
Abstract
A new method of repairing Achilles tendons, which uses a small medial skin incision with a Bunnel-type suture, was performed on 14 patients, and the clinical results were found satisfying. In order to restore the Achilles tendon to its original length, restore tensile strength in the suture site, and minimize injury to the sural nerve, an operative procedure has been devised which uses a limited open repair with a Bunnel-type suture. We followed 14 patients who had undergone the new procedure for a mean interval of 26 months after the injury. They returned to work in six weeks and to playing sports in 25 weeks. There were no cases of late rerupture nor injuries to the sural nerve. This technique approximated the preinjury length and resting tension of the musculotendinous apparatus and minimized sural nerve injury.
Keywords
INTRODUCTION
Percutaneous repairs of ruptured Achilles tendons have a low failure rate and negligible wound complications. 4,6 Even so, they do have a higher rate of rerupture (6.4%) than open repairs (2.7%). 1,11 Percutaneous repairs may not achieve satisfactory contact of the tendon stumps or gain tensile strength for the early postoperative functional rehabilitation. It may take longer to heal, the original length of the tendon may not be accurately restored, early postoperative functional rehabilitation may be impossible and there is the possibility that rerupture and tendon lengthening will impair the function of the triceps surae. 5
Using the Ma-Griffith technique, which employs six skin incisions, 4 Rowley and Scotland (one of 10) as well as Klein (five of 38) 9,3 reported injury of the sural nerve. Webb 12 performed detailed studies on the anatomy of the sural nerve. He stresses that the significant individual variation in the position of the sural nerve in relation to the Achilles tendon should be borne in mind when placing sutures in the proximal part of the Achilles tendon. Therefore, percutaneous sutures should not be performed on the lateral half of the Achilles tendon. Our purpose is to report on a modification of a new technique to repair ruptured Achilles tendons that would restore the original length of the tendon, increase tensile strength and decrease risk of injury to the sural nerve.
MATERIALS AND METHODS
