
Abstract
Eighty six subtalar arthrodeses performed between 1985 and 1996 for complications associated with intra-articular calcaneal fractures were retrospectively evaluated. Patients were divided into three Groups: (I) 59 patients with calcaneal malunions (II) 13 patients with failed open reduction and internal fixation, and (III) eight patients undergoing open reductions and primary fusion for highly comminuted fractures. In each scenario, internal fixation was achieved with cancellous lag screws. Bone graft material consisted of either autogenous iliac crest graft, local graft obtained from the lateral wall exostectomy of the malunion, or freeze-dried cancellous allograft. Fusions in Groups II and III were performed in situ. Fusions in Group I were performed either in situ or utilizing a variety of reconstructive procedures depending upon the type of malunion encountered. Eighty three of the 86 fusion attempts were successful following the initial operations for a union rate of 96%. Fusion rates were similar regardless of the graft material used. Complications included four varus malunions, four cases of osteomyelitis, and two cases of reflex sympathetic dystrophy. A statistically significant shorter hospital stay was found for patients not undergoing iliac crest bone graft procedures. Eighty patients with at least two year follow up achieved a mean American Orthopaedic Foot and Ankle Society(AOFAS) ankle-hindfoot score of 75.0. Scores were similar for all three groups and for the various types of reconstructive procedures used. No correlation was found between postoperative talar declination angle and the AOFAS ankle-hindfoot score. Worker's compensation patients tended to have a poorer clinical outcome.
INTRODUCTION
Posttraumatic subtalar arthritis is a well recognized complication of intra-articular calcaneal fractures.1,2,5,7,15,17,20,21,23 This may occur as a result of a calcaneal malunion1,2,5,6,7,14,20 or in spite of adequate open reduction and internal fixation.17,20,21 Subtalar arthrodesis has been advocated as a means of relieving this painful condition.1,2,5,6,14,17,18,23
Subtalar fusion has also been advocated as a primary treatment for highly comminuted fractures where the joint surface cannot be adequately reconstructed.9,10,11 Recently, open reduction and internal fixation combined with primary subtalar arthrodesis has been suggested as an effective treatment for these extremely difficult fractures.17,20
With malunions, the calcaneus is shortened, widened, and frequently malaligned. Several authors have described complex osteotomies and the use of interpositional bone grafts in an attempt to restore the anatomical relationships of the hindfoot.2,5,6,7,18,23 Others have argued that complete correction of the hindfoot at the time of subtalar arthrodesis is not necessary to obtain a successful clinical result.8,23 Still others have found better clinical results with fractures which were intially treated with open reduction and internal fixation prior to subtalar arthrodesis versus the reconstruction required with a calcaneal malunion. 25 To date, studies concerning these issues have consisted of small numbers of patients and have failed to compare all of the indications for subtalar arthrodesis following calcaneal fractures.
Controversy also exists regarding the use of additional bone graft at the time of subtalar arthrodesis. High fusion rates have been reported when autogenous iliac crest bone graft is used to supplement subtalar arthrodesis.1,5,13,16,19 However, harvesting iliac crest graft has been shown to have significant donor site morbidity, greater blood loss, and higher hospital costs. 13,16,24 The use of local bone graft or allograft eliminates donor site complications and possibly speeds patient recovery, therefore decreasing hospital costs. Although the use of local graft or allograft presents an attractive alternative, the literature on their use in hindfoot fusions is limited.13,15,16
The purpose of this study was to review and compare our experience with subtalar arthrodesis in a large series of patients separated into three groups: (1) patients with calcaneal malunions (2) patients with failed open reduction and internal fixation (3) patients undergoing open reduction and primary fusion for highly comminuted fractures. In each case internal fixation with large cancellous screws was used, however, bone graft material varied with either iliac crest graft, local bone graft, freeze-dried cancellous allograft or a combination of graft materials.
METHODS AND MATERIALS
Between 1985 and 1996, 136 hindfoot fusions in 129 patients were performed by the senior authors (R.W.S. and A.K.W.) secondary to either posttraumatic arthritis related to an intra-articular calcaneal fracture or as a primary procedure due to highly comminuted calcaneal fractures. One hundred eightteen patients were at least two years postoperative following their fusions. Thirteen patients with other ipsilateral fractures of the foot and ankle were excluded and 24 others were lost to follow up. Twenty two of the these 24 could not be located and two were deceased from unrelated causes. One patient from Group III required a Symes amputation prior to union secondary to persistent infection. This left 80 patients with 86 subtalar arthrodeses for evaluation. Of these 86 fusions, 62 (59 patients) were performed secondary to calcaneal malunions (Group I), 16 (13 patients) for failed open reduction and internal fixation (Group II), and 8 (8 patients) secondary to severely comminuted fractures (Group III).
All patients in Group I had been referred to the senior authors after developing calcaneal malunions following failure of initial nonoperative treatment or limited internal fixation. Initial fracture management of patients in Groups II and III was by the senior authors.
