
Abstract
The aim of this study is to search the effects of tibial torsion on flexible flatfoot. For this purpose, 20 children with flexible flatfoot and external tibial torsion were determined as a study group. The control group which consisted of 10 children with flexible flatfoot without rotational problems was included in the study. Plantar flexion angle of talus, talo-1. metatarsal angle and dorsoplantar talocalcaneal angle were measured on standing foot radiographs. Tibial torsion was measured by computed tomography. Plantar flexion angle of talus and dorsoplantar talocalcaneal angle were found significantly lower in the study group (p<0.005 and p<0.005 respectively), although talo-1. metatarsal angle was not significantly different between the groups (p=.2917). Naviculo-cuneiform sag was prominent in all cases of study group. In conclusion, abnormal external tibial torsion may affect the foot deformity and this can change the benign nature of the flexible flatfoot.
INTRODUCTION
In the past, rotational problems in the transverse plane have often been ignored because they are difficult to assess. 5 These problems are likely to attract increasing attention because accurate assessment is now possible using computerized transverse plane tomography and optical and electronic techniques of motion analysis. 5 Rotational problems in the transverse plane of lower extremity are associated with many clinical problems, ranging from in-toeing gait in children to degeneration of adjacent joints. On the other hand, the interactions of the horizontal plane and the deformities in the other planes are not known. This study is an effort to search the effects of tibial torsion on flexible flatfoot especially in the horizontal and sagittal planes.
MATERIALS AND METHODS
The study group (Group 1) consisted of 20 consecutive children who were admitted to the outpatient department between 1993 and 1996 with flexible flatfoot and external tibial torsion, which was assessed by the measurement of angle of the transmalleolar axis on the first clinical examination 6 . The patients who had congenital anomalies, neurologic disorders or treated lower extremity problems previously were excluded from the study. 11 patients were male, 9 were female. Mean age was 49.1 months, range 30 to 71 months. After the study group was completed, ten consecutive children with flexible flatfoot but without external tibial torsion created a control group (Group 2). Distribution of patients for age and gender is displayed in Table 1.