From December 1995 to February 1997 at Gil Medical Center, limited open repair was performed on 14 patients with spontaneous rupture by one surgeon. They consisted of 13 males and one female with a mean age of 36 years (range, 32 to 52) who had sedentary occupations and were recreational athletes. The tendon was repaired under general anesthesia within four days. All patients were reviewed personally at an average of 26 months (range, 21 to 32) after the injury.
Operative Technique
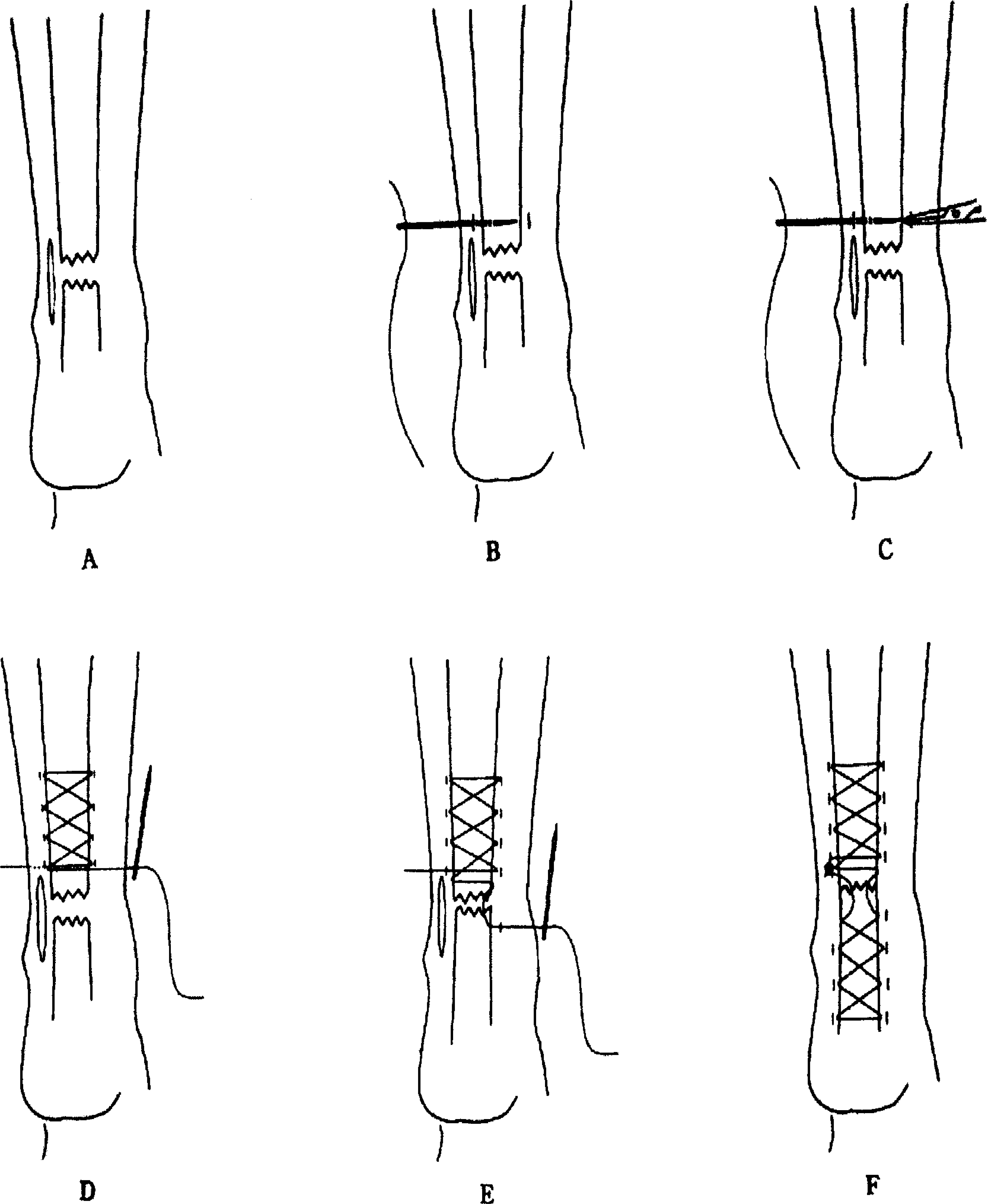
The patient is prone on the operating table with the leg exsanguinated. A 3–4 cm longitudinal incision is made on the skin just medial to the palpable gap on the tendon (Fig. 1a). The paratenon is not opened and a small curved haemostat is used to define the track into the tendon itself. Small puncture skin incisions are made longitudinally parallel to the tendon with a no. 11 scalpel (Fig. 1b). With a mosquito clamp, blunt dissection is performed through the subcutaneous tissue of the tendon and then suture under vision through the small puncture skin incision to avoid the sural nerve (Fig. 1c). A Bunnel-type suture is used in the tendon with a long straight needle and #3 cottony Dacron. When using a Bunnel-type suture, tension should be maintained with Dacron in order to prevent a gap from opening in the suture site (Fig. 1d). Direct observation confirms that the space between the two stumps has been eliminated with little accordion effect and minimal strangulation of the tendon (Fig. 1e). The ankle is then placed in a few degrees more plantarflexion than the position of resting equinus while the suture repair is performed. The suture knot is buried within the medial aspect of the paratenon (Fig. 1f). No drain is used.
Operative technique
Closure of the skin is accomplished with the foot maintained in a plantarflexed position to keep tension off the area of repair. A well-padded below-ankle cast is applied with the foot in about 30° of equinus.
Postoperative Management
For three to five days, the wound is inspected and a more firmly fitting short leg equinus cast is applied. After about two weeks, the short leg cast is replaced and a neutral posture is obtained for another four weeks. At six weeks, the cast is removed and the patient is placed in a shoe with a 1-inch heel lift and partial weight-bearing is allowed. Then the patient wore, on the opposite, uninjured extremity, a shoe which had a 1-inch heel lift added.
