
Abstract
Purpose: The purpose of this investigation was to evaluate the outcome of tibiocalcaneal arthrodesis using an adolescent condylar blade plate for severe ankle and hindfoot deformities. Materials and Methods: We retrospectively reviewed the records of patients managed at our institutions between 1989 and 1996 whose tibiocalcaneal arthrodeses were performed with adolescent condylar blade plates and allograft bone. In these 30 patients (14 men, 16 women; average age, 53 years), the etiologies of the nonbraceable deformity included: diabetic neuroarthropathy with talar fragmentation and resorption (26), inflammatory arthritis (3), and posttraumatic avascular necrosis of the talus with collapse (1). Due to the severity of the deformity in 28 of these patients, the alternative treatment would have been amputation. Thirteen patients had undergone previous surgeries, eight had documented osteomyelitis, and 13 had ulcers ranging from 2 to 27 mm. At surgery, the remnants of the talus were removed. Morcellized bone graft mixed with tobramycin/vancomycin powder was inserted into the arthrodesis site and then fixed with a rigid plate. Intravenous antibiotics, followed by oral antibiotics, were given until wound healing and suture removal. Follow-up averaged 48 months (19 to 112 months). Results: Tibiocalcaneal fusion was achieved in 28/30 patients at an average of 16 weeks (12 to 18 weeks). Complications occurred in seven patients: two developed stress fractures of the tibia at the proximal end of the blade plate, three had superficial cellulitis that resolved with antibiotic therapy, and two had nonunions. Conclusion: Tibiocalcaneal arthrodesis using an adolescent condylar blade plate and allograft bone can be a successful procedure in the patient with severe neuropathic ankle deformity and can achieve a stable plantigrade foot for limited community ambulation with relatively few complications.
INTRODUCTION
Severe ankle and hindfoot deformities, which are often secondary to neuropathy or to inflammatory arthritis, are frequently associated with fragmentation or resorption of the talus. Weightbearing results in abnormal stresses on the hindfoot and ankle, which may lead to ulcer formation and osteomyelitis. The aim of treatment is to stabilize or correct the deformity either by bracing or by reconstructive surgery to prevent ulcer formation.
Although most hindfoot and ankle deformities with or without associated neuropathy may be treated with a brace, efforts to treat severe unstable or unbraceable deformities with special shoes, ankle/foot orthoses (AFOs), or braces are frequently unsuccessful. A below-the-knee amputation may then be required. Current surgical options to stabilize the limb include pantalar, tibiotalocalcaneal, or tibiocalcaneal (TC) arthrodesis. Pantalar or tibiotalocalcaneal arthrodesis may not be possible in the presence of associated talar avascular necrosis, fragmentation, or resorption. There are four reports 1,11,14,15 of TC arthrodesis in the literature. Three studies reported fixation with either screws 11,14 or Steinmann pins 15 ; only one of these studies included patients with neuroarthropathy. 14 The fourth report 1 included preliminary findings of seven patients with diabetic neuroarthropathy, who are also included in the current study.
The purpose of the current study was to evaluate the outcome of TC arthrodesis using an adolescent condylar blade plate and bone graft for severe ankle and hindfoot deformities.
MATERIALS AND METHODS
Patient Population
Between 1989 and 1996, two of the authors performed 30 unilateral TC arthrodeses on 14 male and 16 female patients (average age, 58 years; range, 26–78 years) (Table 1). The preliminary results of treatment of seven of the 30 patients were previously reported. 1
• Patient Data*
The indications for surgery were severe ankle and hindfoot deformity due to diabetic neuroarthropathy with talar fragmentation and resorption (26), inflammatory arthritis (three) or posttraumatic avascular necrosis of the talus with collapse (one). Surgery was performed in an effort to improve both limb alignment and the potential rate of healing. In all these cases, there was fragmentation with partial or total resorption of the talar body, causing either varus or valgus deformity of the hindfoot. For 28 of the 30 patients, the alternative to reconstructive surgery for this deformity would have been an amputation. These patients had either recurrent ulcers or osteomyelitis.