Bone Graft Materials
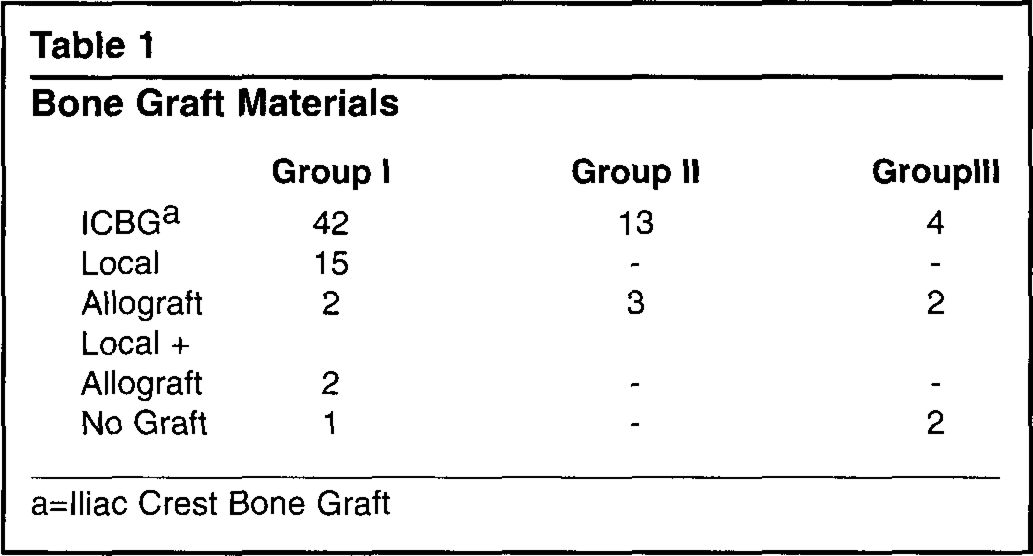
=lliac Crest Bone Graft
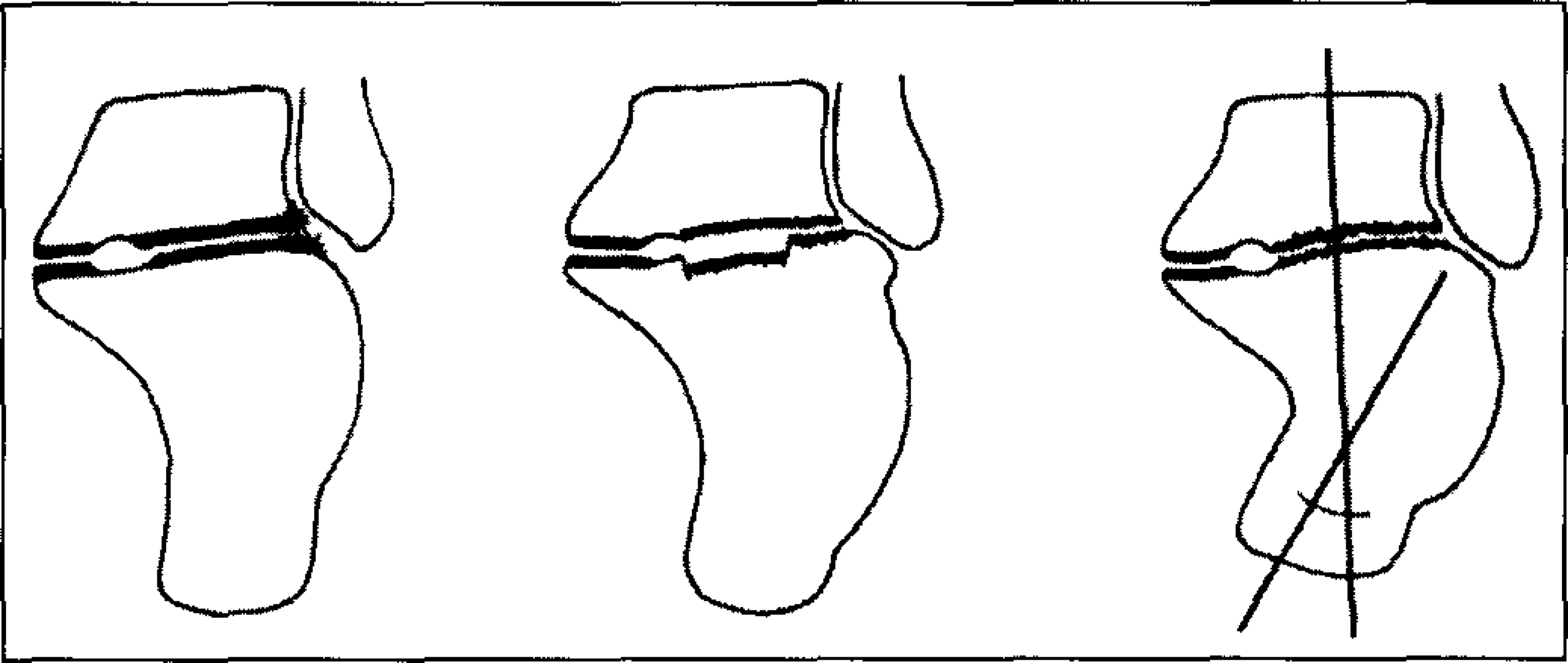
Schematic representations of the three types of calcaneal malunions. (With permission from
Preoperative bilateral transverse and coronal CT scans were obtained on all patients. For patients in Group I these were used to classify the malunion. In Group II these were used to confirm the presence of subtalar joint arthritis and evaluate that the calcaneal height and width were anatomic or near anatomic. For patients in Group III CT scans were used to evaluate the fracture and aid in preoperative planning.
Classifications
Malunions were classified according to a computed tomography system developed by one of the senior authors (R.W.S.) and previously presented (Figure 1). 23 This system places malunions into one of three types. Type I malunions have a large lateral wall exostosis but no subtalar arthritis, Type II have a large lateral wall exostosis with significant subtalar arthritis and Type III malunions include a lateral exostosis, significant subtalar arthritis, and calcaneal body malalignment of greater then 10 degrees of hindfoot varus. Of 62 malunions in this study 36 were Type II and 26 Type III.
Acute fractures treated at our institution were also classified according to a system developed by one of the senior authors (R.W.S.) and based on the amount of comminution of the posterior facet. 21 Type I fractures are nondisplaced, Type II have two part displaced fractures of the posterior facet, Type III fractures are three part fractures and Type IV have four or more parts. All fractures in Group II were Type II or Type III. Group III consisted of only Type IV fractures.
