
Abstract
One hundred and two cases of displaced intra-articular fractures of the calcaneus were treated using this method for manual reduction. All but three were treated within three days of injury. The average follow-up was seven years and three months (range three to 14 years). Patients' ages ranged from 21 to 76 years. Results were assessed by clinical outcome as well as roentgenographic appearance. Successful reductions were obtained in 92 cases. In the remaining 10 cases, the reduction was felt to be unsatisfactory and either percutaneous pinning or open reduction internal fixation was performed. In most cases fractures were reduced and treated successfully using this method of manual reduction. The use of this method does not preclude any further treatment options, and we therefore feel this method is the treatment of choice.
INTRODUCTION
Many treatments for displaced intra-articular fractures of the calcaneus have been tried, but until recently manual reduction has been considered impossible and unrealistic. In 1983, however we presented a new method of manual reduction utilizing the tension of the ligaments around the calcaneus. 7 At that time, there were 11 cases treated using this method. Since that initial report, more than 160 cases have been treated, and the results have proven to be quite satisfactory. Indications and limitations of this method are becoming clear. We here describe our procedure for manipulation, its theoretical background, and limitations of the method using manual reduction in detail.
MATERIALS AND METHODS
From 1979 to 1993, a total of 164 patients were treated using this manipulation. Of this group, 102 patients (98 men and four women) were studied and followed for more than three years. Sixty-two out of 164 patients did not return for follow-up, despite written requests for them to come in for long-term follow-up. However, these patients showed good results as their fractures were reduced in the short period (four months or longer) that we saw them. The remaining 102 patients were examined directly and evaluated accordingly. Average follow-up after manipulation was seven years three months (range three to 14 years). Patients' ages at the time of manipulation ranged from 21 to 76 years.
At follow-up, Maxfield's clinical criteria and plain radiographs (lateral, AP, axial, and Anthonsen's views) were used to evaluate fractures. Maxfield 6 described the clinical criteria as follows:
Excellent: These patients denied any restriction of activities, denied all pain, and said that they could perform any activity that they wished.
Very good: These patients did not complain of any serious interference with their activities, but they did have some minor complaints.
Fair: These patients have some restriction of activities because of pain.
Poor: These patients continued to complain of pain.
Procedure for Manual Reduction
This method should be performed within three days after the injury. Spinal anesthesia is usually used. The patient is placed in a prone position with the knee of the affected leg bent at a 90° angle. An assistant holds the thigh in this position. The operating surgeon stands at the patient's feet.
The surgeon grasps the medial and lateral sides of the heel and clasps the fingers of both hands together over the sole of the heel (Fig. 1). The heel is then compressed and the calcaneal tuberosity is repeatedly squeezed using strong traction in a longitudinal direction away from the body. Strong traction may lift the patient's thigh off of the table, even when the assistant is holding the thigh down. While the patient is in this position, the surgeon should quickly bend the talocalcaneal joint into varus and valgus positions alternately with interlocked hands. Repeating the wrist action in a back-and-forth or rocking motion makes it possible to move the joint to the maximum extent.

Manual reduction method. The calcaneal tuberosity is squeezed using strong traction and quick bending of the talocalcaneal joint into varus and valgus.
Although this manual reduction is relatively easy to perform and takes only a few moments, the following recommendations should be noted:
Both palms should hold the affected region distal from the site of attachment to the calcaneofibular ligament.
Strong traction and quick bending toward varus and valgus positions should be applied. If the manipulation is performed slowly, the entire leg moves, and no effective force is applied to the subtalar joint.
The assistant should hold the thigh to prevent lifting of the thigh by the traction applied by the surgeon.
Drawing the affected foot toward the surgeon's chest facilitates manipulation and potentiates the force applied.
The surgeon should wear wet cotton gloves to assist in obtaining a firm grip when performing this manipulation.
By following these recommendations, reduction can be achieved in most cases. This technique is easy to perform and takes only a few moments. Crepitations usually occur during manipulation but subside as the fracture is reduced.
The mechanism by which this manual reduction works can be explained in these simplified illustrations (Fig. 2, a-c). At the time of injury, the joint fragment is depressed into the distal fragment. Strong traction and adductive manipulation create a varus orientation at the subtalar joint and in the fractured region. When the ligaments are intact, however, the joint will not open excessively due to ligamentous restraint. Therefore, when manipulation is performed in the region of the fracture, a compression fracture can be released from the “bite” position. At the same time, spreading is reduced to almost normal width. Therefore, with subsequent adductive manipulation, the displaced joint-fragment canbe pushed up by the distal fragment, and reduction can be achieved.
