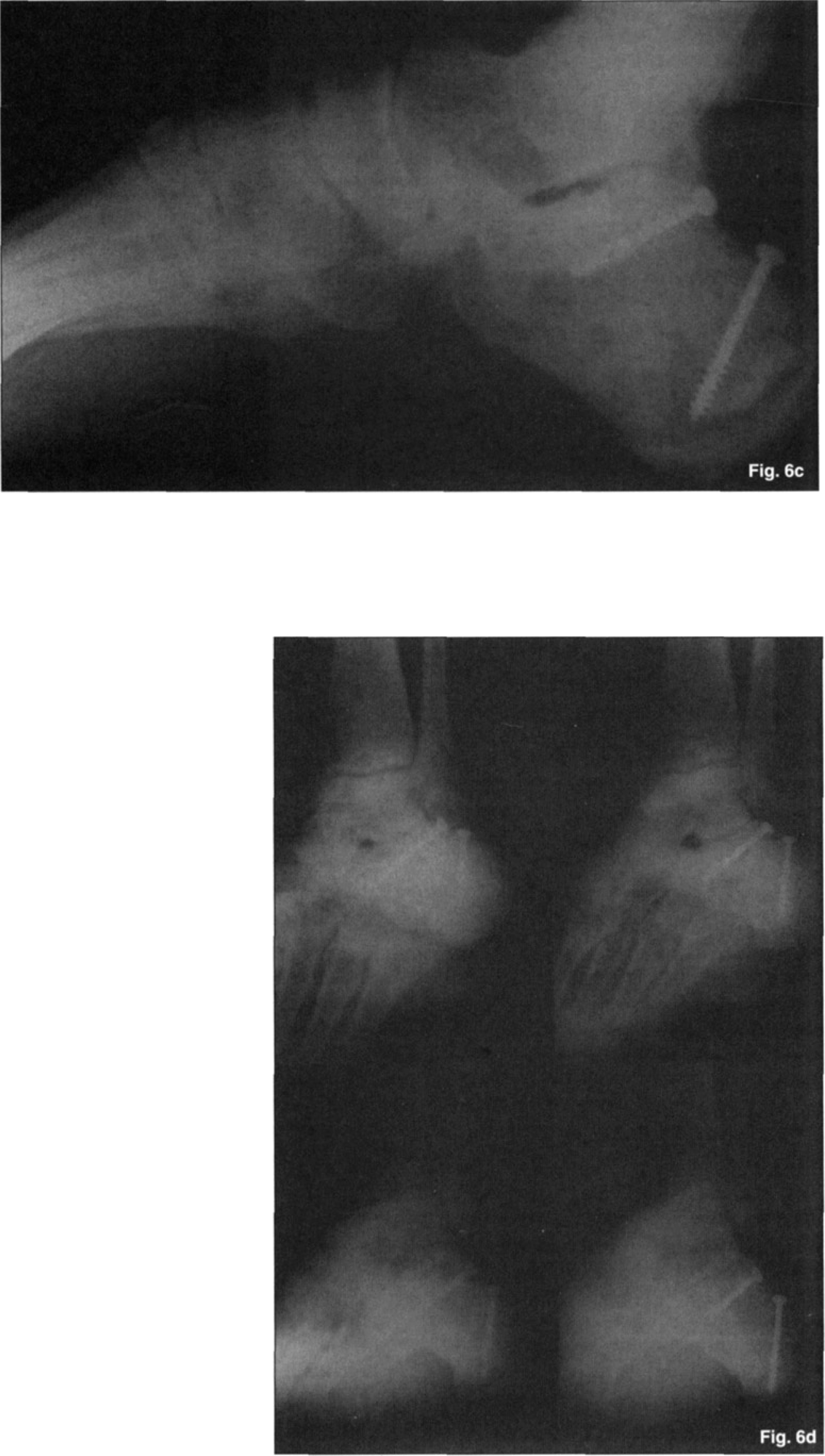
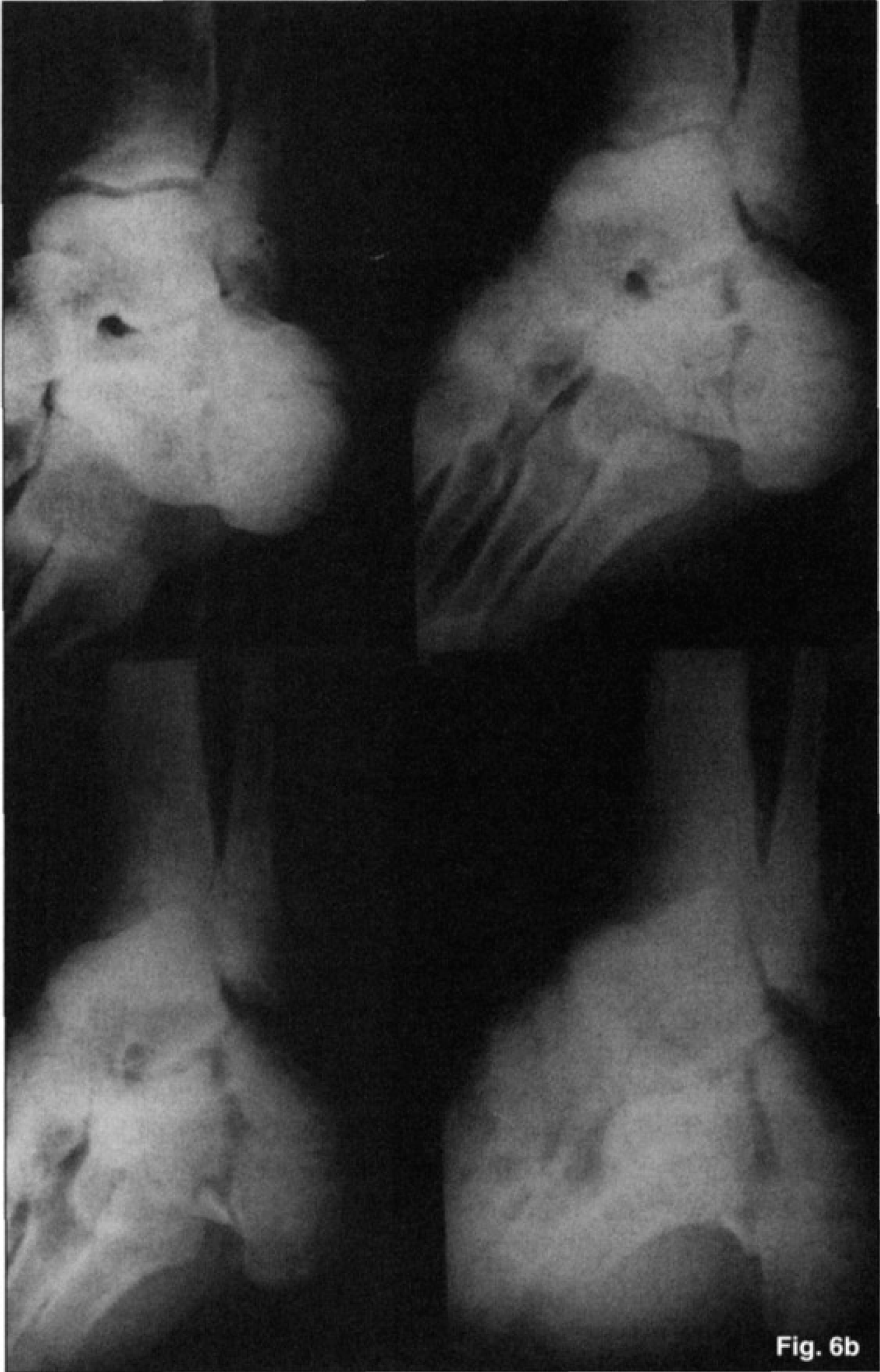
At 3 months after operation, lateral and Broden's views show excellent reduction and fixation of the fracture fragments and a well aligned posterior facet.
SUBTALAR MOTION BY CIRCLE DRAW TEST
McReynolds introduced the medial approach, which has been strongly advocated by Burdeaux. 4 Advantages of the medial approach include clear observation of the medial fracture line, easier reduction of the sustentaculum fragment, easier measurement of heel height, decreased soft tissue dissection, and good bone for internal fixation. Disadvantages include a potential problem for injuring the neurovascular structures (especially the calcaneal branch of the tibial nerve) due to dissecting around the neurovascular bundle, lack of adequate visualization of the subtalar joint and blind reduction of the posterior talocalcaneal joint, limited room for fixation, lack of ability to extend the wound, and limited exposure to the anterior aspect of the calcaneus and calcaneocuboid joint. 17,20
The lateral approach has been strongly advocated by Palmer 21 and others. Benirschke and Sangeorzan 1 have recommended extensive right angle lateral incision. The lateral extensile exposure technique has become very popular, especially among foot and ankle surgeons and traumatologists. Advantages include visualization of the subtalar joint, allowing more accurate reduction of the facet fragment, ability to decompress the lateral wall, access to the calcaneocuboid joint, and sufficient area laterally for plate fixation. Disadvantages include a greater amount of soft tissue dissection with potential for malreduction of the sustentacular fragment, higher incidence of wound problems and skin necrosis and deep wound infection, injury to the sural nerve, poor bone fixation due to the cortical comminution of the lateral wall, and inability to directly assess reduction of the medial wall and thus inability to accurately assess restoration of the height and length of the calcaneus. 15,17 Soft tissue problems, particularly wound edge necrosis and deep wound infections, further mitigate against the use of this approach.
