
Abstract
We previously reported an unexpected statistically significant decline in the mean transcutaneous partial pressure of oxygen (TcPO2) with cutaneous warming from 37°C to 44°C on the plantar diabetic foot, as opposed to the expected increase seen at the dorsal sites. To elucidate this relationship we compared changes with cutaneous warming in TcPO2 and skin circulation measured by laser Doppler flowmetry on the right plantar foot surface of 20 consecutive subjects.
Neuropathy by monofilament testing was present in 55% of the cases. Right dorsal foot TcPO2 increased with cutaneous warming from 37°C to 44° by a mean change of +43.6 ± 20.7 mmHg (± standard deviation) in 95% of the cases. In 42% of cases right plantar first metatarsal head TcPO2 fell with warming from 37°C to 44°C by a mean change of −10.7 ± 7.6 mmHg. In the remaining 58% of cases right plantar first metatarsal head TcPO2 rose by 6.8 ± 6.3 mmHg. In 95% of cases right plantar great toe laser Doppler perfusion units (LDPU) increased with warming from 36°C to 44°C by a mean change of +50.4 ± 37.1. Blood flow measured by laser Doppler flowmetry increased in 95% of the subjects with heating. The finding that blood flow was increased with warming contradicts the hypothesis that arterioles in the plantar great toe cannot vasodilate in response to thermal stimuli.
This finding supports the hypothesis that the decline in TcPO2 with warming might be due to an increase in epidermal oxygen consumption that exceeds the increase in oxygen delivery due to increased blood flow. The pathological mechanisms behind microvascular dysfunction in skin microcirculation in the diabetic foot need further investigation.
We previously reported an unexpected statistically significant decline in the mean transcutaneous partial pressure of oxygen (TcPO2) with cutaneous warming from 37°C to 44°C on the plantar great toe and plantar metatarsal head surface, as opposed to the expected increase seen on the dorsal foot and below the knee. 1 This finding was not due to the presence of diabetes since an even larger drop in TcPO2 at the great toe plantar surface was seen in non-diabetic subjects. This finding did not vary by the presence of autonomic neuropathy or diabetes type among diabetic subjects.
Since TcPO2 is determined by several factors, including cutaneous tissue oxygen delivery, skin diffusion, and epidermal oxygen consumption, we postulated two hypotheses that might explain this seemingly paradoxical decrease:
warming of the great toe plantar surface may have caused vasoconstriction of the plantar toe cutaneous vasculature and diminished blood flow instead of the usual vasodilatory response or warming of the great toe plantar surface may have caused an increase in epidermal oxygen consumption that exceeded the increase in oxygen delivery due to vasodilation.
In support of the first hypothesis Stevens et al. reported a paradoxical decline in microvascular blood flow in response to local heating in their studies of arteriovenous shunt flow using laser Doppler flowmetry on the plantar great toe surface. 2,3 This occurred in subjects with and without diabetes and subjects with and without peripheral neuropathy.
In order to elucidate this relationship we compared changes with cutaneous warming in TcPO2 and skin microvascular circulation measured by laser Doppler flowmetry on the right plantar foot surface of 20 consecutive subjects in the Seattle Diabetic Foot Study.
SUBJECTS AND METHODS
The Seattle Diabetic Foot Study is an ongoing prospective study of risk factors for diabetic foot complications among U.S. veterans. Details of the study design and methods appear elsewhere. 4 The first 20 subjects who reported for testing between July 20,1996, and Oct. 3, 1996, with an intact right foot were included in this sub-study. Eligible subjects were all diabetic patients attending a general internal medicine clinic of the Seattle division of the Veterans Affairs Puget Sound Health Care System. Exclusion criteria included being non-ambulatory or unable to provide informed consent due to medical or psychiatric reasons. Diabetic subjects were identified by review of computerized pharmacy data for receipt of insulin, oral hypoglycemic medication, glucose test strips, and review of medical record problem lists for the diagnosis of diabetes mellitus. A nurse practitioner interviewed subjects using a standard questionnaire to collect data on demographics, diabetes type, duration and treatment. A random venous blood sample was drawn for measurement of glycosylated hemoglobin (Isolab, Akron, Ohio). Only right lower limb measurements are considered in this analysis.