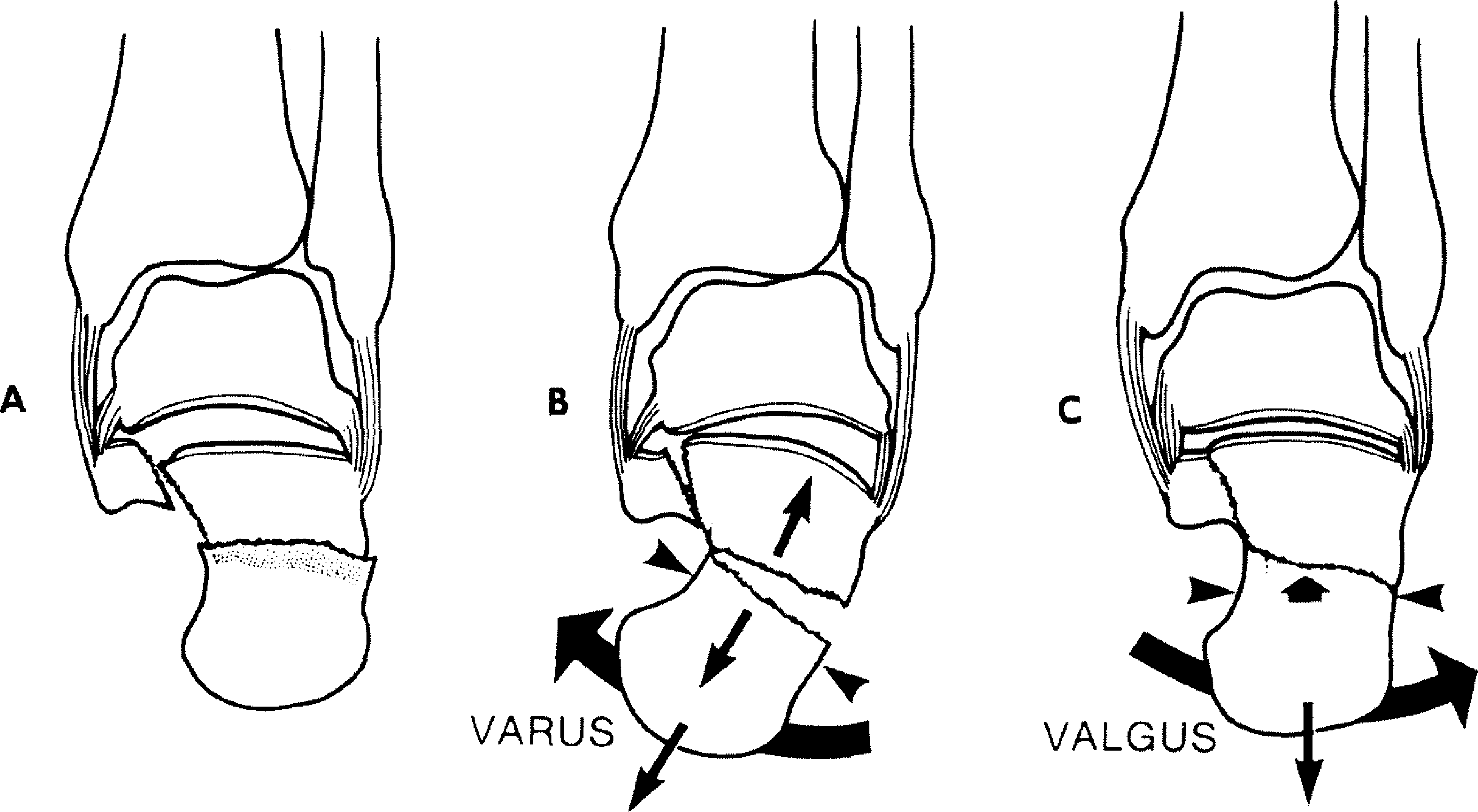
From DeLee
5
(Redrawn from Omoto et. al.
7
).
Post-Reduction Treatment
Generally, a plaster cast is not required after the reduction, because the fragments are interlocked with one another. The soft tissues around the calcaneus, the inferior peroneal retinaculum, and the peroneal tendon sheath help to retain the reduction. We have recently begun using a below-the-knee walking cast with the ankle in 45° equinus. The cast is bivalved with anterior and posterior half shells so that the patient can remove it and perform active-motion exercises. The patient can walk with the cast when it is affixed with tape or a bandage.
One day after the reduction, the patient is encouraged to begin motion. After the swelling decreases, thermotherapy such as a vibra-bath is started, and a walking brace similar to the cast is applied (Fig. 3). A program of graded active exercises is then prescribed. About one month after reduction, the patient begins weight-bearing exercises by walking in a pool. About two months after reduction, the patient is allowed to walk using an arch support and crutches. Three months after reduction, the patient can walk without using any support. Four months after reduction, most patients can return to work.