At the time, 13 patients had ulcers of the foot or ankle ranging from 2 to 27 mm. Osteomyelitis (four in the head of the talus, two in the fibula, and two in the medial malleolus) was documented in eight patients with concurrent technetium and indium-labeled white cell scans. 10 Two patients had received previous treatment for osteomyelitis of the fibula or medial malleolus; both cases had resolved.
Thirteen patients had undergone previous surgery: open reduction and internal fixation (ORIF) of ankle fractures (patients #1, 11, 17, 20, 25); ORIF and multiple fusion procedures (patients #4, 16); debridement of osteomyelitis (patients #3, 5, 8, 9, 19); and ankle fusion (patient #22).
Management
Initial Intervention. Treatment after presentation at our institution(s) included ORIF (patient #10) and revision ORIF for nonunion (patients #1 and 11). The other 27 patients were treated with protected ambulation using an AFO, cast, or boot to reduce inflammation and swelling and to control ulceration, if present. Ulcers were dressed and swelling was controlled with an Unna boot (Carapace, Inc., Tulsa, OK). Surgery was deferred until there was no evidence of clinically active infection and until swelling had decreased. If the limb was swollen, diuretic agents, bed rest with limb elevation, and a Unna bandage (Carapace, Inc) were used for 48 hours before surgery. In patients with documented osteomyelitis, the treatment had been initiated with culture-specific intravenous antibiotics, wound care, and limited ambulation. Although the infection was not eradicated in these patients, there was no drainage or surrounding erythema at the time of reconstructive surgery. The osteomyelitis was localized to the medial malleolus (in two), the distal fibula (in two), and the talar head (in four), and the infected bone was completely resected at surgery. The administration of intravenous and oral antibiotic therapy did not depend on the peroperative presence of ulcers or osteomyelitis (which would have been grossly eliminated by ostectomy at surgery).
