
Abstract
A prospective case-control study was performed comparing axial and coronal CT scan images of 11 patients (14 ankles) with chronic lateral instability and 12 controls. Scans were performed in a standardized fashion to simulate weight-bearing. Nine measurements to evaluate the alignment of the hindfoot and forefoot were made on two occasions by two observers. The blinded images were read in order of assigned random number. The angle between the calcaneus and the vertical plane showed a statistically significant difference between patients (6.4 +/- 4° varus from vertical) and controls (2.7 +/- 5°) using unpaired ANOVA (p < 0.01). Intra-observer (R2 = 0.49 +/-0.19) and interobserver (R2 = 0. 71 +/- 0.13) variation showed moderate reliability across all measurements. This study demonstrates a method to evaluate hindfoot varus on CT scan. Many factors have been studied (e.g., proprioception) as the cause for recurrent instability, and this is the first time, to our knowledge, that an anatomic cause has been demonstrated. Although calcaneal osteotomy is clearly not indicated routinely, it may have a role in correcting extreme varus, which may contribute to failed ligament reconstruction in patients with ankle instability.
INTRODUCTION
Lateral ankle instability is a common problem seen by sports medicine physicians and orthopaedic surgeons. The vast majority of these patients are best treated without surgery. There is, however, a group of patients (approximately 20%) 5 who develop chronic and/or recurrent instability for whom surgical stabilization may be appropriate. Many theories exist regarding the underlying cause of chronic lateral ankle instability, including proprioceptive deficits, muscular weakness, and residual ligament laxity. 11,19 There are numerous procedures described to stabilize the chronically unstable ankle; 2,3,5,7,10,12,13,21 however, all of these procedures are meant to reconstruct the damaged ligaments, without addressing the underlying cause of the chronic instability.
The normal valgus alignment of the heel relative to the tibia theoretically protects the ankle and subtalar joints from excessive inversion stress. The hindfoot inversion just prior to toe-off likely makes the ankle more susceptible to instability at this point in the gait cycle. It has been suggested that patients with chronic, recurrent instability may have relatively more varus malalignment of the hindfoot, which predisposes them to lateral ankle instability. 5
Accurate measurement of hindfoot alignment remains elusive. We believe that clinical evaluation of hindfoot alignment is inaccurate, and we are aware of only one paper in the literature assessing the measurement of hindfoot varus using radiography. 18 A reliable, accurate, and reproducible measure of hindfoot alignment is needed. We believe that computerized tomography (CT) is the best imaging modality to evaluate hindfoot alignment in that it gives accurate and detailed information in the coronal plane. The purpose of this study is to determine the radiological differences with respect to hindfoot varus/valgus alignment seen on CT scan between a group of patients with chronic ankle instability and normal controls.