Age and the gender of the patients.
Distribution of patients for gender is almost same in both groups.
A thorough musculoskeletal and neurologic examination was carried out for each case, with special reference to range of motion of the joints, muscle power and lower extremity lengths. Intercondylar and intermalleo-lar distances were also recorded to evaluate frontal plane alignment.
Medial arch depression was assessed by the criteria of Tachdjian, as follows: The deformity is divided clinically into three categories; first degree in which on weight bearing the longitudinal arch is depressed but still visible; second degree in which the longitudinal arch is not visible in stance and third degree in which the longitudinal arch is absent and the medial border of the foot is convex with the head of the talus presenting on the plantar aspect of the foot. 8 Foot progression angles for each child were also recorded.
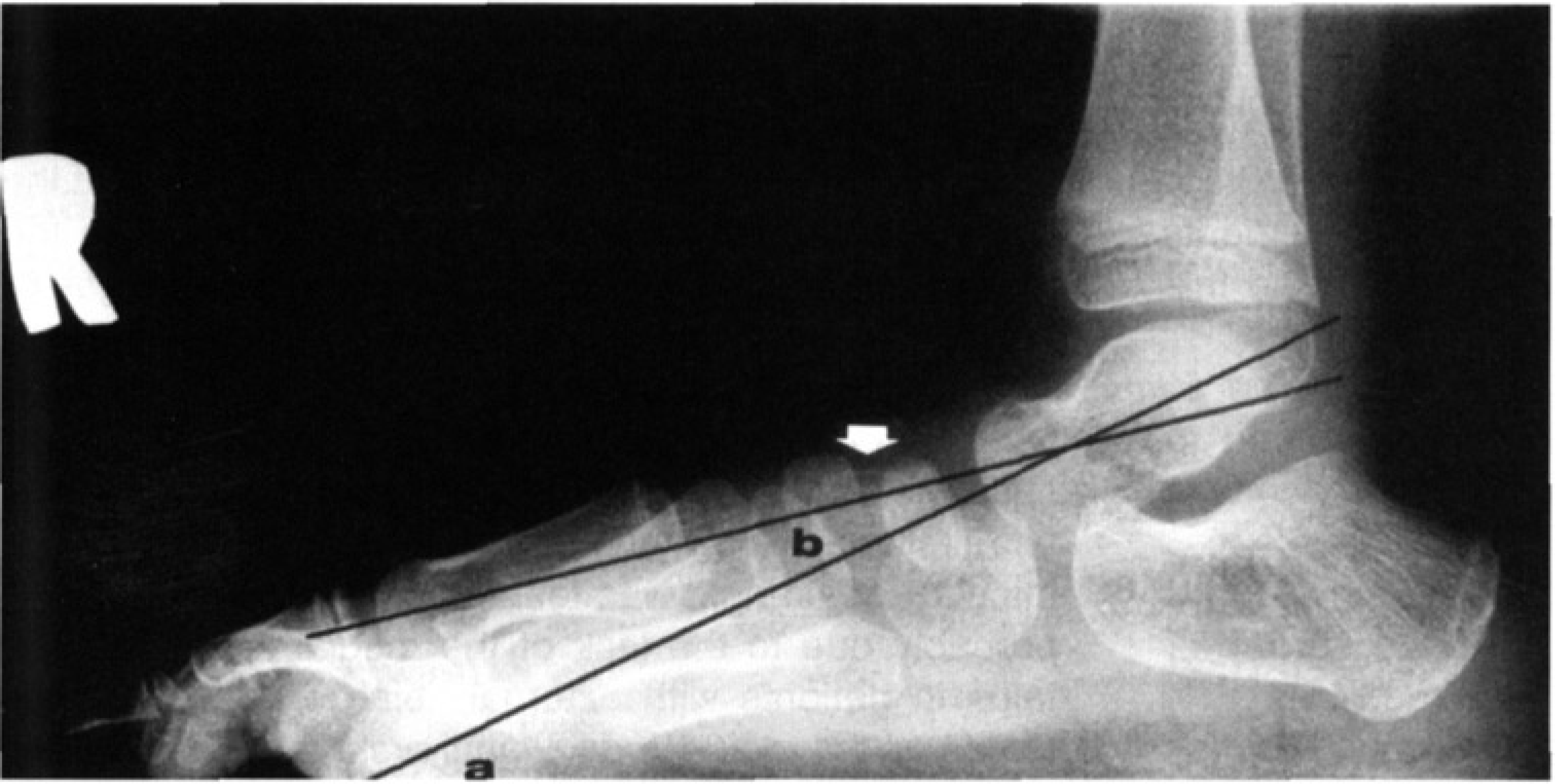
The measurements of plantarflexion angle of talus (a) talo-1. metatarsal angle (b) on lateral standing radiograph. Note that the depression of the medial langitudinal arch is prominent at the naviculocuneifom joint (arrow).
Dorsoplantar and lateral standing foot radiographs were taken for each case to assess the bony components of the medial longitudinal arch. Dorsoplantar talocalcaneal angle, plantar flexion angle of the talus and talo-first metatarsal angles were also recorded. (Fig. 1)
Tibial torsion was measured by the technique of Yagi and Sasaki with computed tomography. 10 Subjects were placed in a supine position and stabilized with hip and knee joints in extension and the foot in the neutral position. The patients with poor cooperation were evaluated under sedation. The limb was scanned from proximal tibial condyle to the ankle joint. The axes for which measurements were taken were the transverse axis of the proximal tibial condyle and the trans-malleolar axis. The angle between these two axes is the degree of torsion of the tibia. On the average tibial torsion has been shown to range from +2° to +4° at birth and from +10° to +20° in adults. 6 In our study, the measurements over +15°, which is the mean value of adult tibial torsion, were considered abnormal external tibial torsion 7 . (Fig. 2)
All radiographic analyses were performed by the same author (O.A.) and the results were assessed by Mann-Whitney U test.