Surgical Procedure. A curvilinear incision was made over the distal 10 cm of the fibula and was extended distally toward the sinus tarsi. Whenever possible, previous incisions were followed. A full-thickness skin flap was developed. In the patient with neuropathy, the sural and superficial peroneal nerves were cut to avoid excessive skin retraction and dissection.
The distal 10 cm of the fibula were resected after an oblique osteotomy with an oscillating saw. If not associated with ulcer or infection, the fibula was harvested for bone graft using an acetabular reamer or, after osteotomy, the fibula was morcellized in a bone mill, and the harvested graft was added to the allograft (Fig. 1). The remnant of the talus was excised. Specifically, the frag-merited body of the talus was always removed, although the head of the talus was protected and preserved provided it was vascularized and not involved with a medial dislocation of the talonavicular joint or infection.
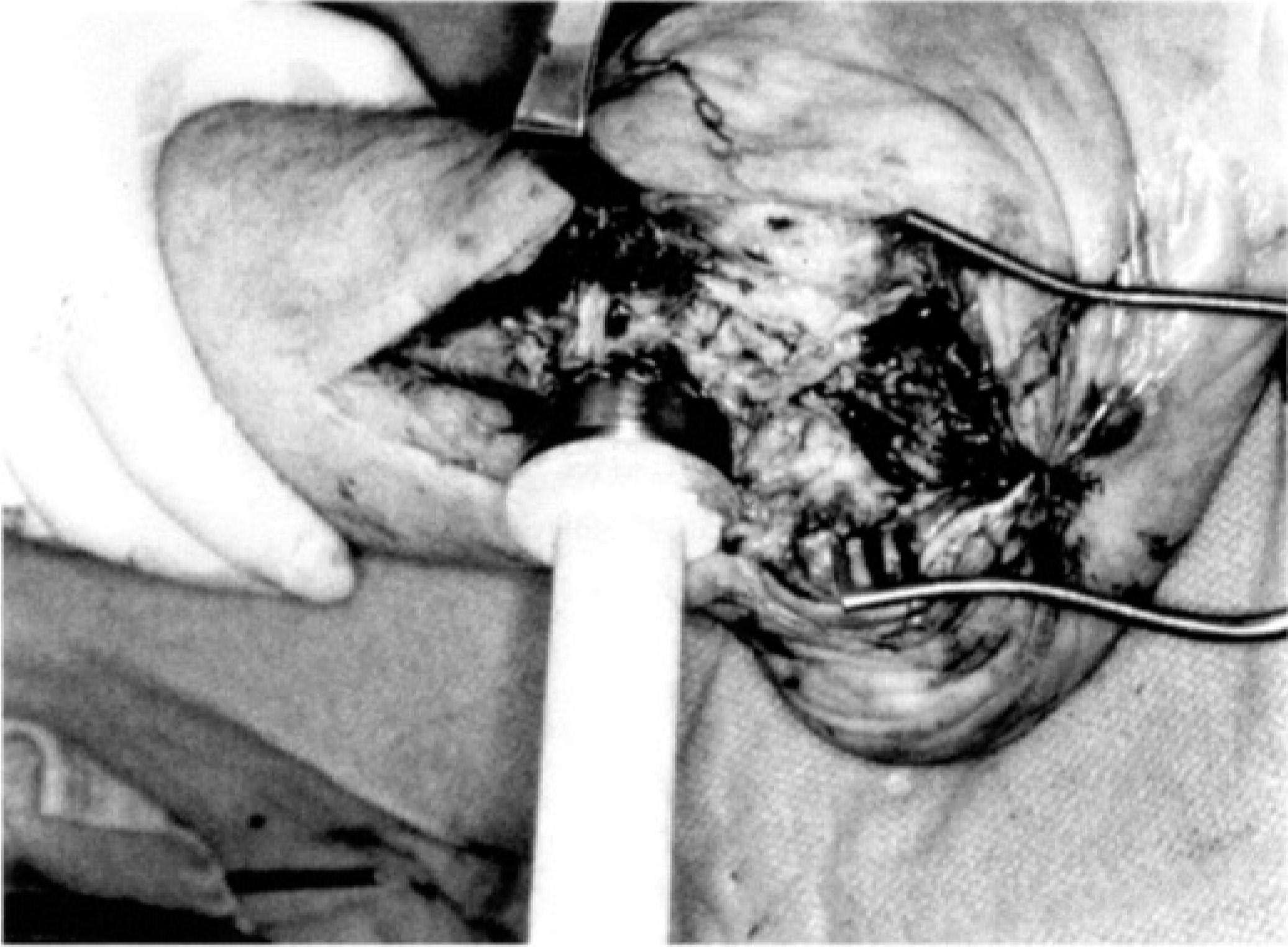
The acetabular reamer is used to harvest the distal fibula for autograft.
The articular surface of the distal tibia was prepared by making a flat cut with an oscillating saw, and a flexible chisel was used to debride the articular cartilage on the dorsal surface of the calcaneus. Great care was then taken to establish precise alignment of the foot under the leg. The aim was to obtain a plantigrade foot with the foot at 90° with respect to the leg, the hindfoot in 5° of valgus, and slight (5 to 10°) external rotation of the foot (Fig. 2). After the deformity was reduced, it was stabilized initially with two 1.6-mm guidepins. One guidewire was inserted through the heel posteriorly into the distal tibial metaphysis anteriorly. The second guidewire was inserted posteriorly through the distal tibial metaphysis into the talar head (if present) or the navicular.