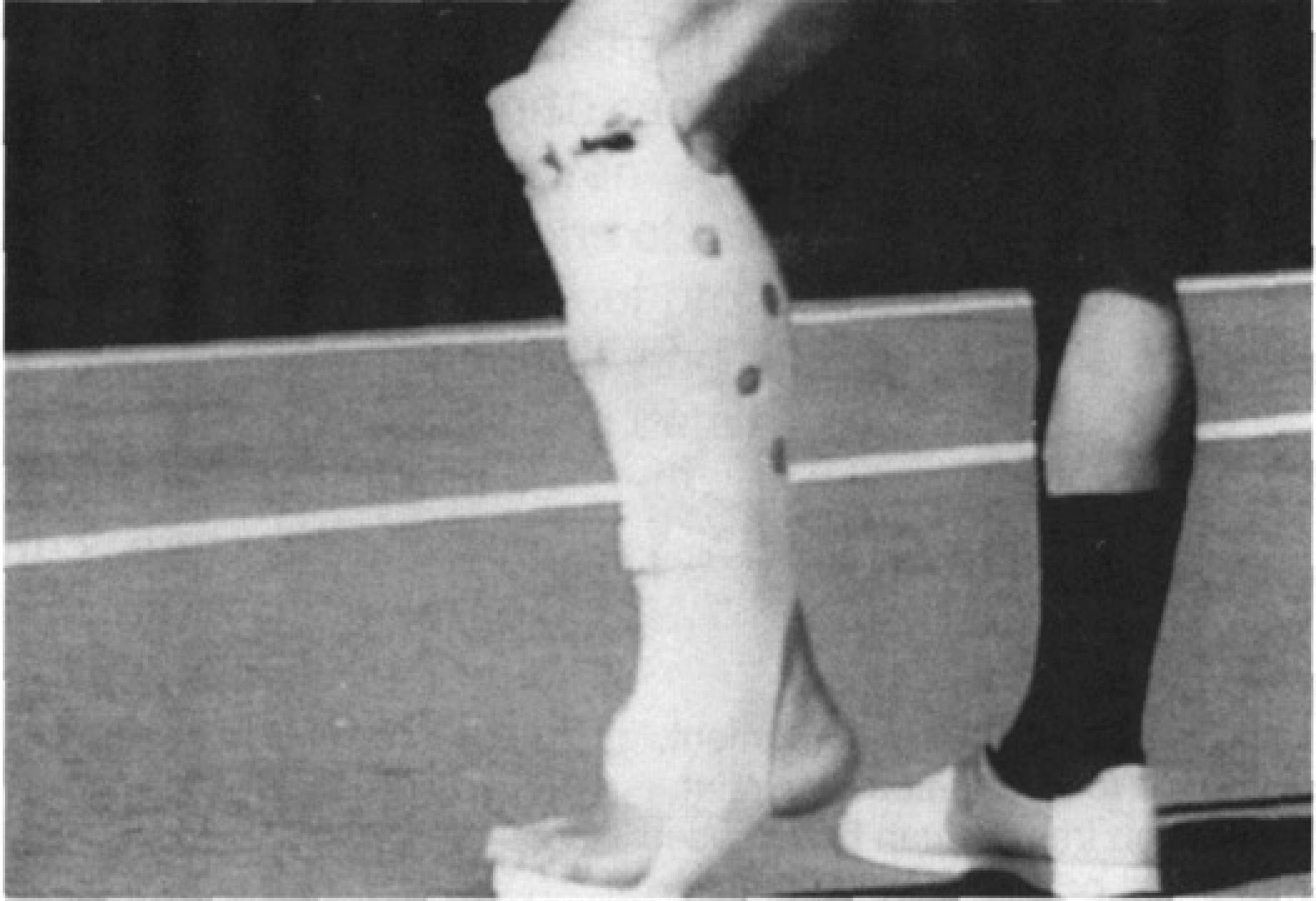
A below-the-knee walking brace is applied with the ankle in the equinus position at 30° and the forefoot bearing the weight.
