
Abstract
Necrotizing soft tissue processes of the foot secondary to an acute stingray envenomation can be a challenge to manage. Very little is reported in the orthopaedic literature to aid the practicing surgeon faced with this problem. In this case report, we describe the wound management and team approach employed in this patient's care, including the indications for hyperbaric oxygen therapy, which, in this case, was ultimately successful.
INTRODUCTION
Stingrays are members of the class Elasmobranchii, which also includes the sharks. 1 Stingray wounds are inflicted on the foot or the leg when a swimmer, wading through the open water, inadvertently steps upon a ray resting partially buried in the sand. 3 The wound that results from a stingray envenomation is caused by a flick of the ray's tail. 7
The tail of the stingray contains at least one serrated spine, and envenomation by these may result in either jagged lacerations or simple puncture wounds. In approximately two-thirds of documented stingray puncture wounds a protein venom is deposited which causes severe pain and subsequent local tissue necrosis. The venom can cause extensive necrosis of tissue adjacent to the wound even if these puncture wounds are small. 3 The stingray venom contains insidious, but powerful, local tissue necrosis factors for humans and this is felt to be mediated by a heat labile venom 7 .
Initial treatment, therefore, is directed at denaturing this venom as well as providing quick and definitive pain relief. Starks, in 1918, recommended immediate immersion of the affected extremity in water, as hot as tolerable, in order to destroy the heat-labile venom and help prevent tissue necrosis. 7 The application of ice, if heat is not available, is another option, as it may decrease pain and reduce inflammation; however, it has not been shown to effectively denature the venom.
Irrigation of the wound to remove venom, or even immediate surgical exploration to remove venom containing fragments of the sting integument, is also recommended. In fact, some authors believe that all stingray wounds should be explored fully and be examined radiographically for the presence of retained barb fragments- even if the wound appears clean.
In the case presented herein, our patient never received any formal first aid therapy, and, despite later surgical intervention, hyperbaric oxygen therapy (HBO) was eventually utilized to facilitate healing. This paper, therefore, focuses on the natural history and treatment of stingray wounds as well as reviews the indications and proposed mechanisms of action for adjunctive HBO therapy in the treatment of soft tissue processes and management of the wound at risk.
CASE REPORT
A 46 year old female patient presented to the emergency room eleven days after being stung by a stingray over the dorsum of her left third toe. Her history revealed that she had initially responded to warm water soaks, felt better over the course of two days, and then returned to her usual activities, including running. After an additional three to four days a vesicle developed and some serous material drained. Soon thereafter, the area became increasingly erythematous, edematous and painful. One week after the initial sting she was started on Augmentin (500mg po q8h) with no improvement and three days later Doxycycline (100mg po BID) was added for possible Vibrio species with superimposed Staphylococcal and/or Streptococcal cellulitis. An orthopaedic consultation was obtained when the condition of the foot continued to worsen.