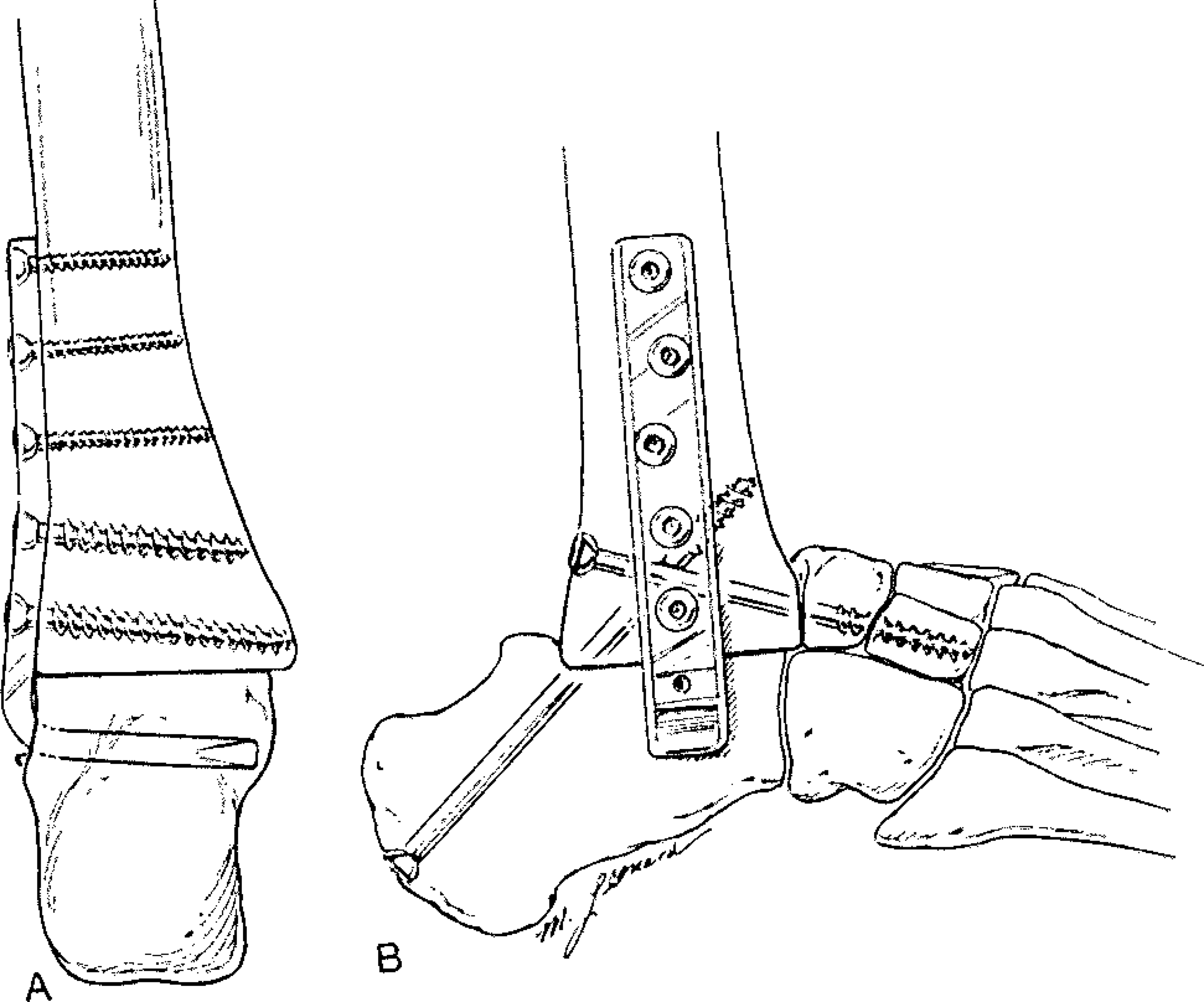
The position and application of the blade plate. [By permission from: Myerson MS: Diabetic neuroarthropathy. In Myerson MS (ed): Foot and Ankle Disorders; pp 439-465. Philadelphia, WB Saunders Co, 2000.]
The blade plate was then placed on the lateral calcaneal subchondral bone in the region of the posterior facet. Care was taken to position the hindfoot in neutral because there is a tendency for the calcaneus to displace into slight valgus as compression is applied to the plate proximally (Fig. 3). We typically applied compression to the plate through the two most proximal screw holes. If added stability was required, a fully threaded 6.5-mm cannulated cancellous screw was placed over a guidepin from the calcaneus posteriorly to the anterior distal tibia proximally.

After the foot is positioned with cannulated guidepins, the blade plate is applied.