AMERICAN ORTHOPAEDIC FOOT AND ANKLE SOCIETY SCORE
The posterior approach has not been introduced for treating displaced intra-articular calcaneal fractures. In 1943, Gallie 8 described a posterior approach to the subtalar joint for subtalar fusion. This study has used this posterior approach for open reduction and internal fixation of displaced intra-articular calcaneal fractures. In this series, 90% of the cases had good or excellent functional results.
As compared with the medial approach, the advantage of the posterior approach is visualizing the entire posterior facet of the calcaneus, without risk of injury of the major neurovascular structures, as well as identification of the displaced or the depressed fragment of the articular surface of the posterior facet without extending the incision onto the foot. Therefore, the sustentacular fragment and the tongue fragment can be seen well, reduced and internally fixed.
Compared with the lateral approach, the posterior incision should not further injure the lateral cortex of the calcaneus nor the peroneal tendons. In addition to lack of marginal necrosis of the wound at the apex of the extensile incision as well as avoiding the large exposure to place a plate are avoided.
The lateral wall bulge is reduced by pressure on both sides of the calcaneus with a compression device. Almost normal width of the heel was obtainable by this method, without impingement on the peroneal tendons by a plate and screws.
The evaluation of the results at follow-up was based on the adequacy of the reduction, the restoration of motion of the subtalar joint, and the ability of the patient to return to work.
The radiographs were measured as follow: Bohler's angle, crucial angle of Gissane, talocalcaneal angle, the Achilles tendon fulcrum distance, the width of lateral bulge, and efficacy of reduction of posterior facet. 18 CT scan gives information about the articular surface of the posterior facet, the sustentaculum, calcaneal cuboid joint, the shape of the heel, and the position of the peroneal and flexor hallucis tendons. Initially CT scan had been taken for evaluation of subtalar joint, but Broden's views could give enough information as CT showed. In this study, CT scans have not been routinely used. Because plain films and Broden's views have been sufficient for planning surgery 4,5,24 , as well as intraoperative evaluation of the posterior facet by direct vision of the articular surfaces, and the radiographic costs have been reduced. If the fracture(s) cannot be visualized sufficiently to plan the surgical procedure, then CT scans should be obtained.
The final physical examination emphasized range of motion of the subtalar joint and the location of the tenderness. Because of its complexity, the subtalar joint has historically been difficult to assess both clinically and radiographically. 11 This difficulty is evidenced by the numerous studies that have been dedicated to the radiographic determination, the biomechanical analysis, and the measurement of movement at the subtalar joint. 18,20 The importance of subtalar movement has been related to its capacity to allow the foot to adapt to uneven terrain during bipedal ambulating. 26 The advantages of clinical measure are its simplicity and portability. 10 For this reason, measurement of subtalar joint motion has been widely used as an outcome measure following certain fractures and subsequent treatments. We evaluated the range of motion of the subtalar joint with “Circle draw test” for physical evaluation. The Circle draw test demonstrated plantarflexion-supination-adduction and dorsiflexion-pronation-abduction of the subtalar and ankle joint coupling. The American Orthopaedic Foot and Ankle Society Scoring System for the Ankle and Hindfoot was used for this study.
CONCLUSION
Intra-articular calcaneal fractures are severe injuries with long-term effects on function. When all results are compared, open reduction and internal fixation techniques yield the best results when anatomic restoration of the subtalar joint is achieved. This review lead to recommendation of the Gallie incision (straight posterior-lateral) for open reduction and internal fixation of displaced intra-articular calcaneal fractures.
No major structure can be damaged except the sural nerve.
Good exposure of the posterior talocalcaneal joint.
Reduction of articular fragments under direct vision.
Straight forward internal fixation of the fracture(s) of the posterior facet and tuberosity
Less extensive soft tissue dissection and less chance of major wound problems.