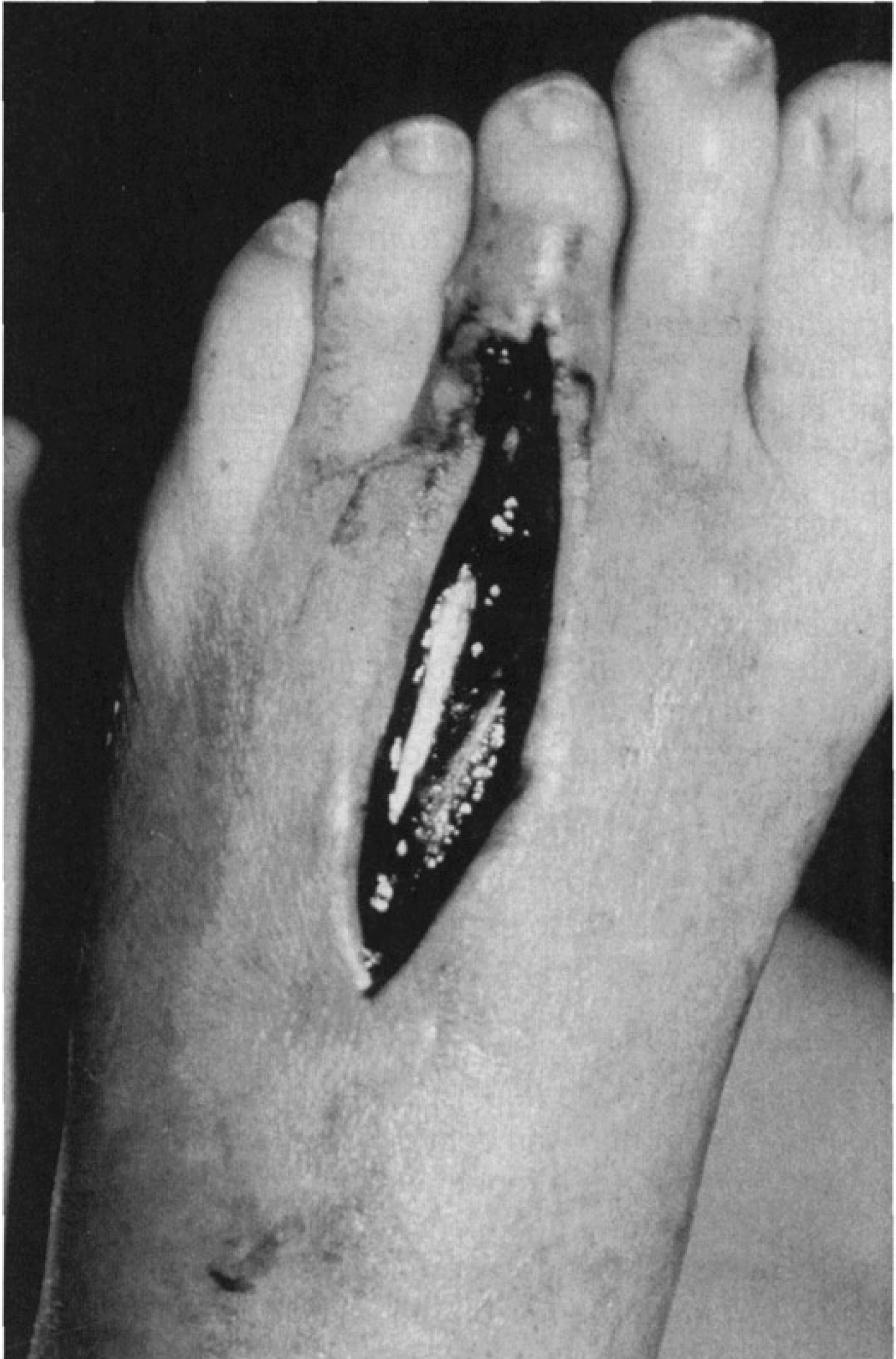
The patient complained of intense pain over the dorsum of the toe and foot which radiated proximally and prevented full weightbearing. She denied any paresthesias or any neurologic symptoms. On examination the patient was afebrile with normal vital signs. Her left foot had a 10 × 14 cm area of erythema and warmth over the mid-dorsum of the foot which extended proximally to the ankle. The skin over the central area (>1cm) was necrotic. A punctate lesion on the dorsum of the third toe was also noted (Fig. 1). There were no areas of fluctuance or drainage. She had no palpable lymphadenopathy. Her neurological exam was normal and she had no pain with passive stretch of her toes. X-rays of the foot were negative for foreign bodies.

Initial presentation to orthopaedics (post-injury day number 11): note the primary puncture site along the base of the dorsal aspect of the third toe. Note also the erythema extending back into the forefoot.
With the tentative diagnosis of Vibrio infection with a superimposed Staphylococcus or Streptococcus cellulitis the patient was admitted for intravenous antibiotics and formal irrigation and debridement. (See Table 1 for antibiotic coverage and medications used during the hospitalization.)