Allograft or autograft bone, or a combination thereof, was used; the choice was determined by the amount of bone harvested from the fibula and the size of the defect to be filled. In the current study, 18 patients had femoral head allograft, six had fibula autograft, and six had both autograft and allograft. The bone graft was then mixed with 400 mg of tobramycin and 500 mg of vancomycin powder. The antibiotic bone graft mixture was firmly packed between the bone surfaces anteriorly, in addition to the posterior aspect of the tibia and calcaneus, to facilitate an extraarticular as well as the intraarticular arthrodesis. The wound was closed in layers using 2-0 absorbable sutures, and 3-0 nylon sutures were used for the skin. If tension was present on the skin edges during closure, it might have been due to the change in shape of the hindfoot or the added subcutaneous bulk of the plate. In the current study, four patients underwent excision of the peroneal tendons to provide sufficient room for wound closure without tension.
Postoperative Care. A bulky sterile dressing and well-padded short-leg posterior plaster splint was applied. Intravenous antibiotic therapy (3 to 5 days) followed by oral antibiotic therapy was administered until the wound was healed, at which point (generally between 2 and 4 weeks) the sutures were removed. The limb was immobilized in a below-the-knee nonweightbearing cast for 3 months, followed by a weightbearing below-the-knee cast for an additional 2 to 3 months. Cast changes, clinical evaluation, and radiographic examination were performed every 4 weeks. The patient was then allowed to walk as tolerated wearing an AFO or a shoe with a cushioned heel and rocker sole.
Fusion was determined both clinically (no increase in warmth, improvement in swelling, and stable to stress) and radiographically (trabeculation across arthrodesis site and no lucency around hardware).
Evaluation by range of motion and American Orthopaedic Foot and Ankle Surgery score was not performed for our group of patients because the only goal was to obtain a braceable foot for community ambulation.
RESULTS
All patients presented for a follow-up examination and radiographic evaluation at a mean of 48 months (range, 19–112 months) after surgery (Table 1). Fusion was achieved in 28/30 patients at an average of 16 weeks (range, 12–18 weeks) (Fig. 4). Nonunion occurred in two patients (patients #5 and 8). In one (patient #5), who weighed 160 kg, compliance with respect to weightbearing was a problem, and the plate broke at 4 months. The hindfoot remained stable, no subsequent problems with the hardware occurred, and he now uses a clam shell AFO boot for ambulation. At 38 months after surgery, the foot is stable. The second patient (patient #8) developed loosening of the plate and a broken cannulated screw at 3 months. The hardware was removed at 4 months due to pressure on the skin. He currently ambulates in a clam shell AFO boot, and at 22 months after surgery there is no skin ulceration although gross motion is present in the hindfoot. Preoperatively, 13 patients in this series had ulcers, all of which healed after correction of the deformity. Two patients developed superficial ulceration of the plantar lateral aspect of the midfoot at 24 and 32 months after surgery, which resolved with 4 weeks of treatment in a total contact cast and no subsequent recurrent ulceration.