Brachial and lower extremity arterial blood pressures were performed in both limbs by usual segmental Doppler techniques. 5 The ankle arm index was calculated as the ratio of the highest ankle or dorsal foot pressure on the right foot divided by the higher brachial pressure on either limb, except in cases where the ankle blood pressure could not be heard or was > 200 mmHg, indicating incompressible vessels.
Orthostatic blood pressures were recorded in the supine and standing positions and a decrease of 10 mmHg or more was considered to indicate autonomic neuropathy, although we cannot rule out other causes for this result.
Peripheral neuropathy was measured using a 5.07 monofilament (Sensory Testing Systems, Baton Rouge, LA) and coded as insensate if the subject was unable to perceive the monofilament at any of nine standard sites on the right foot.
Measurements of lower extremity transcutaneous oxygen tension (TcPO2) in mmHg were performed at 37°C and 44°C with Radiometer TCM-3 monitors (Radiometer, Copenhagen, Denmark) under uniform conditions at standard locations on the dorsal foot (just proximal to the second toe), and on the plantar surface of the right first metatarsal head. Cutaneous warming with the TcPO2 monitor probe occurred over 20 minutes until the temperature reached equilibrium.
Skin blood flow was measured using the Periflux PF3 laser Doppler flow meter (Perimed, Smithtown, New York) on the plantar surface of the right great toe. The laser Doppler flow meter allows non-invasive measurement of skin blood flow by detecting the intensity of laser light scattered by erythrocytes moving under the sampling probe and the degree of scatter. The Periflux PF3 flow meter uses a double channel probe with a standard low power laser emitting an infrared beam. A warming ring surrounds the probe. The signal recorded from the digital signal receiver is expressed as laser Doppler perfusion units (LDPU), the number of blood cells moving in the measured volume multiplied by the velocity of these cells. We also recorded the concentration of moving blood cells (CMBC) which is a measure of the intensity of reflected light. A reading at 36°C was recorded, as well as a reading at 44°C after 10 minutes of cutaneous warming.
These sites were chosen because other investigators proposed that the plantar surface of the great toe represented a site where skin blood flow was dominated by arteriovenous shunt flow and the dorsum of the foot represented a site without anastomotic flow. 3
Mean values were compared using the unpaired two tailed t-test, the Mann Whitney U test, and linear regression for continuous variables. The significance of mean differences was assessed using the paired t-test. 6
RESULTS
There are 20 male subjects in this analysis, with a mean age of 60.7 ± 10.2 years (± standard deviation) (range 45 to 76 years). The subjects were 80% white race and had primarily type 2 diabetes mellitus (85%) with a mean duration of diabetes of 8.6 ± 7.8 years. The majority of the subjects (60%) were treated with insulin while the remaining subjects were treated with oral hypoglycemic agents. Their blood glucose control as indicated by a single glycosylated hemoglobin (HbA1 c) at study entry averaged 9.2% ± 3.0% (standardized to a non-diabetic reference range of 4.6 to 6.6%).
Fifty-five percent (n = 11) of the subjects were insensate to the 5.07 monofilament at one or more sites on the right foot. Almost half (47%, n = 9) of the subjects had a blood pressure drop of 10 mmHg or more upon standing. Only one subject (5%) had a blood pressure drop of 30 mmHg upon standing.
The mean transcutaneous oxygen tension (TcPO2) and laser Doppler measures (LDPU and CMBC) on the various sites of the right limb with and without heating are shown in the table.
Results of transcutaneous oximetry and laser Doppler flowmetry on the right foot before and after cutaneous warming as described in the text are means ± standard deviations (SD).