Mechanism of Injury
The mechanism of injury for 58 of the 80 patients was a fall. Twenty others were involved in motor vehicle accidents and the remaining two were injured in sporting activities. Fourteen patients suffered other orthopaedic injuries at the time of their calcaneal fractures.
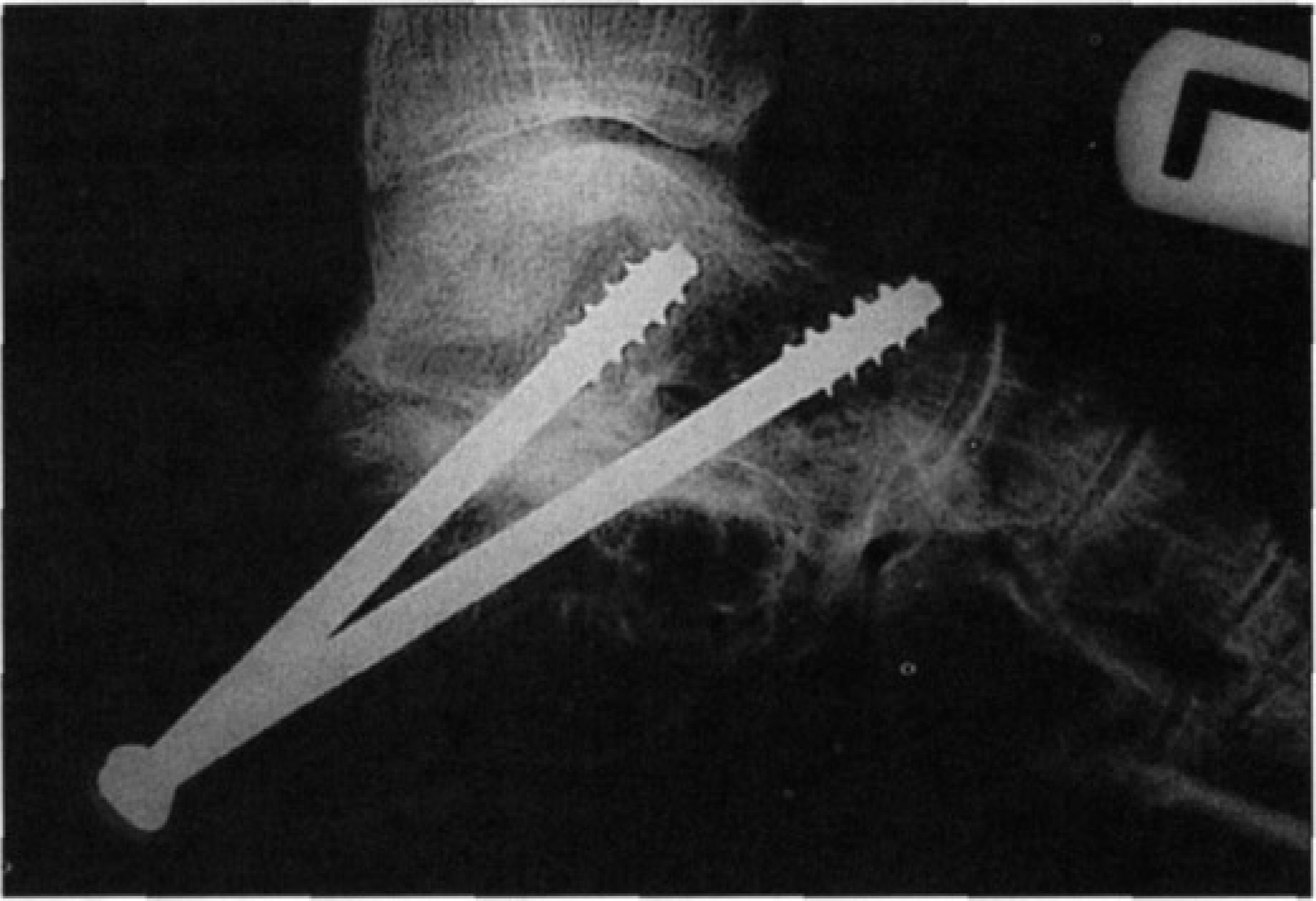
Lateral postoperative radiograph demonstrating placement of subtalar screws.
Operative Indications
All patients in Group I and II were preoperatively evaluated with weightbearing anterior posterior and lateral radiographs as well as CT scans. Subtalar arthrodesis was indicated for those patients with pain localized to the hindfoot whose preoperative radiographic studies showed significant subtalar arthritis. All patients had failed nonsurgical management which included activity change, shoe modifications, and anti-inflammatory medications. If in any case the diagnosis was in question patients were given an injection of lidocaine into the subtalar joint under fluoroscopic guidance. Patients without significant radiographic evidence of subtalar arthritis who also did not achieve adequate relief of symptoms following injection were not considered for surgery.
Primary fusion was indicated for Type IV fractures when a congruous reconstruction of the posterior facet could not be achieved. In all cases preoperative CT scans had suggested that a fusion may be necessary and the patients informed consent was obtained.
Patient Data
Of the Group I patients there were 42 males and 17 females with an average age of 45 years (range, 23 to 66 years). Time from injury to fusion averaged 24 months (range, 4 months to 30 years). Eight of the malunions were initially treated with limited internal fixation and the remaining 54 had been treated nonoperatively. Two of the fusions were revisions of previously attempted subtalar fusions by other orthopaedic surgeons which had gone on to nonunions.