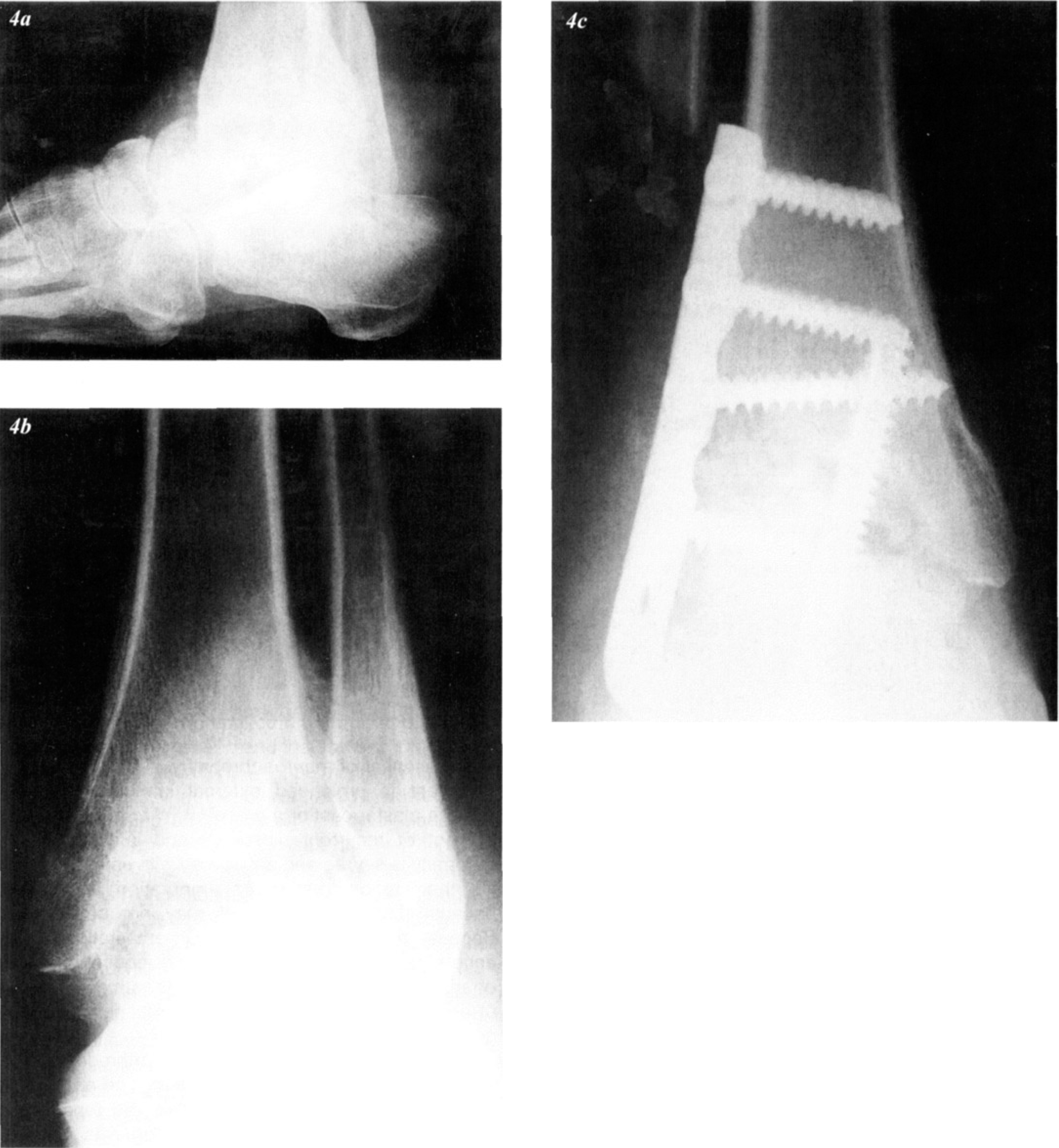
This patient was treated for recurrent ulceration over the medial malleolus and, despite a molded clam shell boot, instability and ulceration persisted. Note the collapse of the talus on the lateral (a) and anteroposterior (b) views of the ankle. At 39 months after surgery, the foot is stable and fusion is present. (c), anteroposterior view. (d), lateral view. (e), mortise view.
There were no deep infections. Complications included three cases of superficial cellulitis that resolved with oral antibiotic treatment and two tibial stress fractures, each occurring at the proximal end of the blade plate. The fractures, which occurred at 9 and 14 months after surgery, healed with treatment in a nonweightbearing above-the-knee cast for 6 weeks, followed by weightbearing in a below-the-knee cast for 6 to 8 weeks. The etiology of these fractures was likely to have been the stress concentration at the proximal screw or plate, possibly aggravated by the lack of use of the AFO in one patient.
All patients were braced in a polypropylene AFO worn in a shoe with a slight rocker-bottom and were able to ambulate in the community without ancillary aid. Bracing and shoe modifications were made easier because the treated leg was 2.5 to 3.0 cm shorter than the contralateral leg.