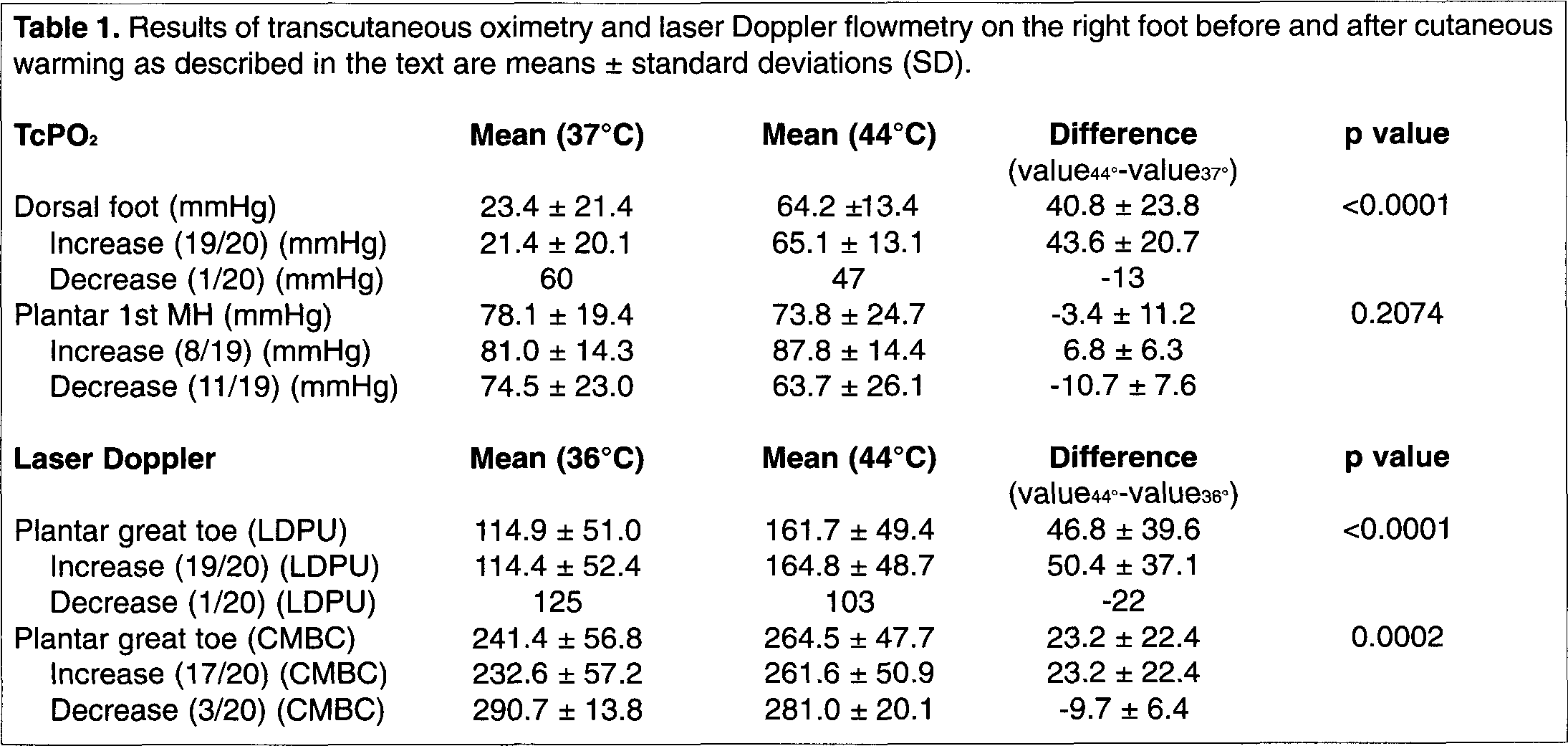
In 19 of the 20 cases (95%) right dorsal foot TcPO2 increased with cutaneous warming from 37°C to 44°C and decreased in one case (5%). The mean change in right dorsal foot TcPO2 readings when an increase occurred was +43.6 ± 20.7 mmHg (range one to 74). There was a decrease of −13 mmHg in the one subject whose TcPO2 fell with warming. The TcPO2 value at the starting temperature of 37°C was considerably higher in the subject who had a decrease in right dorsal foot TcPO2 (60 mmHg) than the mean starting value (21.4 ± 20.1 mmHg) in the subjects who had an increase in TcPO2 with warming to 44°C. The mean TcPO2 value at the ending temperature of 44°C was 65.1 ± 13.1 mmHg in subjects who had an increase in TcPO2 with warming at the right dorsal foot location.
In 11 of 19 cases (58%) right plantar first metatarsal head TcPO2 decreased from 37° C to 44° C and increased in eight cases (42%). The mean change in eight right plantar first metatarsal head TcPO2 readings that increased or stayed the same was +6.8 ± 6.3 mmHg (range zero to 19). There was a mean decrease of −10.7 ± 7.6 mmHg in the 11 TcPO2 readings that fell with warming. Overall mean change in plantar first metatarsal head TcPO2 with warming was −3.4 ± 11.2 mmHg.