Cases
RESULTS
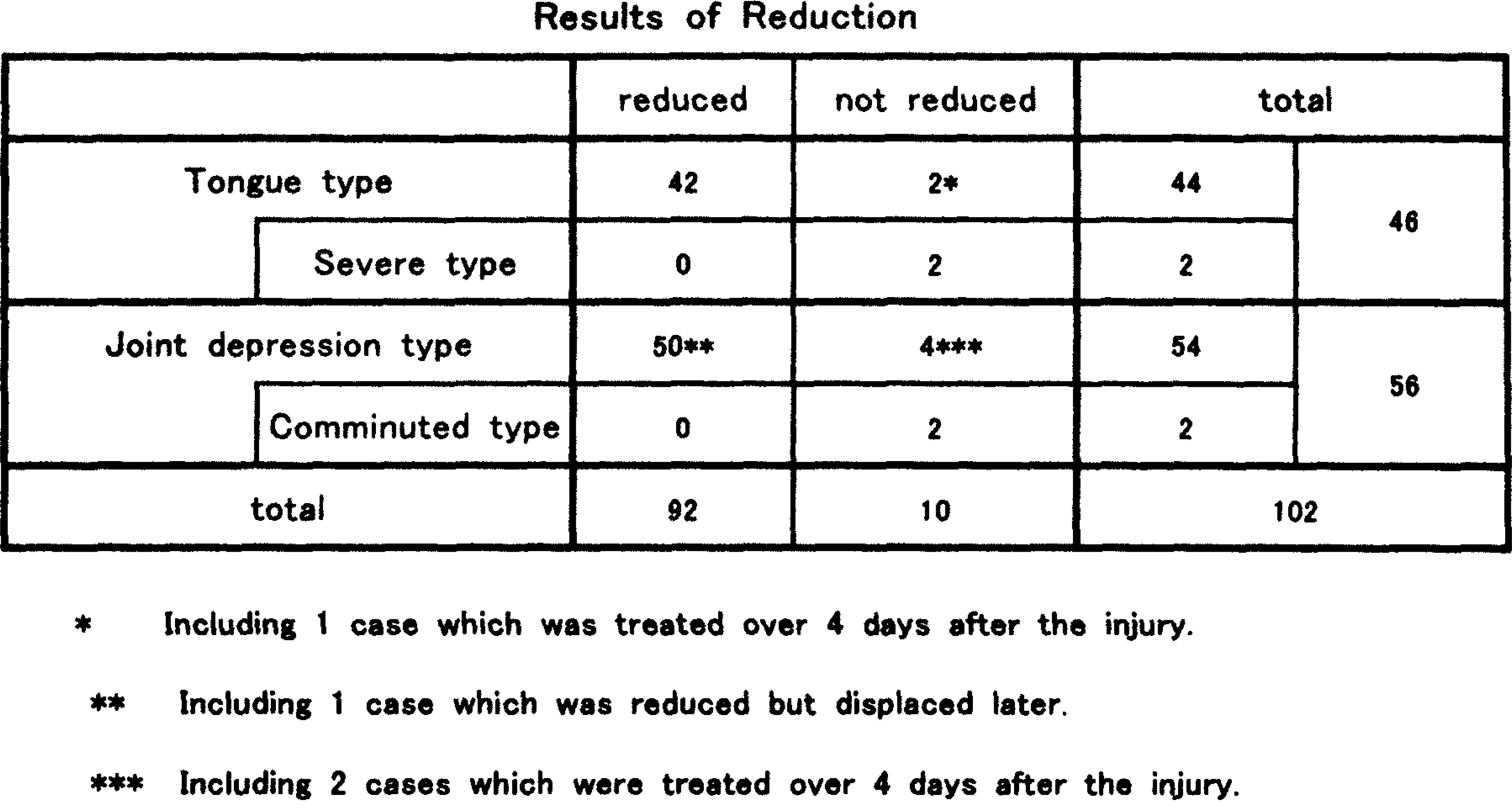
All but three cases were treated within three days of injury and successful reductions were obtained in 92 of the 102 cases. These fractures were reduced by the manual reduction technique without invasive open reduction and were followed by early exercise involving motion and early weight-bearing. In the remaining 10 cases, it was not possible to achieve a closed reduction (Table 1). Analysis of the 10 cases revealed that three of the 10 patients came to our hospital