In Group II there were 12 males and one female. Average age was 42 years (range, 24 to 68 years). Time from initial open reduction to fusion averaged 16 months (range, 5 to 48 months). Six of the 16 feet had had calcaneal plate removal and joint exploration as a previous procedure.
For Group III patients, there were 6 males and 2 females. Average age was 36 years (range, 19–69). Surgery was delayed an average of 17 days (range, 9 to 30 days) to allow for adequate soft tissue healing.
A retrospective clinical and radiographic analysis of those patients with at least two year follow up was performed. All patients were examined by one of three physicians (R.W.S., A.K.W. or A. S. F.). In addition, a detailed history regarding patients pain, function, narcotics use, employment, and level of satisfaction was obtained. Patients covered under worker's compensation insurance were noted. The medical records, pre and post operative radiographs, and CT scans of each of the 86 fusions were evaluated. Union rate, perioperative complications, and length of hospitalization were recorded.
Clinical Evaluation
Patients were scored according to the American Orthopaedic Foot and Ankle Society's (AOFAS) ankle -hindfoot scale. 12 This is a 100 point scale which assigns 40 points for pain, 50 points for function, and 10 points for alignment. Due to the expected loss of hindfoot motion, the maximum score in this study was 94 points. Although nonnumerical gradings (e.g. excellent, good, poor) are not assigned with this system we graded any patient scoring 69 or greater as a satisfactory result.
Radiographic Evaluation
All 86 fusions were evaluated with serial lateral and axial views of the calcaneus. In addition, weightbearing anterior posterior and lateral radiographs were also obtained at final follow up. All fusions were evaluated for union and gross changes in alignment. Lateral weight-bearing radiographs were evaluated for talocalcaneal height and talar declination angle according to methods previously described.4,6
Operative Technique
All patients undergoing unilateral fusions were positioned in the lateral decubitus position on a radiolucent table. Three patients underwent bilateral procedures with a single draping. These three patients were placed in the prone position which allowed access laterally to both feet.
A Seattle modified Kocher incision3,20,21 was used in all cases. This incision is an extensile right-angled incision which allows a thick flap to be lifted from the subperiosteal surface of the lateral calcaneal wall.
For all Type II and III calcaneal malunions, the lateral wall exostosis was removed with an oscillating saw and saved for later use. Sharp periosteal elevators and curettes were used to denude the articular surfaces with care being taken to maintain the contour of the subtalar joint. Bone graft, if used, was then placed into the subtalar joint. Two cannulated cancellous lag screws were then placed in a retrograde fashion from the calcaneal tuberosity across the subtalar joint with the joint being held in slight valgus. (Figure 2) During this study screw sizes used included thread widths of 6.5, 7.0, and 7.3 millimeters.
A bone block fusion was indicated based on the surgeon's perception of severe hindfoot shortening. If a bone block arthrodesis was performed, distraction was obtained with the use of either a medially placed femoral distractor, a laterally placed large bone spreader, or both.
For Type III malunions with remaining hindfoot varus following joint correction, a lateral closing wedge osteotomy was also required. The osteotomy was performed through the calcaneal body up to but not through the medial cortex. Wedges of 5–10 mm were removed depending on the degree of hindfoot varus. The osteotomy was then closed and screws were placed across the osteotomy site and the denuded subtalar joint. In this study 6 patients required a calcaneal osteotomy. In one other patient with excessive calcaneal shortening and heel varus, an osteotomy was done through the primary fracture line using both medial and lateral incisions. This was a modification of a previously described technique. 18
Fusions required for failure of open reduction and internal fixation were all performed in situ. The operative approach, method of cartilage removal, and screw placement were as described above. No lateral wall exostectomies or calcaneal osteotomies were required. Previously placed hardware, if present, was removed prior to screw placement.
Primary fusions were also performed in situ following open reduction and rigid internal fixation the technique for which has been well described.4,20,21 Two screws were preferred however, in some cases the fracture pattern would allow the placement of only one screw. (Figure 3)
Of the fusions in Group I, two of 15 local grafts were placed as a bone blocks to restore talocalcaneal height. Twenty — four of the 42 iliac crest grafts used were tricortical bone blocks and the remainder were cancellous.
Postoperative Care
Patients were treated for approximately 8 weeks in a partial weightbearing short leg cast. Progressive weightbearing was then begun usually in a removable prefabricated walker boot. After 12 weeks most patients were weightbearing as tolerated and physical therapy for strengthening and ankle range of motion was begun.
Statistical Analysis
A Pearson correlation coefficient was used to assess the relationship between postoperative talar declination angles and AOFAS ankle- hindfoot scores. Differences between groups were assessed using analysis of variance. The Student's t-test was used to determine differences within subgroups. In all cases, statistical significance was set at p < 0.05.
RESULTS
Union
Patients were considered to have a successful subtalar fusion if: (1) they were able to ambulate comfortably without immobilization (2) hindfoot motion could not be detected on clinical exam (3) there was evidence of trabeculation across the athrodesis site on plain radiographs. Patients who did not meet these criteria were examined under fluoroscopy to further determine union. If no motion was detected to inversion and eversion stress the arthrodesis was considered solid.
Bone Grafting
Three different bone graft materials were used either alone or in combination to supplement fusions. (Table 1) These included local bone graft from the lateral wall exostectomy or calcaneal osteotomy, autogenous iliac crest bone graft either tricortical or cancellous and freeze dried cancellous allograft. In three cases joint surfaces were felt to be congruent enough that no bone graft was required.
