
Abstract
Hindfoot and forefoot arthrodeses procedures are commonly performed using autogenous bone graft harvested from the distal tibia. A new technique is described for obtaining cancellous bone graft from the distal tibia using a bone graft harvesting system specifically designed to obtain morsellized material through a small incision site. The use of this device in association with low dose fluoroscopy and backfilling of the defect with osteoconductive synthetic graft material is also discussed.
INTRODUCTION
Arthrodeses are commonly performed procedures in the treatment of degenerative and post traumatic problems of the foot and ankle. While autogenous iliac crest graft is the traditional source of material for these procedures, there are some studies that have indicated that the harvesting of this graft is not without morbidity 1,2 . These complications have included donor site pain, bleeding, infection, heterotopic bone formation, hernia, nerve injury and fractures. Because of these complications orthopaedic foot and ankle surgeons have preferred to harvest bone from the distal tibial region due to its convenience and perceived lower morbidity rate. 3,4 These authors among others have indicated the distal tibial bone graft can be successfully used in arthrodesis in the foot and ankle. While the distal medial tibia has been shown to be a good bone graft source, stress fracture through a rectangular or square cortical window is a potential complication whereas a circular window has been shown to be the least likely to result in stress fracture 5 . It is most important in harvesting bone from the distal tibia not to encroach too closely the tibial plafond and it would appear prudent, if feasible, to backfill the cavity created by harvesting with some form of osteo-conductive material.
The author has used a bone graft system developed by Acumed (Beaverton, Oregon) for the purposes of obtaining graft with intra-operative low dose fluoroscopy combined with backfilling of the donor defect with Osteoset bone void filler (Wright Medical Technology, Arlington, TN) for this. The Acumed system consists of a selection of cutting hollow tubes in a range of sizes (6,8,10 and 12mm) which morcellize bone graft material from appropriate donor areas through a small incision site with the potential for minimal morbidity.
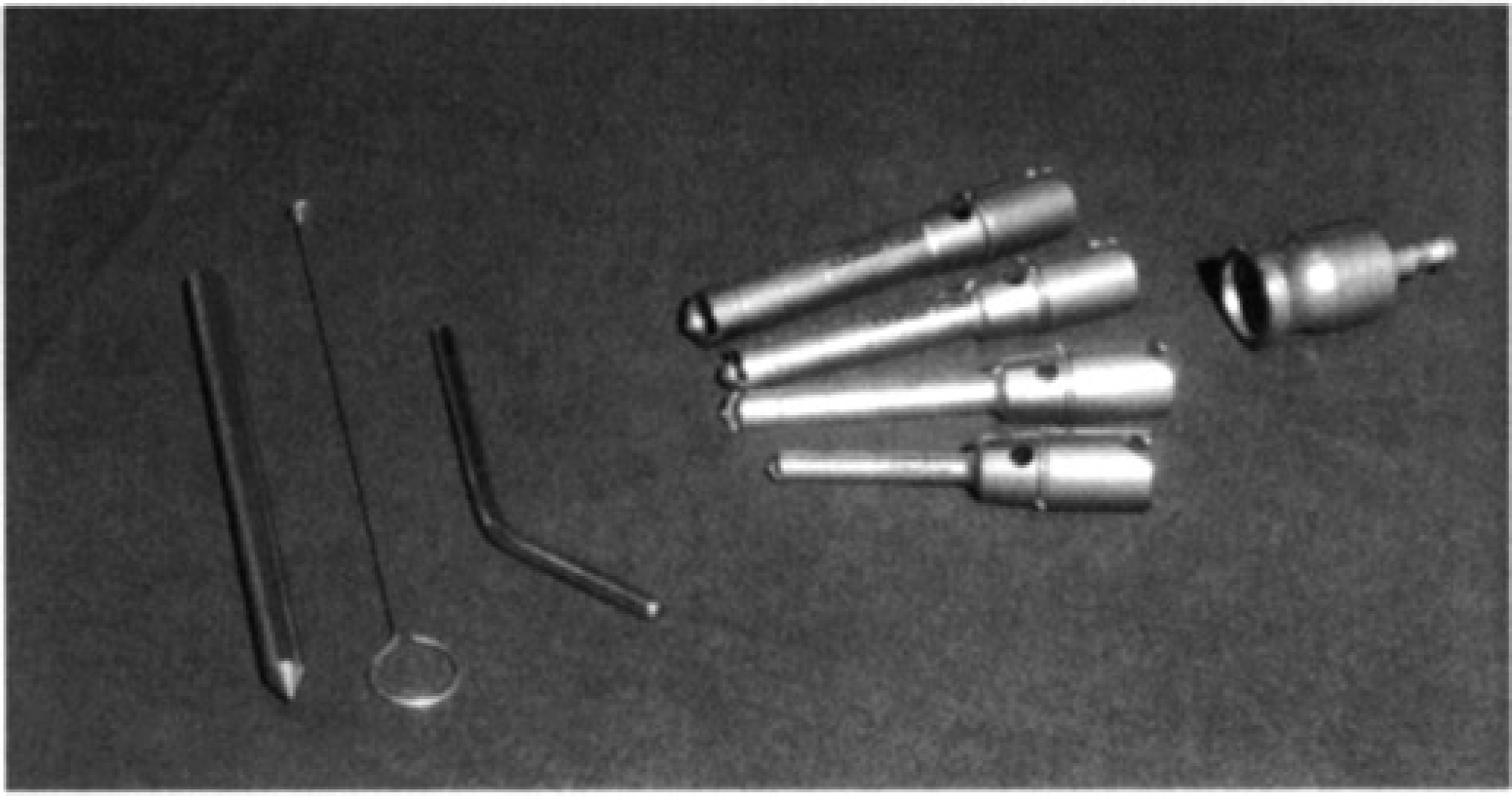
Photo of the Acumed device showing the instrumentation
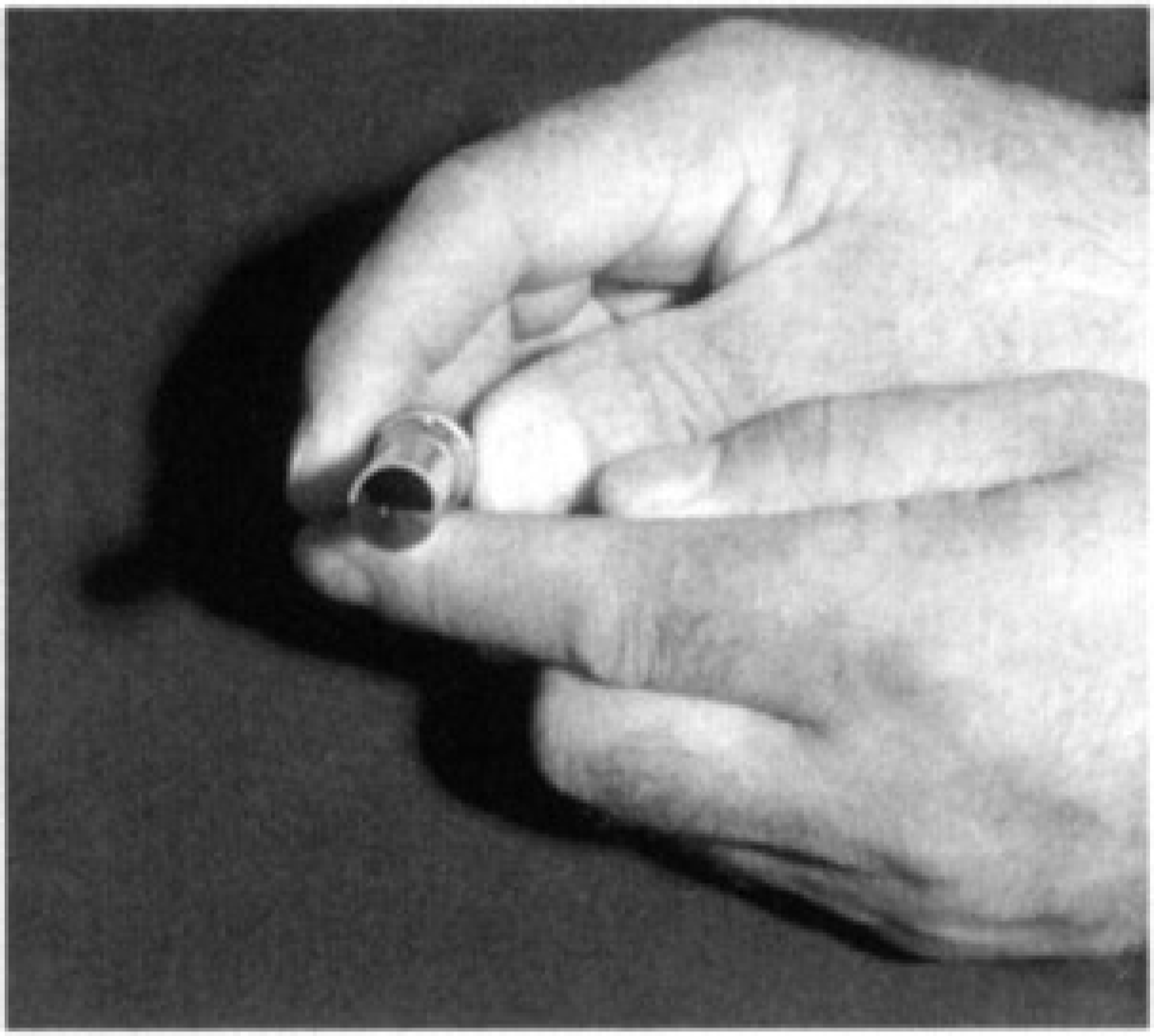
Photo showing the end-cutitn flute of the device. This allows the device. This allows the obtaining of morsellized graft material. The volume obtained depends partly on the diameter of the device.