The TcPO2 values at the starting temperature of 37°C in subjects who did and did not have a decrease in right plantar first metatarsal head TcPO2 with warming to 44°C were not significantly different (81.0 vs. 74.5 mmHg, p = 0.4877) but the TcPO2 values at the ending temperature of 44°C were significantly different (87.8 vs. 63.7 mmHg, p = 0.0315).
In 19 of the 20 cases (95%) right plantar great toe LDPU increased with warming from 36°C to 44°C and decreased in one case (5%). The mean change in right plantar great toe readings that increased was +50.4 ± 37.1 LDPU (range five to 150). There was a decrease of −22 LDPU in the plantar great toe reading that fell with warming. The value at the starting temperature of 36°C was 125 LDPU in the subject who had a decrease in right plantar great toe LDPU while the mean starting value in the subjects who had an increase in LDPU with warming to 44°C was 114.4 ± 52.4 LDPU. The mean value at the ending temperature of 44°C was 164.8 ± 48.7 LDPU in subjects who had an increase in LDPU with warming at the right plantar great toe.
There was no significant difference in laser Doppler readings at 36°C, 44°C, or the change in laser Doppler values by sensory or autonomic neuropathy status. There was no significant difference in TcPO2 readings at 37°C, 44°C, or the change in TcPO2 values by neuropathy status.
By regression analysis, laser Doppler readings on the plantar great toe at 36°C were not significantly associated with TcPO2 values at 37°C on the dorsal right foot or the plantar right first metatarsal head. Laser Doppler readings on the plantar great toe at 44°C were not significantly associated with TcPO2 values at 44°C on the dorsal right foot. However, laser Doppler readings on the plantar great toe at 44°C were significantly and positively associated with TcPO2 values at 44°C on the plantar right first metatarsal head (p = 0.0471) by regression analysis.
DISCUSSION
In 58% of subjects an increase in TcPO2 with warming occurred at the right first metatarsal head. However, an unexpected paradoxical decline with warming in TcPO2 at the right first metatarsal head was demonstrated in 42% of our subjects. While this is not as striking as our previous report of a paradoxical mean decline with warming in TcPO2 readings at the plantar great toe surface over 656 subjects, 1 it is still disconcerting. One cannot always assume that readings obtained at 44°C on the plantar surface represent maximal tissue oxygenation as might logically be expected.
Blood flow measured by laser Doppler flowmetry increased in 95% of the subjects with heating. The finding that blood flow was increased with warming contradicts the hypothesis that arterioles in the plantar great toe cannot vasodilate in response to thermal stimuli. This finding of increased blood flow with warming is contrary to a previous report that showed laser Doppler blood flow declines with local heating to 65% of its resting value in diabetic patients with neuropathy. 3 Differences in equipment, methods or the depth of the laser Doppler probe may account for these contradictory findings.
In our earlier report we proposed that the decline in TcPO2 with warming might be due to an increase in epidermal oxygen consumption that exceeds the increase in oxygen delivery due to increased blood flow. Our current finding supports this conclusion indirectly, since blood flow did not fall on average over the plantar toe surface in response to cutaneous warming. A direct demonstration of increased oxygen consumption by the skin at this location with warming would serve to directly support this conclusion.
In the clinical setting, TcPO2 readings have been used to predict wound healing 7 and determine appropriate treatment. 8 The data presented here bring into question whether the warmed or unwarmed plantar foot TcPO2 should be used to make these decisions. Since cutaneous warming can lead to a decrease in these measurements it may not be appropriate to extrapolate results from other sites typically done at 44°C to measures done at plantar sites. The TcPO2 values obtained at 37°C may represent maximum tissue oxygenation.
This finding supports the hypothesis that the decline in TcPO2 with warming might be due to an increase in epidermal oxygen consumption that exceeds the increase in oxygen delivery due to increased blood flow.
Footnotes
ACKNOWLEDGMENT
This work was supported by the Department of Veterans Affairs Merit Review Rehabilitation Research and Development grants.