Medication Used per Hospital Day
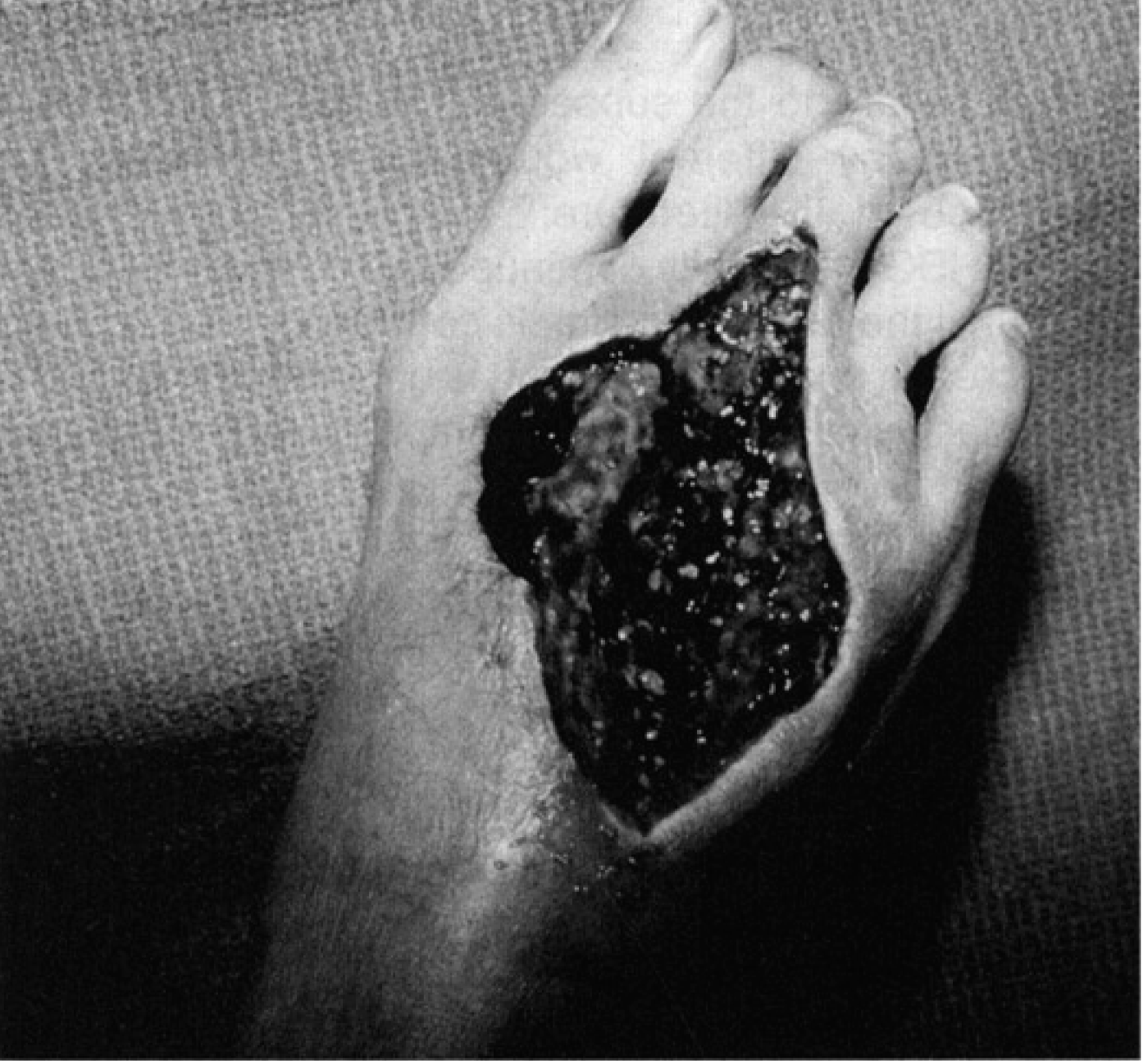
At the time of initial debridement (Fig. 2), an incision was made directly over the dorsum of the third toe along the third metatarsal to the area of necrosis. Necrotic fat and muscle were noted, but most obvious was a green discoloration of the extensor tendon and sheath. Approximately three quarters of the extensor tendon had been destroyed (Fig. 3). No purulent material was found. The wound was debrided and packed open with a plan to return for a repeat washout in 48 hours.