six to 14 days after injury and this delay after injury precluded manual reduction. The calcaneofibular ligament was torn in another case. The six other patients were divided into three groups as follows:
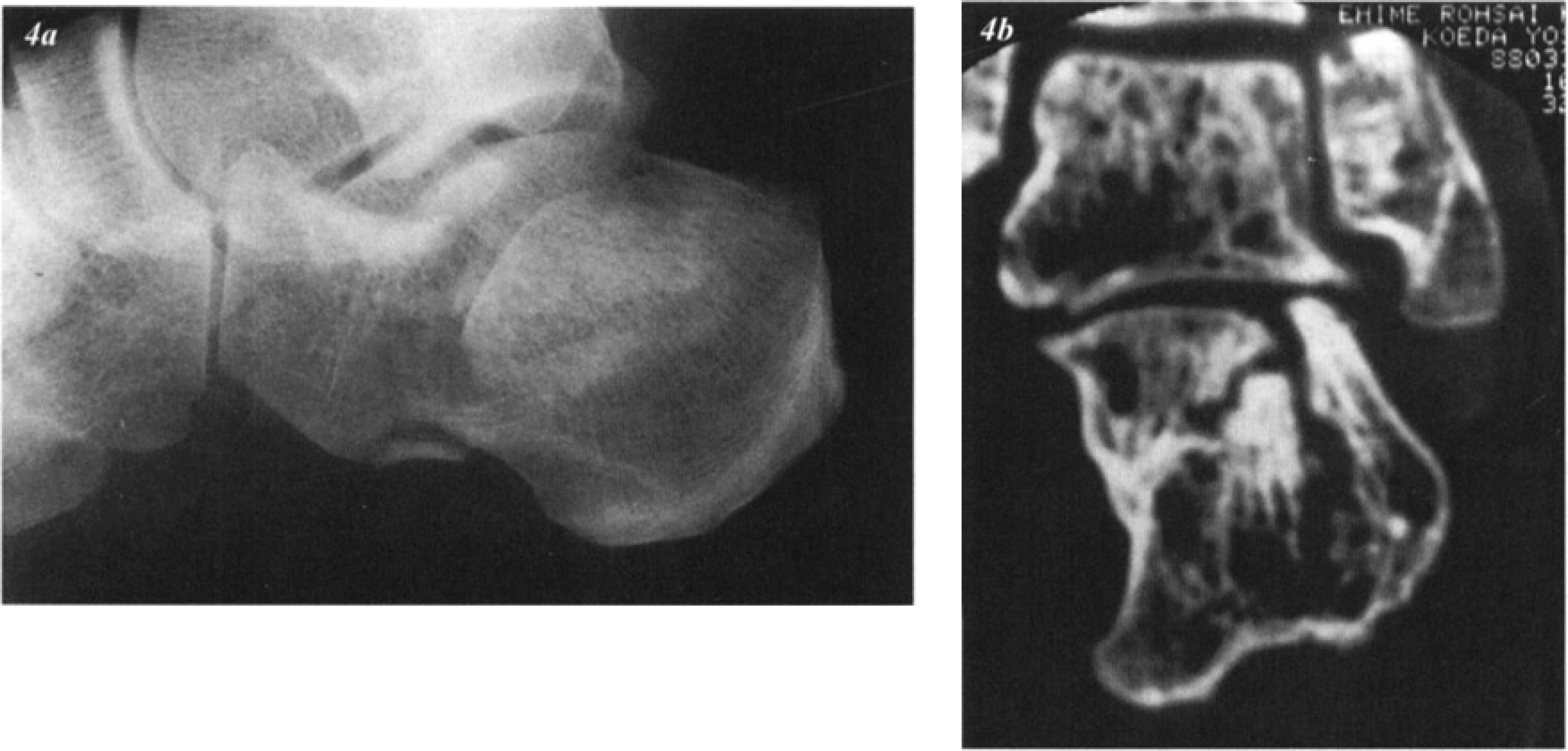
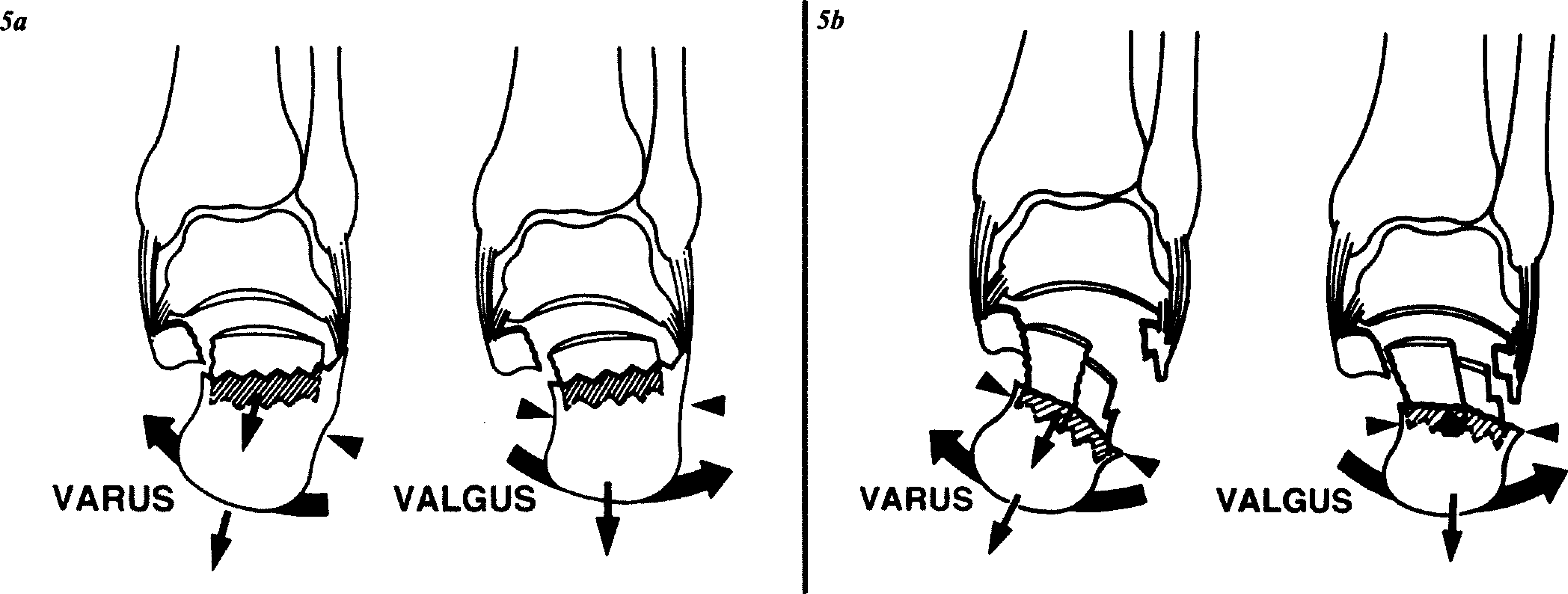
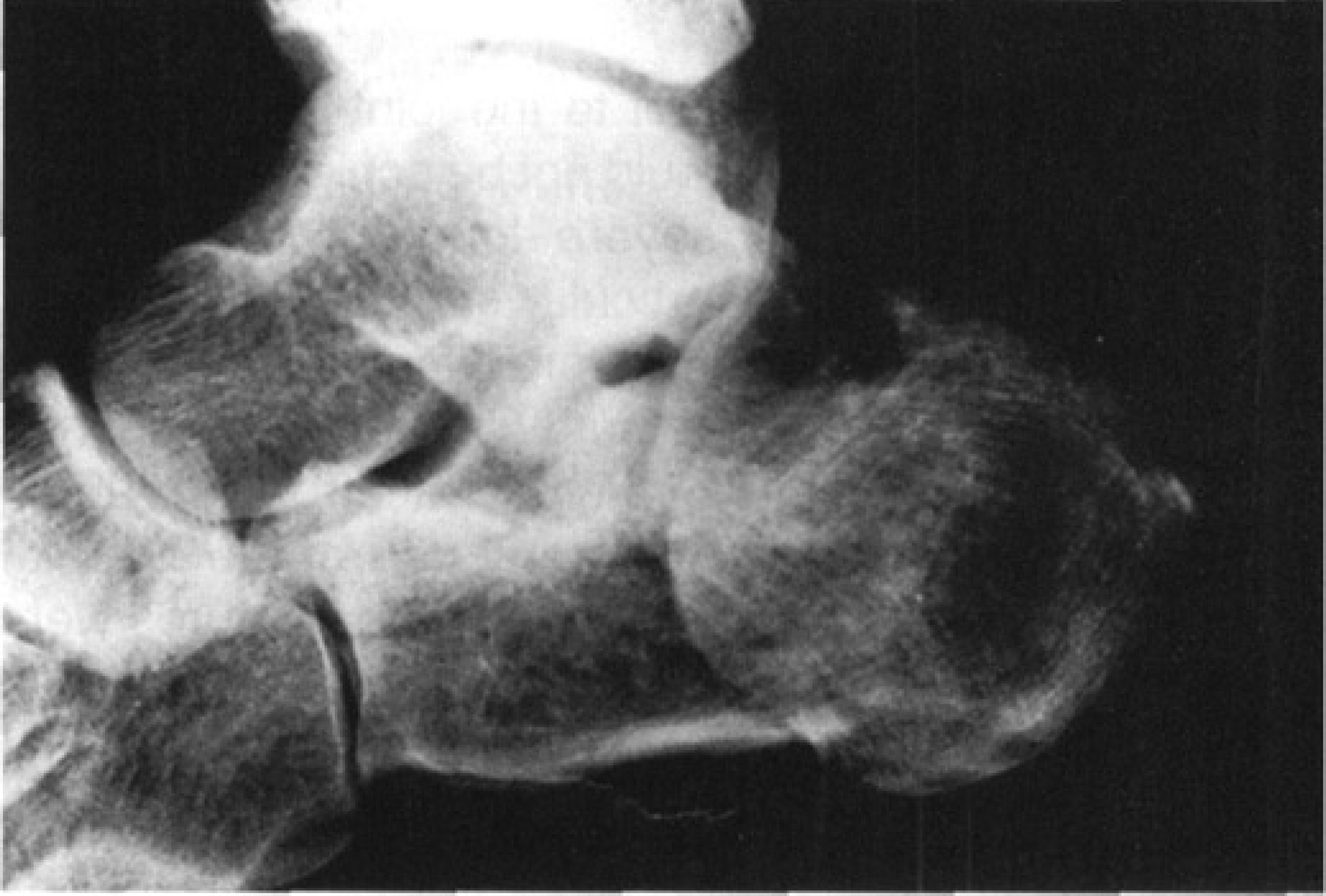
Two patients had joint-depression types of fractures without comminution but with the calcaneofibular ligament detached from the displaced fragment. One case was a two-diagonal type of fracture. Although the lateral radiograph showed that the joint-fragment was depressed without rotation, CT-scanning revealed that only the central articular surface was depressed, while the lateral part was preserved (Fig. 4a, 4b). In the other case, the joint-fragment was too small and without ligamentous attachment. In these two cases, the calcaneofibular ligaments were attached to the distal fragment and not to the joint-fragment, and therefore reduction could not be achieved (Fig. 5a).
Joint depression type (a two-diagonal type).