Malunion Results
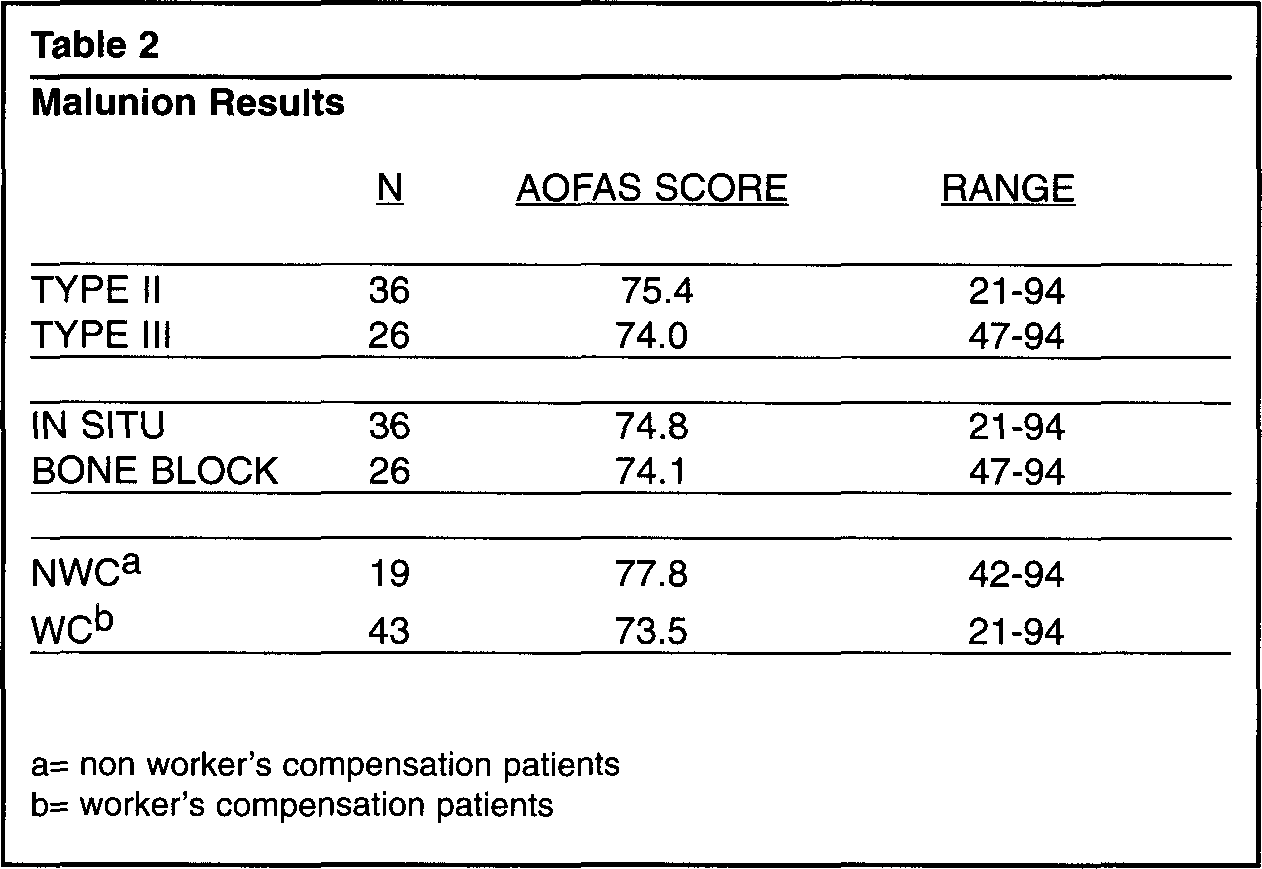
= non worker's compensation patients
= worker's compensation patients
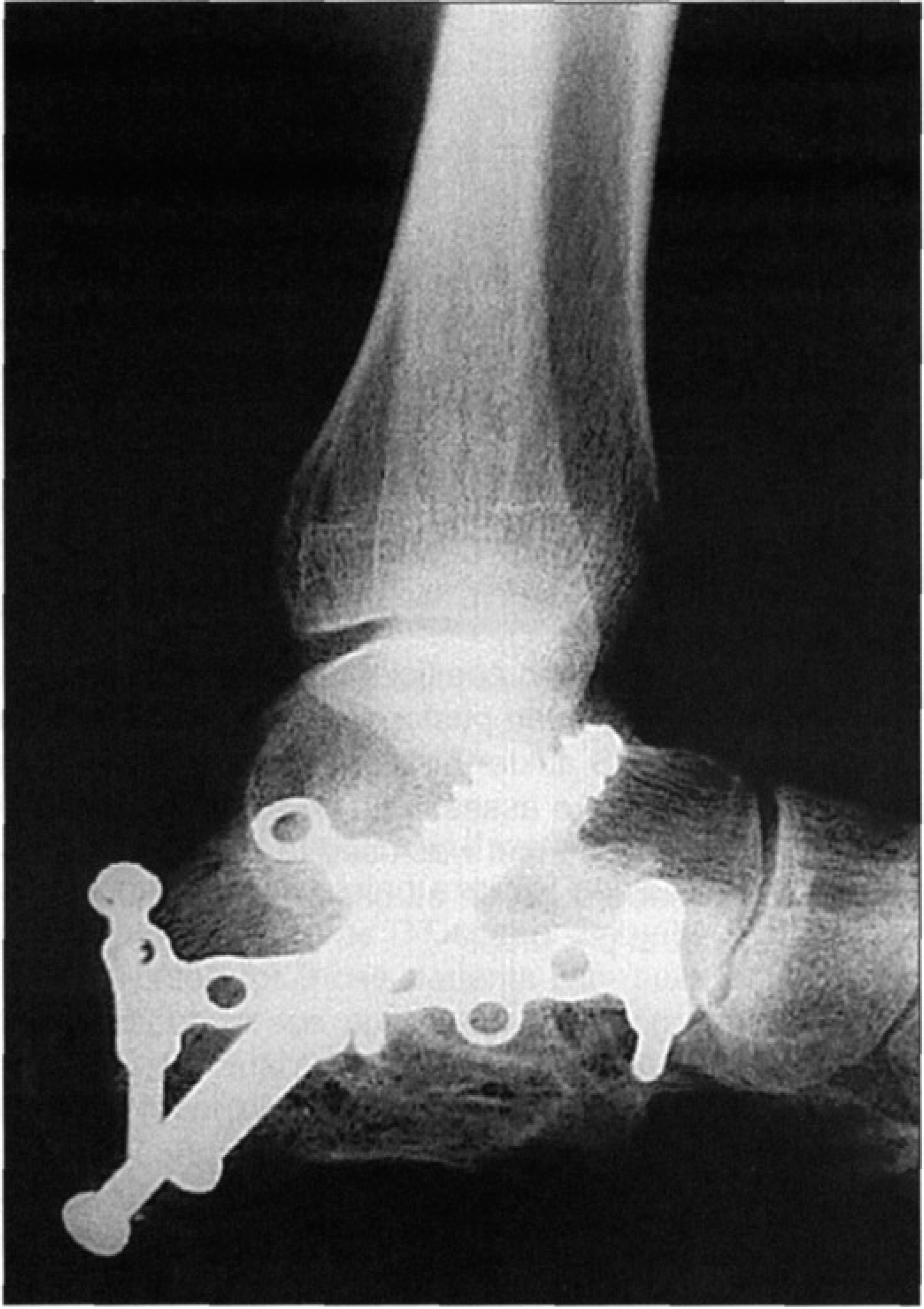
Lateral postoperative radiograph showing screw placement for primary fusion.
Of the 86 fusions 83 were united within four months, for a union rate of 96%. All three nonunions occurred in patients in Group I. One had been supplemented with a tricortical iliac crest graft used as a bone block, one received local graft, and in the other no graft was used. All 3 were successfully revised; 2 with ICBG and one with allograft.
Clinical Followup
(Group I): Fifty-nine of a possible 65 patients (62 of 68 feet) with at least two year follow up were available for evaluation at an average of 50 months (range, 24–156 months). Forty-one patients (43 fusions) were involved in worker's compensation claims.
The overall AOFAS ankle — hindfoot score for all 62 fusions was 74.8 (range 21 to 94). Scores based on malunion classification (Type II versus Type III), arthrodesis technique used (in situ versus bone block), and patient population (non worker's compensation versus worker's compensation), are listed. (Table 2) Differences within these subgroups were not statistically significant.
Of the 62 feet, 50 scored 69 points or greater. Fifty patients (85%) were satisfied with their outcome. Sixteen of 18 non worker's compensation patients and 26 of 41 worker's compensation patients returned to work.
Of the 12 patients who scored less than 69 points, 9 were worker's compensation patients. Six of these 12 patients had some other documented condition which influenced their result. Two patients suffered from lumbar radiculopathy, which radiated into their operative foot and one had a painful peripheral neuropathy secondary to chemotherapy for adenocarcinoma. Two suffered from a postoperative reflex sympathetic dystrophy. Another patient had severely symptomatic calcaneocuboid joint arthritis and was offered conversion to a triple arthrodesis but had refused. In the remaining 6 patients with less than satisfactory results, radiographic and clinical exam were unremarkable and no reason for their poor outcome could be determined.