At the time of initial surgical incision: note hemorrhagic muscle.

Further surgical debridement reveals more extensive necrosis.
After the second debridement, hydrotherapy and wet to dry dressing changes were initiated. On hospital day four the patient had a dramatic increase in pain, the area of erythema was increasing and petechiae were noticed on the dorsum of the foot to the ankle. This prompted an immediate return to the OR; where, upon operation, grossly necrotic and liquefied tissue were noted, necessitating a more extensive debridement of the extensor brevis and dorsal interossei. Despite continuation of the hydrotherapy, treating the wound with REGRANEX, and, continued IV antibiotic coverage, the wound required serial debridements (every 24#x2013;48h) over the next three weeks. The debridements consisted of sharp removal of the obviously nonviable skin edges and scraping/excision of tissue using a curette.
Despite the apparent excision of all nonviable tissue at the time of each debridement, the involved wound envelope continued to expand, and, hoping to prevent a further loss of tissue on the dorsum of the foot, hyperbaric oxygen (HBO) therapy was initiated. Upon referral, the wound measured approximately 5×7 cm and was centered over the dorsum of the foot. The extensor tendons of the third and fourth toes had been removed (Fig. 4). The patient had no peripheral leukocytosis or fever. Again, no inguinal lymphadenopathy was present.
At the time of final surgical debridement: note the extensive nature of the underlying pathology.
The hyperbaric regimen consisted of 72 hours of twice daily HBO consisting of 90 minutes at 2.4 ata (atmospheres absolute) followed by final debridement and subsequent split thickness skin grafting from a left thigh donor site to the granulating bed on the dorsum of her foot. After the grafting, the patient underwent four additional days of once daily post-operative HBO at 2.0 ata.
The pathology reports from the multiple debridements confirmed hemorrhagic necrosis in the deep dermal layers as well as in the muscle and tendons. All cultures were negative and special tissue stains did not reveal any organisms or foreign material. The patient had been started on an outpatient antibiotic regimen prior to the debridements, which might have hampered the identification of a pathogen. In some of the early pathologic specimens there was an abundance of eosinophils which were presumed to be indicative of a hypersensitivity reaction. At the time, a course of steroids was initiated, but, when no clinical improvement was noted, the prednisone was discontinued.
Follow-up care was essentially uneventful. At her most recent, six month evaluation, the skin graft had healed completely and she has returned to full activity.
DISCUSSION
In stingray injury cases, where adequate first aid has not been administered, local necrosis, ulceration and/or secondary infection are not uncommon. 5 In addition, clinically resistant localized edema in the area around the stingray wound is a constant clinical finding. 8 Exploration of the wound and excision of hemorrhagic and necrotic tissue are recommended, with one large study of stingray assaults demonstrating that 5% of barbs had broken off of the ray to remain in situ; and, at the time of surgical exploration, had penetrated the skin and the subcutaneous tissue to a depth of approximately four centimeters. The pathology from these cases typically revealed either a foreign body reaction or a more hemorrhagic picture with muscle necrosis coupled with a heavy infiltration of neutophils. 1,5,7
Our patient received minimal first aid after the stingray injury. As she did show some early improvement, it is possible that the venom was denatured by the warm soaks and at initial orthopaedic presentation her diagnosis was more likely a hypersensitivity reaction to a small retained barb. With continued necrosis of the soft tissues the diagnosis quickly became more consistent with a necrotizing soft tissue infection. The causative organism was felt to be Staphylococcus or Streptococcus; however other microorganisms, associated with stingray wounds, such as: Haemophilus parahaemolyticus, Enterobacter sakazakii, Vibrio parahaemolyticus, Pseudomonas aeruginosa, and Acinetobacter anitratum could not be excluded; and, therefore, broad spectrum antibiotic coverage was initiated (See Table 1). 7,13 Although an organism was never identified, it was felt that an infection was the cause of the continued necrotic process.