Two patients had severe tongue-type fractures involving the entire articular surface with rotation, and the joint-fragments were lying near the plantar surface of the calcaneus. These were different from the usual tongue-type fractures that commonly involve only the lateral part of the articular surface. These severe tongue-type fractures were similar to Soeur's third-degree type. 9 Although the joint-fragments had ligamentous attachment, the joint-fragments were so big in both cases that the reductionary force of manipulation was insufficient to restore them to their proper location (Fig. 6).
Two patients had joint-depression types of fractures with comminution and with the calcaneofibular ligaments attached not to medial displaced fragments but to the lateral fragments. The lateral joint-fragments had ligamentous attachment, but medial fragments were comminuted into so many pieces that the force of manual reduction to the medial fragments was ineffective (Fig. 7).
Severe tongue type. Comminuted joint depression type.
The joint-depression type of fracture is slightly more difficult to reduce than a tongue-type fracture. Most cases of tongue-type fracture are easily reduced. All cases reduced, except for three with fair results, had 56 excellent and 33 very good results according to Maxfield's clinical criteria. Most patients had no complaints at follow-up.
DISCUSSION
The technique described above for manual reduction is particularly effective when the calcaneofibular and the lateral talocalcaneal ligaments are intact. Calcaneal fractures are usually caused by a fall from a height and since the calcaneus receives mostly direct vertical forces, the ligaments surrounding the calcaneus remain undamaged in most cases. These ligaments restrict abnormal or excessive movements of the talocalcaneal joint, and manual reduction utilizes the tension of the intact ligaments. The calcaneofibular ligament plays the most important part in this method.
In rare cases, reduction cannot be achieved. For example, when the ligament is not attached to the joint-fragment but remains with the distal fragment, or when the fragment attached to the ligament has completely broken away from the main joint-fragment, the impacted joint-fragment moves with the distal fragment and cannot be reduced because of the lack of ligamentous restraint to control movement of the joint-fragment (Fig. 5a, 5b). In most calcaneal fractures, however, reduction can easily be achieved by utilizing the tension of the ligaments around the calcaneus.
In the treatment of calcaneal fractures, radiological findings must first identify the type of fracture. There are many ways to classify the types of fracture, but the one used most commonly by us is by Essex-Lopresti (Fig. 8). This classification divides the intra-articular fractures into a “tongue-type” and a “joint-depression type,” with or without comminution. Essex-Lopresti recommends closed reduction with an axial percutaneus pin for the tongue-type, and open reduction for the joint- depression type. 3 Although classifications using CT scans can indicate the use of a closed or a open method of reduction, it is sometimes difficult to determine whether the type of fracture is tongue-type or joint-depression type even with CT scan.
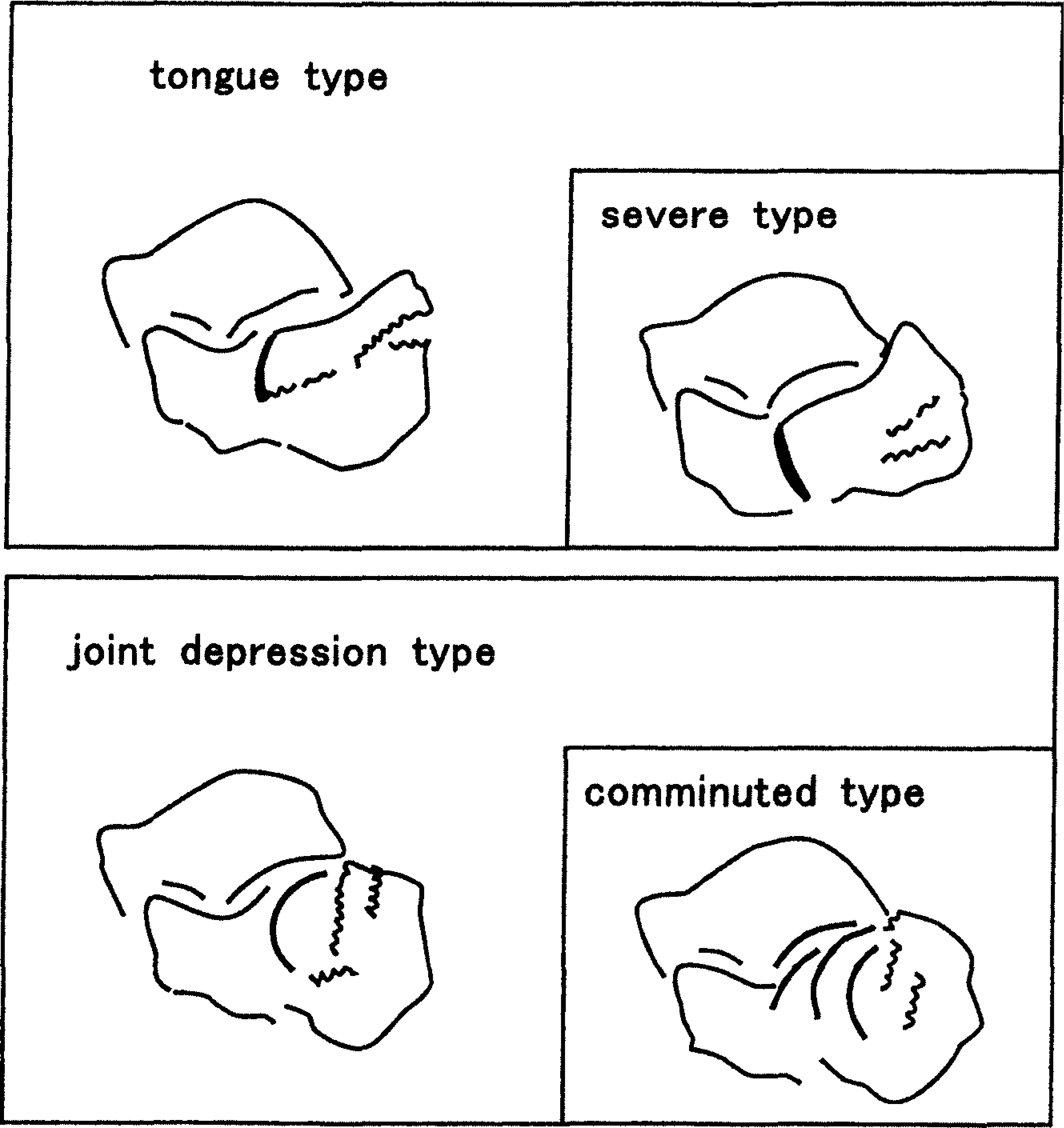
Classification of displaced intraarticular calcaneal fractures.