RESULTS
There was no difference between the groups, as far as age and gender distribution. There was no leg length discrepancy or muscle weakness nor ankle or subtalar motion restriction in any child. Valgus of the heel in the stance phase was present in both groups. In group 1, medial arch depression was first degree in 6 patients (30%), second degree in 11 patients (55%) and third degree in 3 patients (15%). In group 2, first degree medial arch depression was found in 4 patients (40%), second degree in 5 patients (50%), and third degree in 1 patient (10%). Heel cord tightness was not detected in the two groups. Both groups showed physiological genu valgum in the frontal plane alignment. Intermalleolar distance was 3.0 cm ±0.8 (range 2.0 to 4.5) in group 1 and 3.4 cm ±0.9 (range 2.0 to 4.0) in group 2. The differences between two groups was not statistically significant (p=.3425).
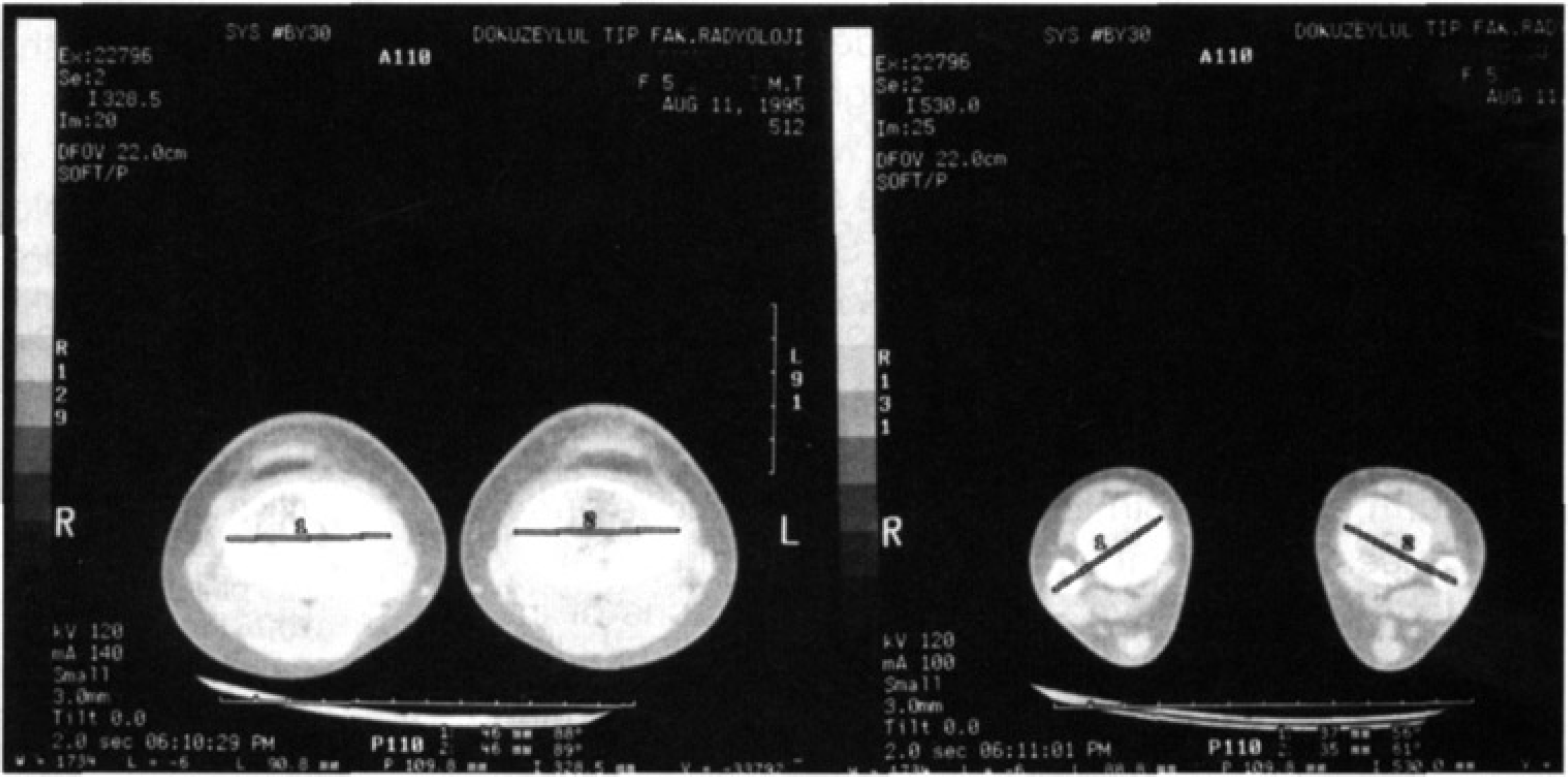
Measurement of tibial torsion angle with computed tomography. External tibial torsion was calculated 32 degrees and 30 degrees on the right and legt tibia, respectively. On the left is proximal tibia just inferior to the joint surface, and on the right the anatomical level is transmalleolar.