(Group II): Follow-up was possible in 13 of 16 patients (16 of 19 feet) at an average of 48 months (range, 24 to 94 months). The AOFAS ankle-hindfoot score for the group averaged 75.2 (range, 52 to 91). Thirteen fusions in 10 worker's compensation patients scored an average of 75.0 (range, 52 to 91). The three other patients scored an average 75.3 (range, 57 to 82). Thirteen feet scored at least 69 points. All 13 patients were satisfied with their outcome. One of 3 non worker's compensation returned to work and 7 of 10 worker's compensation patients returned to work.
Of the 3 patients not scoring at least 69 points, 2 had other orthopaedic problems which contributed to their pain. One suffered from a lumbar radiculopathy and the other had more pain from a contralateral calcaneal fracture which had undergone open reduction and internal fixation but had not had a subtalar fusion. All three patients were involved in worker's compensation cases.
(Group III): Eight of 12 possible patients with at least two year followup were available. Average follow up was 34 months (range, 24 to 55 months). Two of 8 patients were covered under worker's compensation. The average AOFAS ankle-hindfoot score for the Group was 75.4 (range, 48 to 88). The two worker's compensation patients had a scores of 48 and 69. Scores of the other 6 patients averaged 81.3. Seven of 8 patients had scores of 69 or greater. Six of 8 were satisfied with the result of their fusion. The six non worker's compensation patients all returned to work. Neither of the worker's compensation patients, both construction workers, returned to work. One was entered into vocational rehabilitation and the other who had suffered calcaneal osteomyelitis as a complication of his fusion was disabled.
The average AOFAS ankle-hindfoot score for all three groups was 75.0. Differences between groups were not statistically significant. The average score for fusions in worker's compensation patients was 73.5 and for fusions in non worker's compensation patients the average score was 77.8. This difference approached but did not reach statistical significance(p= 0.12). Thirty-three of 53 (62%) worker's compensation patients returned to work versus 23 of 27 (85%) of non worker's compensation patients. No patient in either of the groups was still taking narcotic analgesics at the time of latest follow up.