SURGICAL PROCEDURE
The tibial bone graft site is identified using low dose fluoroscopy at an area just over the medial aspect of the distal tibia, proximal to the flare of the meta-physis. A one to two cm incision is centered over the marked area and an incision is carried down to the periosteum. The saphenous vein and nerve are identified and protected. The periosteum is incised longitudinally and elevated. Using a sharp pointed awl and mallet the Acumed bone graft system starting hole is made over the center of the medial tibia at the desired entrance point. This hole prevents the trephine from walking off the bone. An appropriate sized trephine is attached to a Hudson adapter rotating clockwise and the trephine is then drilled into the bone.
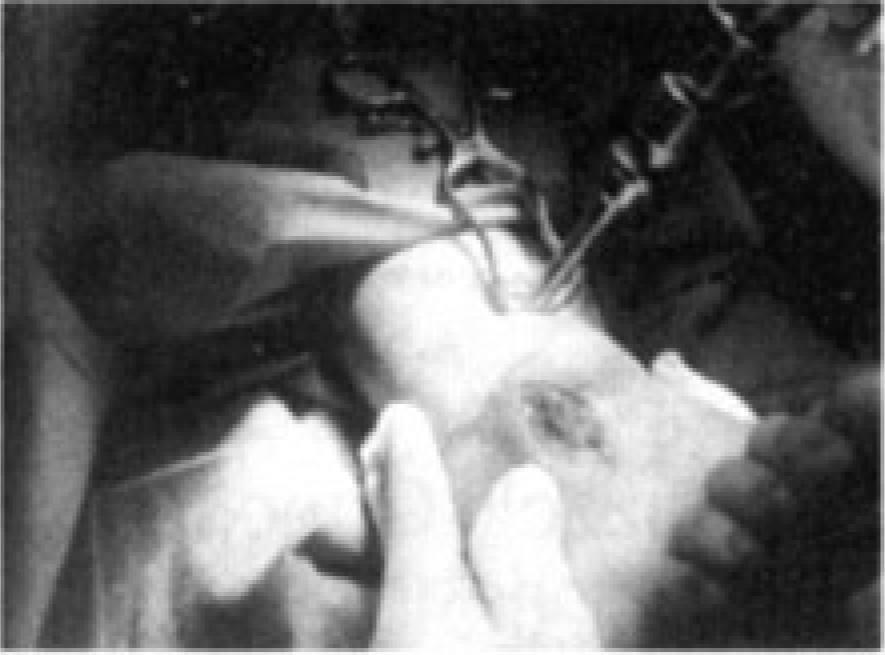
Clinical photo of the device in use of the distal tibia.
A 12mm or 10mm core drill is used. Progress is monitored using low dose fluoroscopy. Care is made not to penetrate the opposite cortex or to angle the drill distally towards the tibial plafond. Following each pass the drill is disengaged and bone graft material is extracted using the appropriate wire extractor. Passes in multiple directions can be made. With the 12mm core drill inserted 2 or 3 cms, approximately 2 1/2 ccs of bone material can be obtained with each pass. A small curette can be inserted through the circular hole to obtain extra graft material. The residual void is then backfilled using small Osteoset beads.