RESULTS
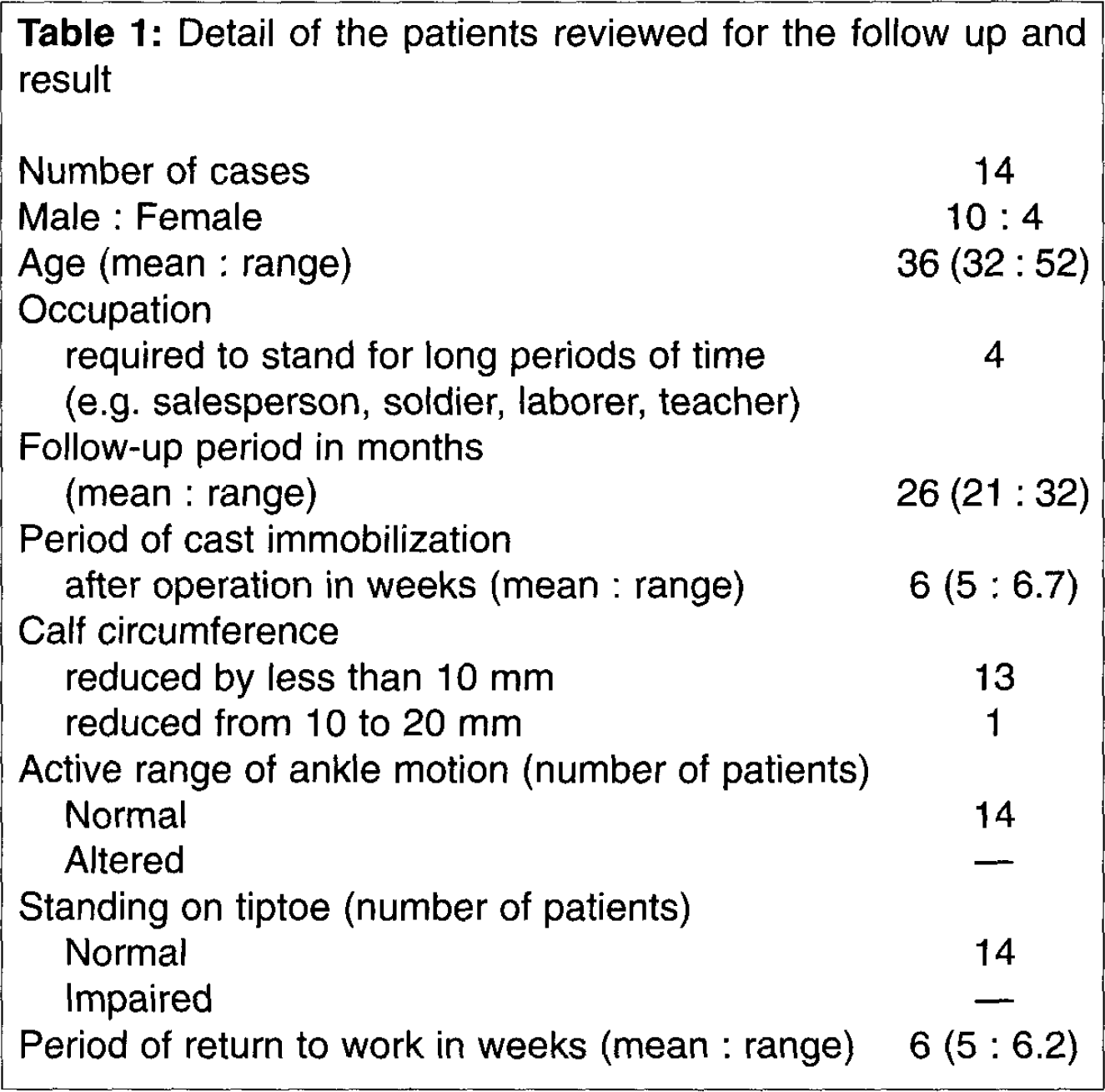
All the tendons healed primarily with no breakdown of the wound, no rerupture, and no sural nerve injury. All patients recovered a full range of ankle movement. It took six weeks for 14 patients to return to work and 25 weeks to sport (range, 21 to 27) (Table 1).
Detail of the patients reviewed for the follow up and result
DISCUSSION
To prevent rerupture, Masaaki 5 recommended a combined open and percutaneous technique to repair the Achilles tendon and to restore the original length of the tendon. Yet his method may not provide adequate tensile strength for early postoperative functional rehabilitation. Treatment results are determined not only by the method of repair but also by early postoperative functional rehabilitation. 8 Our method was able to achieve satisfactory contact of the tendon stumps, restore the original length of the tendon and gain great tensile strength by using a Bunnel-type suture. In addition, early postoperative functional rehabilitation was possible, and reruptures were not found in our study. Some cases of sural nerve injury have been reported when the percutaneous method has been employed. 2,9 Webb 12 advised that percutaneous sutures should be placed on the posterior part of the Achilles tendon and not on the lateral half of the Achilles tendon. In our method of repair, sural nerve injuries were not found.
Our technique had no wound healing problems. Adhesion of the scar on the underlying tendon is quite common after open repair in Nistor's series, 7 as this occurred in 45% of cases, but it is rarely seen after limited open repair. Contrary to Strickland's 10 report that Bunnel-type sutures produce an accordion effect with strangulation of the tendon, this accordion effect was eliminated by this technique.