COMPLICATIONS
(Group I): There was one case of osteomyelitis which resolved with serial debridements and long term IV antibiotics. There were 3 varus malunions that required reoperation. All 3 patients had undergone bone block arthrodesis with tricortical iliac crest graft. All 3 patients were treated with a lateral closing wedge osteotomy with resolution of their symptoms. There were 3 nonunions as previously described and 2 patients developed reflex sympathetic dystrophy.
(Group II): One patient developed an osteomyelitis. This was an individual with diabetes who was insulin dependent. He had a deep wound infection at the time of his initial open reduction. This was treated with serial debridements and intravenous antibiotics. The infection was felt to be resolved. Eight months later he underwent a subtalar arthrodesis with iliac crest graft. Interestingly, he did not present with calcaneal osteomyelitis until two years his after fusion. He was successfully treated with serial debridements, distant flap coverage, and intravenous antibiotics.
(Group III): There were two cases of osteomyelitis including the patient who required the Symes amputation. One patient had received iliac crest bone graft and one allograft. The patient who received iliac crest bone graft required the Symes amputation due to uncontrolled infection. The patient in the allograft group responded to serial debridements, distant flap coverage, and intravenous antibiotics.
There was one symptomatic varus malunion which required reoperation. This was treated with a lateral closing wedge osteotomy with resolution of the patients symptoms. Ten patients from Group I, 5 patients from Group II, and 1 patient from Group III required hardware removal for persistent heel pain localized over the screw heads.
There was one wound complication in 59 iliac crest donor sites. This was a fascial herniation which required reoperation. One other patient continued to experience pain localized to his anterior donor site more than three years after his fusion.
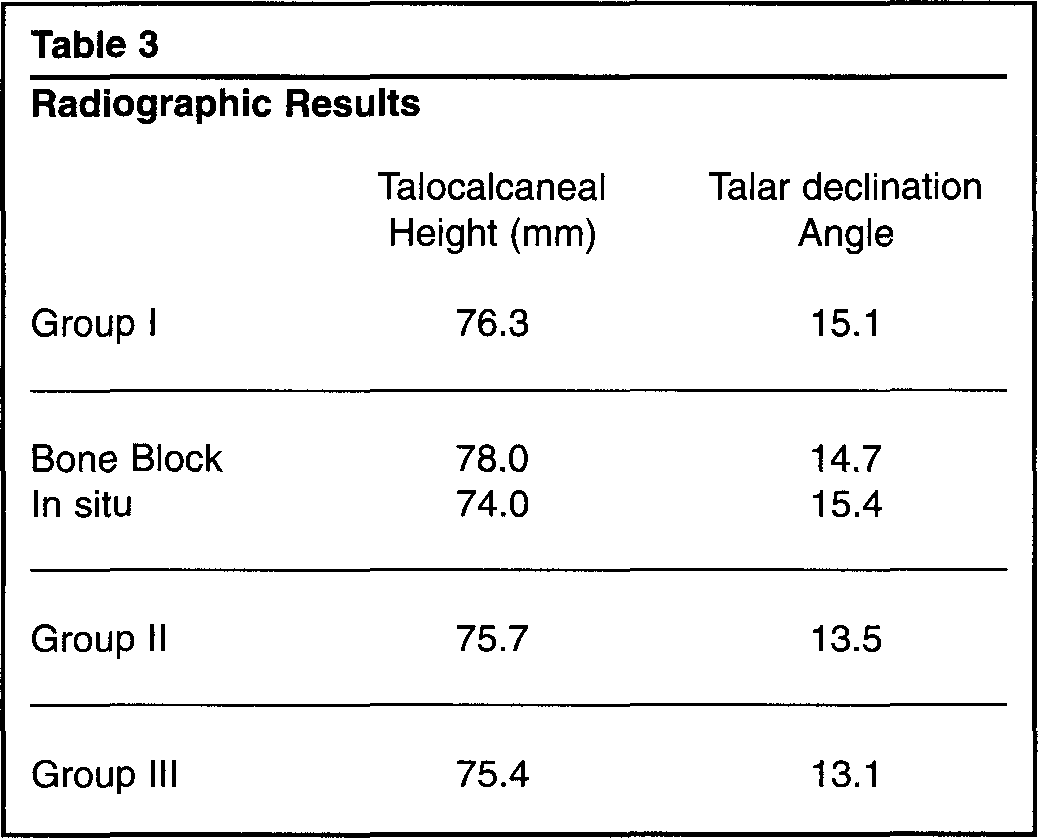
Radiographic Results
Radiographic Results
There were no gross changes in alignment following intial correction for any of the 86 fusions evaluated. The mean values for talocalcaneal height and talar declination angle are listed for each group (Table 3). Differences between groups were not statistically significant. The average postoperative talar declination angle for all 86 fusions was 14.6 degrees(range, 5 degrees to 28 degrees). Postoperative talar declination angles ranged from 5 degrees to 10 degrees in 15 fusions, from 11 to 15 degrees in 26 fusions, from 16 to 20 degrees in 41 fusions, and 21 to 28 degrees in 4 fusions. No correlation could be found between talar declination angle and the AOFAS ankle — hindfoot score (r = −0.04).
Hospital Stay
Seventy eight of the fusions were performed as isolated unilateral procedures. In 53 fusions autogenous iliac crest graft was used and in 25 fusions no iliac crest graft was taken. Length of hospital stay for patients with iliac crest bone grafting procedures averaged 3.7 days (range, 1 to 8 days). For those 25 procedures in which local, allograft, or no graft was used the length of hospitalization averaged 2.6 days (range, 1 to 6 days). This difference was statistically significant (p < 0.001). Nine of 53 (17%) of patients undergoing a ICBG procedure were discharged within 48 hours. Eleven of 25 (44%) of patients not undergoing an ICBG procedure were discharged within 48 hours.