In a joint-depression type fracture, usually only the lateral articular surface of the posterior facet is displaced with rotation, but when the injury is severe there may also be fragmentation of the entire surface into many pieces. On lateral radiographs, comminuted joint-depression type fractures can be diagnosed by observing double or triple subchondral bone lines in varied degrees of rotation. This type of fracture may be comparable to gross comminution of the joint-depression type according to the Essex-Lopresti classification, and also comparable to Sanders' type III and IV fracture. That is, manual reduction cannot be achieved because restraint by the calcaneofibular ligament cannot easily control movement of the medial joint-fragments (Fig. 5b). In such cases, open reduction is required instead of further manual reduction.
The incidence of irreducible calcaneal fractures is small and, consequently, most cases can be successfully treated by manual reduction, if it is performed within three days after injury.
Crosby reported that fractures in the pattern he called type II (displaced more than 2 mm but not comminuted) did not yield acceptable results when treated with the closed method, and he recommended that type II fractures be treated with open reduction and internal fixation. 2 Sanders stated that most displaced intra-articular calcaneal fractures of type II were amenable to operative intervention, with good results and return to work to be expected. 8 His type III fractures occur less frequently and have a worse prognosis. Patients should be counseled that there may be resultant disability and the possible need for a late subtalar fusion. Crosby's type II and Sanders' type II fractures seem to be similar, and these types are also the same as tongue- and joint-depression types of fractures. Crosby's type II and Saunders' type II fractures can easily be reduced using manual reduction technique described above. Complications were rare when we used this manipulation for such cases, and in view of the reported rate of possible complications (as high as 53% after operative treatment 1 ), nonoperative treatment of type II fracture should be the first choice.
The manual reduction technique is a noninvasive procedure that utilizes the tension of the ligaments around the calcaneus to reduce calcaneal fractures within a very short period. This method can be performed on patients of all ages, using spinal anesthesia, and also on an outpatient basis on the day of or shortly after the injury. Furthermore, early exercises involving motion and early weight-bearing on the forefoot reduce the healing time and side-effects of the fractures. The most important objective of postreduction treatment is to avoid loads on the calcaneus while applying loads to other regions to prevent atrophy of bone, contracture of the small joints, and formation of scar tissue. If attention is not paid to such potential complications, the therapeutic result will be poor regardless of the perfection of the anatomical reduction. 4
SUMMARY
Our results show that the manual reduction technique we describe produced satisfactory results in certain intra-articular fractures of the calcaneus. This procedure requires only a few minutes to perform and does not preclude use of other treatment later. If the reduction fails, the patient may still undergo open reduction and internal fixation or percutaneous reduction. It is our recommendation that this manipulation be tried first, before open reduction and internal fixation. This technique is noninvasive and utilizes the tension of the ligaments around the calcaneus to reduce the calcaneal fragments. Furthermore, early exercises involving motion and early weight-bearing on the forefoot reduced the healing time and side-effects of the fracture. This method can be performed on an outpatient basis on the day of or shortly after the injury. This method of manual reduction may be considered to be the first choice of therapy for displaced intra-articular calcaneal fractures by successfully reducing fractures in most cases, if it is performed within three days after the injury.