DISCUSSION
The management of patients with severe deformities of the ankle and hindfoot is challenging, particularly in the presence of neuroarthropathy. The mainstay of treatment is prolonged external immobilization with either a plaster cast or a brace 3,5,7,9,13,16 to prevent development of recurrent ulceration and infection. If the deformity is severe and associated with severe instability, then reconstruction or amputation is required because brace management may not be feasible. Because most patients undergoing amputation experience some limitation in function and require increased energy to walk 6 and because patients with diabetes are at risk for contralateral amputation, reconstructive surgery may be the preferred option.
Reckling 15 reported on primary TC arthrodeses after displaced talus fractures in eight feet. The arthrodesis was fixed with three Steinmann pins. He reported no wound problems and that solid fusion was obtained within 17 weeks. Mann and Chou 11 reported on nine TC arthrodeses: seven for revision arthrodesis (three failed total ankle arthroplasties, three nonunion ankle arthrodeses, one nonunion pantalar arthrodesis), one for posttraumatic talar avascular necrosis, and one for rheumatoid arthritis. There were no cases of neuroarthropathy. Fixation was performed with 6.5- or 7-mm cannulated cancellous screws or multiple staples. Autogenous corticocancellous bone graft was used. Fusion was achieved at an average of 22 weeks (range, 12–40 weeks). Complications included local infections (two), malunion (two), wound slough (one), prominent fibula (one), and loss of fixation requiring supplemental external fixation (two). Papa et al 14 reported on 29 patients with chronic diabetic neuroarthropathy who were treated with open reduction and arthrodesis for unbraceable hindfoot deformity. Of the 29, there were 11 patients for whom a TC arthrodesis was performed using cannulated cancellous screws, supplemented by allograft and/or autograft bone. There were seven nonunions; the remaining four patients healed at an average of 21 weeks (range, 16–24 weeks). Alvarez et al 1 reported on seven patients treated with TC fusion (included in the current series).
Intramedullary devices used for tibiotalocalcaneal arthrodesis have had satisfactory results. 8 A biomechanical study by Berend et al 2 compared intramedullary nail fixation with lag screw fixation and showed that the intramedullary device is a stiffer construct than crossed lag screws, which might help increase fusion rate. However, its use has not been reported for TC arthrodesis. An intramedullary device would not provide rigid fixation for TC arthrodesis because the calcaneal fragment is relatively small and would allow insertion of only one interlocking screw.
Other studies in the literature have found that successful fusion in the presence of neuroarthropathy has been difficult to achieve 16,17 and that rates of infection (13 to 33% 16,17 ), wound breakdown, and malunion have been relatively high. 16,17 In the current study, however, TC arthrodesis using an adolescent condylar blade plate resulted in fusion in 93% of cases and few complications, despite the presence of osteopenia in all patients treated. This high fusion rate was due to the strong purchase of the blade in the calcaneal subchondral bone in the region of the posterior facet. In the current series, fusion was achieved at an average of 15 weeks. This is despite the inclusion in the current series of many patients with neuroarthropathy (26/30) and the exclusion of such patients from the other two reported series.
Also in contrast to the previously reported incidence of deep infection after fusion in neuroarthropathic joints, the current series had no deep infections despite the presence of ulcers in 13 patients. The use of antibiotic bone graft mixture may have reduced the risk of deep infection. Morcellized cancellous bone is a suitable vehicle for depot administration of antibiotics. 12 In vitro elution studies have shown that mobilization of tobramycin from morcellized cancellous bone depends on the exposed surface area and antibiotic concentration. 12
The TC procedure in the current study used the principles of Drennan et al 4 for arthrodesis in neuroarthropathic joints: 1) careful removal of all cartilage and debris; 2) thorough removal of sclerotic bone down to bleeding, well-vascularized bone; 3) meticulous fashioning of congruent bone surfaces for apposition; 4) firm fixation of bone; and 5) complete debridement of all synovial and scar tissue.
CONCLUSION
TC arthrodesis using a condylar blade plate is a demanding technique but has resulted in more rapid fusion and fewer adverse events, such as deep infection, than previously described. TC arthrodesis provided salvage for severe hindfoot/ankle deformities, resulting in a plantigrade foot for community ambulation.