DISCUSSION
Subtalar arthrodesis may be required following calcaneal fractures for: (1) Deformity and subtalar arthritis associated with malunions (2) post traumatic arthritis following failed open reduction and internal fixation (3) Type IV fractures which cannot be adequately reduced.
Various treatments of calcaneal malunions are described in the literature. Romash 18 described a reconstructive osteotomy for severely malunited fractures. The osteotomy was carried out through the primary fracture line which allowed repositioning of the tuberosity into a more anatomic position. This was followed by subtalar arthrodesis. Good results were reported in 7 patients at 6 month follow up. The results from bone block arthrodesis to restore heel height and talar inclination 6 have been mixed. They have varied from malunions and 50% good results 17 to overall significant improvement in pain and function in 28 patients 2 . However, problems with nonunions and varus malunions have been reported. Because of these complications noted with distraction bone block arthrodesis this procedure was not advocated by Stephens and Sanders 23 except in cases of severe hindfoot shortening. Rather, in their series of calcaneal malunions, they advocated adequate lateral wall exostectomy, correction of heel varus, and the achievement of a solid subtalar fusion. Using these techniques they achieved good or excellent results in 23 of 26 malunions with minimal reported complications.
Distraction bone block fusion attempts to restore hindfoot alignment thru correction of talocalcaneal height and talar inclination. The need to fully correct these parameters is controversial. In a review of 19 in situ subtalar fusions performed for late sequelae of calcaneal fractures, no significant correlation between patient outcome and talar declination or talar height was found. 8 Distraction arthrodesis was recommended only if anterior ankle impingement was present. Similarly, we could not find a correlation between postoperative talar declination angle and AOFAS ankle-hindfoot score for the 86 fusions followed for at least 2 years. In our study bone block fusions were performed in cases of severe hindfoot shortening and loss of talar inclination. At final follow up all patients had talar declination angles of at least 5 degrees and none of these patients had clinical evidence of anterior ankle impingement. It is possible that with negative talar declination angles or severe hindfoot shortening ankle impingement may occur therefore requiring a bone block procedure.
In our study, several procedures were used to reconstruct calcaneal malunions. These included lateral calcaneal closing wedge osteotomies, bone blocks arthrodeses, and in situ fusions. Outcome based on the AOFAS ankle- hindfoot score was similar regardless of the type of procedure used. However, complications of malunion or nonunion occured in 4 of 26 (15%) bone block procedures versus 2 of 36 (5%) insitu fusions.
Direct comparison of our results with these other studies on malunions is difficult because of the different grading systems used. Previously, the senior authors had used a modification of the Maryland foot score in reporting on subtalar arthrodesis.22,23 In order to help increase consistency in reporting on foot and ankle problems we elected to use the AOFAS rating system for this study. AOFAS scores from four studies of subtalar arthrodesis after calcaneal fracture correlated closely with our results 1,2,5,7
Primary subtalar arthrodesis combined with stable internal fixation has been advocated for the treatment of severely comminuted fractures.4,20 A recent report showed good results following this treatment with 14 patients achieving an average AOFAS ankle-hindfoot score of 72.44. Eleven of 12 previously employed patients were able to return to work. We report a similar AOFAS ankle-hindfoot score of 75.4 for the 8 patients in our study. Six of 8 patients were able to return to work. The remaining 2, both construction workers out on worker's compensation, had not yet returned to work.
A recent study 25 looked at a group of subtalar fusions which were done after calcaneal fractures treated nonoperatively. This was compared with a group whose fractures had been treated with open reduction and internal fixation. Various scoring systems were used and with each system those patients initially treated with open reduction and internal fixation scored slightly better. Results, however, were not statistcally significant. In our study 16 fractures with anatomic or near anatomic reductions which still required subtalar fusion were compared to 62 calcaneal malunions. No difference was found based on the AOFAS ankle-hindfoot score.
Overall patient satisfaction was high with 69 of 80 patients (86%) with 2 year follow up being satisfied with their outcome. In spite of this level of satisfaction 15% of non worker's compensation patients and 38 % of worker's compensation patients were unable to return to work.
In our study, there were no nonunions in 7 attempted fusions using allograft alone, and only one nonunion occurred in the 24 fusions in which local graft, allograft, or a combination of the two was used. Overall there were only two nonunions in 83 fusion attempts in which supplemental bone graft was used. In 3 cases performed early in the study period joint surfaces were felt to be congruent enough that no bone graft was required. Of these 3 attempted fusions in which no bone graft was used one nonunion occurred. We now use supplemental bone graft for all subtalar fusions and we routinely use cancellous allograft in any situation in which local graft is either unavailable or insufficient.
Luber and Nunley 13 were able to document shorter hospital stays and lower hospital costs in patients undergoing hindfoot arthrodesis using local bone graft versus those undergoing similar procedures using ICBG. Similarly, we found that the average hospital stay for fusions not involving autogenus iliac crest graft was significantly shorter.
Based on our results subtalar arthrodesis is an equally effective procedure following calcaneal fractures regardless of the indication. Complete anatomic restoration of hindfoot, based on talar declination angle, is not necessary for a satisfactory outcome. Therefore, in the absence of anterior ankle impingment, in situ fusions are recommended versus more complicated distraction bone block fusions.
Supplemental bone graft is recommended when performing a subtalar fusion, however, autogenous iliac crest graft is not needed as union can be achieved using a variety of bone graft materials. The advantages of local graft or allograft include lack of donor site morbidity and decreased postoperative pain. Finally, in situ fusions performed with local graft or allograft, result in decreased length of hospital stay thereby reducing overall cost to the insurer.