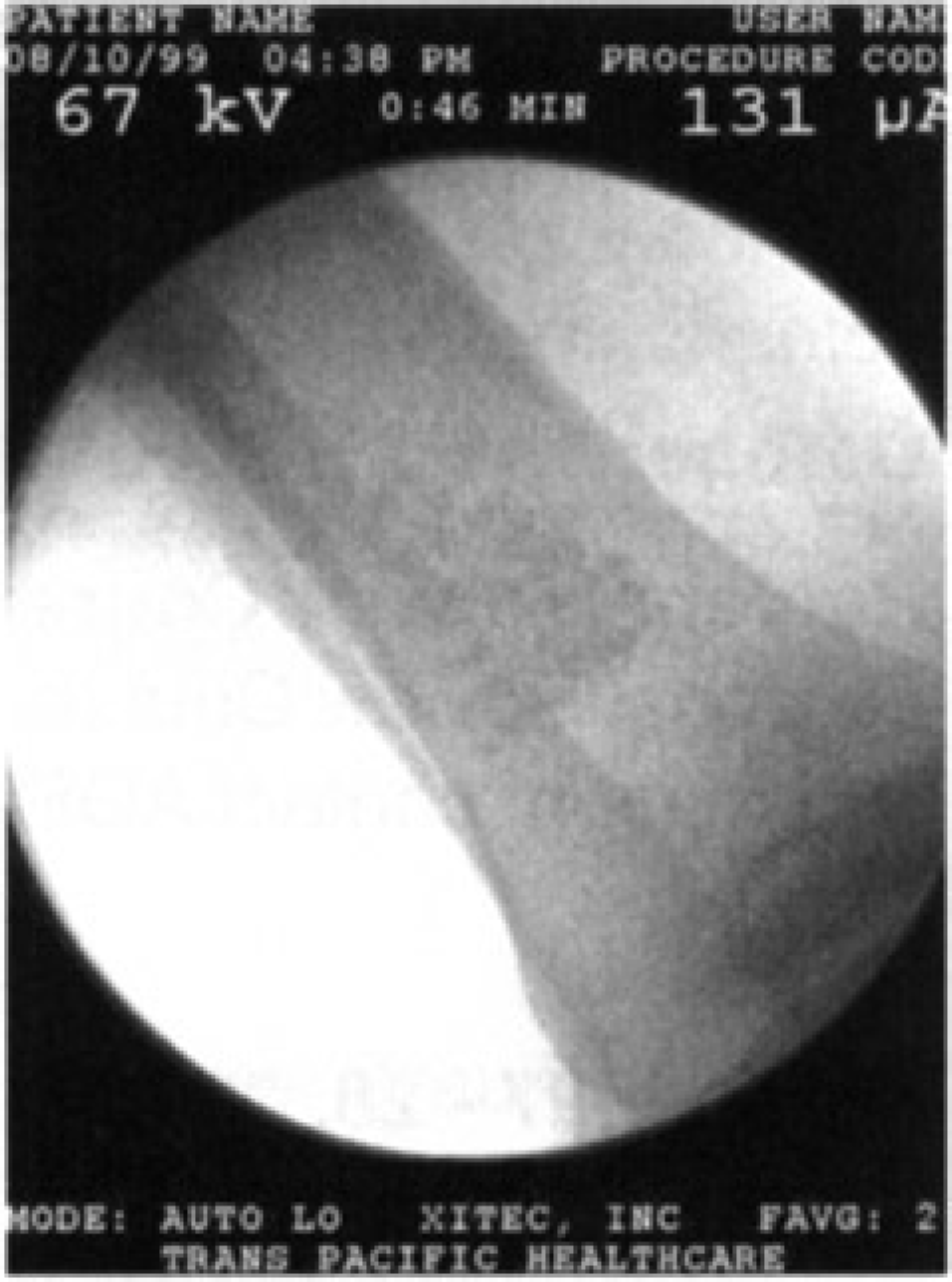
Intra-operative film showing the backfilled defect giving an idea of the volume of material, which can be obtained with this method.
A small amount of this material may be mixed with bone graft material for the fusion if necessary. The periosteum is closed using an interrupted no. 0 absorbable suture and the wound closed in layers using subcuticular absorbable suture. The patient is normally placed in a well-moulded short leg cast after surgery as determined by the procedure for which the arthrodesis is indicated.
RESULTS
To date no intra-operative complications have been encountered and the quality and quantity of the bone harvested have been appropriate for the arthrodeses undertaken. Additional autogenous bone graft has not been used in any of the procedures. The cavity created by the harvesting has normally accommodated 8 to 9 mis of substitute bone graft material.
DISCUSSION
The distal tibia provides an excellent source of autogenous bone with relatively low complications 4 . Common potential complications of distal tibial bone graft include wound erythema at the donor site and the potential for nerve parasthesias.
The technique described in the method above has advantages of using a small circular opening to avoid stress riser in the distal tibia and can be done through a relatively small incision to decrease morbidity. The device described facilitates safe rapid harvest of morsellized autogenous graft and the use of a drill affords a degree of control to avoid inadvertent plunging.
The use of low dose fluoroscopy allows precision placement and the optimum site for obtaining of the graft and backfilling of the defect. The bone substitute material facilitates rapid healing of the donor site and reduction of potential morbidity.
SUMMARY
The harvesting of distal tibial bone graft is a safe and effective method of obtaining cancellous bone with well-described good results. The technique described using a hollow bone trephine under x-ray control with backfilling of bone substitute would appear to add safety precision to this technique.
Footnotes
ACKNOWLEDGMENTS
I would like to thank Dr. Nancy Cullen and Mr. Lee Major for their assistance in preparing this paper.