In group 1, all cases showed out-toeing gait, whereas all but one case in group 2 had neutral foot progression angle. Only one case had in-toeing gait.
The mean dorsoplantar talocalcaneal angle was 30.8°±3.1 (range 26 to 38) and 40.8°±3.9 (range 34 to 48) respectively in group 1 and 2. The measurements were found different between the two groups and this difference was statistically significant (p<0.005).
Plantarflexion angle of the talus was found lower in group 1 (25.9°±1.6 range 22 to 29) as compared to group 2 (31.8°±1.9 range 29 to 36). The difference was statistically significant. (p<0.005)
Although talo-1 metatarsal angle was not significantly different (p=.2917) between the groups, group 1 showed wider range (13°±5 range 6 to 25 and 13.9°±2.4 range 10 to 18). In addition, while talonavicular sag was detected in all cases of group 2, naviculocuneiform sag was prominent in group 1.
Mean values of torsion are different in both groups because of selection of patients were made according to tibial torsion angle. Tibial torsion angles in group 1 and 2 were 29.4°±6.7 (range 19 to 42) and 9.8°±2.7 (range 4 to 14) respectively.
DISCUSSION
The subtalar joint is a complex joint which behaves like an oblique hinge, and its best defined axis has an oblique orientation averaging 42 degrees of upward tilt from posterolateral to anterolateral with 23 degrees of medial angulation. The joint acts like a hinge to transfer the rotation at the leg to the feet. 1,2,3 So the internal and external rotation of the leg produces foot pronation and supination respectively. 3
Depression of the medial longitudinal arch in flexible flatfoot is localized at the talonavicular joint, naviculocuneiform joint, or both joints. 8 The pathologic features and causes of different sag locations are not known.
Vaderwilde et.al. have studied on radiographs of the foot in normal infants and children. Radiographs were made of each case at three different positions during weight bearing. Their measurements showed that the mean values are changing with age and the ranges of normal values are wide. They proposed that their data provide a standard assessment of initial deformity in patients with different foot deformities. 9 In our study, the values are compared between control and study groups. So the patients are not classified as normal or abnormal according to radiographic measurements.
During the normal gait cycle, approximately 60% of the time is spent in stance and 40% in swing. 4 After floor contact by the heel in stance phase, the foot quickly drops into 10 degrees of plantarflexion. While this sagittal motion occurs, there is also transverse rotation at the subtalar joint placing the heel at contact lateral to the midline axis of the ankle joint. This creates a valgus of the heel and the talus falls into internal rotation. 4
Although we found significant differences in plantar flexion angle of the talus between the groups (p<0.005), this difference was not significant with respect to the talo-first metatarsal angle(p=.2917). Also dorsoplantar talocalcaneal angle was found lower in group 1. This is probably due to the lack of the medial rotation of the talus in patients with external tibial torsion. Then the forces on the medial longitudinal arch, act from the naviculocuneiform joint rather than talonavicular joint, so the depression becomes more prominent distal to the navicular, if the ligamentous support is not sufficient. This results in depression of the horizontal angle of the first metatarsal. Conversely, medial rotation of the talus is more prominent in cases with neutral tibial torsion, and depression of the medial arch is localized on the talonavicular joint.
As a result, it can be said that, if a child with flexible flatfoot has excessive external tibial torsion, the torsional problem may affect the foot deformity and convert the benign nature of the flexible flatfoot to a more complex problem.