Although the value of HBO in this type of treatment scenario is debated in the literature 4,6,10,14,15 we elected to offer it as adjunctive therapy in this case where the patient's necrotizing deep space infection seemed to be responding poorly to serial debridement. In this situation, HBO seemed a natural modality for combating the complex pathologic process at hand.
Technically, HBO is the medical treatment in which the patient breathes pure oxygen in a pressurized vessel. Through this process the oxygen carrying capacity of blood is dramatically increased, not so much by changing the saturation level of hemoglobin, but by exponentially increasing the partial pressure of oxygen dissolved in the serum itself. 1,12 This serum hyperoxygenation results in a greater oxygen diffusing capacity at the tissue level, decreases tissue edema, and stimulates the microbicidal properties of white blood cells. 2
As a result of its superphysiologic effect, hyperbaric oxygen improves the chances of survival of marginally viable tissue by increasing tissue oxygen tension in hypoxic tissues to a level at which oxidative cellular function can occur.
In addition to supplying this gradient driving pressure for providing oxygen to ischemic tissue, HBO has also been shown to successfully reduce the edema associated with acute traumatic peripheral ischemias such as that encountered in this case. While the exact mechanism of action by which the vasoconstriction occurs is unclear, it has been repeatedly demonstrated that superphysiologic levels of oxygen do cause vasoconstriction which reduces edema, and, in turn, decreases the distance the oxygen must diffuse from the capillaries to the cells in need. 11
Despite some authors’ enthusiasm for the role of hyperbaric oxygen in the treatment of necrotizing soft tissue infections, it must be emphasized that complete and repeated debridement of all necrotic tissue, along with the administration of appropriate antibiotics, is the real mainstay of treatment, and should be performed every 24–48 hours based on the aggressiveness of the infection. 10 In fact, delay in the time between admission and first debridement significantly affects ultimate outcome. 6
In patients with proven myonecrosis, however, HBO therapy should be considered immediately after surgical debridement. In addition to the above stated effects on tissue oxygenation and edema, once HBO is instituted there becomes a clear demarcation between the necrotic tissue and the remaining viable tissue which aids in performing repeat debridements. 12 This can ultimately reduce the extent of debridement that is needed to control the process.

HBO therapy complete with skin graft in place: no further surgical interventions were required.
With regard to the subsequent foliow-on HBO treatments, many different wound treatment tables are described in the literature; 12 however, as a general guide, HBO is typically continued twice daily for 90 minutes until the active infection is controlled; then, in order to decrease toxicity potential, it is commonly changed to once daily until all potentially compromised wounds are healed. 6
In all patients treated for necrotizing fasciitis, of which patients with injuries to the foot constitute approximately 15%, broad-spectrum antibiotics of various combinations are routinely used, with coverage eventually narrowed based on culture results. As alluded to earlier, however, HBO is also known to augment the effectiveness of antibiotics and can be employed specifically in order to enhance the polymorphonuclear cell phagocytosis of invading microbes. 9,11,12
SUMMARY
Because the heat labile venom has been determined to be the causative agent in early wound necrosis, it is recommended that all stingray wounds be treated initially with hot water soaks in an attempt to denature the venom. If this fails to stop progression of the process, early exploration of the wound for retained barb fragments should be considered. Factors such as progressive erythema and edema and a palpable foreign body should lead to early surgical exploration rather than observation. Exploration should involve opening the entire length on the wound and all involved tissue should be removed. Excision of all venom containing integument should be undertaken. Serial debridements, as often as every two to three days, and broad spectrum antibiotics might be necessary if the necrotizing process continues. Use of hyperbaric oxygen therapy can be beneficial by increasing the patient's ability to mount an effective defense against infection, increasing the potential to heal compromised tissues, and allowing for greater demarcation to aid in the debridement process.
Prevention should always be first in combating a problem. Extensive patient education in susceptible areas to include use of proper footwear, using a shuffling gait while wading in high population sting ray areas as well as proper initial first aid can prevent a majority of stings presenting for medical care.