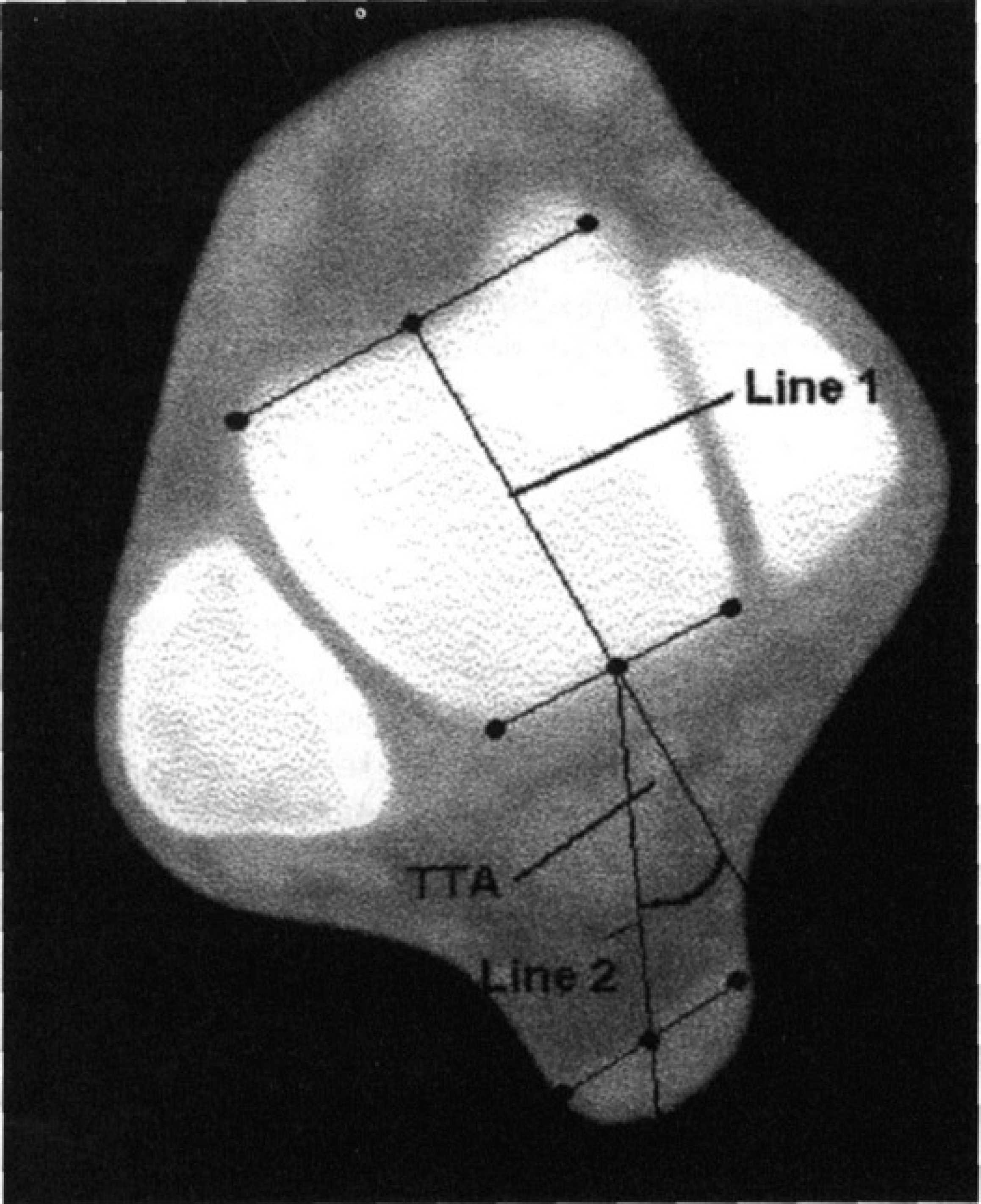
Axial image at level of superior dome of talus
MATERIALS AND METHODS
Subjects
Patients were recruited from the practice of an orthopaedic foot and ankle surgeon (A.Y.) after having been referred with a chief complaint of chronic or recurrent lateral ankle instability. Patients were included if they had at least three episodes of lateral ankle sprain or instability with ongoing symptoms for at least six months. Patients were excluded if:
they had prior surgery of the affected ankle/hindfoot;
they had a history of fracture of the hindfoot; or
they were younger than 16 years of age.
All patients were examined and a detailed history was taken. Patients were included only if a final diagnosis of lateral ankle instability was made.
Control subjects were recruited via poster from the general population. Exclusion criteria included:
a positive history of ankle/hindfoot fracture or sprain;
prior hindfoot surgery; and
age less than 16.
Control subjects were age- and sex-matched to patients in the study with ankle instability.
Twelve patients and 12 controls participated in the study. There were 10 males and two females in both the patient and control groups, with an age range from 27 to 60 for patients and 26 to 48 for controls. All study participants were fully informed of the purpose of the study and any risks associated with the CT scanning. Each subject signed an informed consent form approved by the hospital's ethics committee prior to participation. A modest stipend was paid to each control subject for participating in the study.
After the scans were reviewed, one control subject was found to have obviously deformed feet and congenital foot abnormalities despite a screening questionnaire. This subject was replaced by another recruited control. One study patient was excluded after review of the CT scan confirmed syndesmosis widening and arthritis of the ankle, leaving 11 patients in the study. As there were three patients with bilateral instability, a total of 14 ankles were studied as subjects, with 14 ankles matched as controls in the paired analysis.
Imaging Technique
All participants in the study had CT scans performed on both lower extremities in a standardized fashion using the same technician and scanner for each subject. A helical CT scanner was utilized with axial and coronal plane images taken at 3 mm intervals with both feet resting against a foot-plate and the heels together, as described by Martinez 16 and Seltzer. 20 A footrest was utilized to simulate weight-bearing conditions, and to align the ankle joint in a neutral position.
Axial images were obtained from the distal tibial diaphysis to the inferior aspect of the calcaneus. Coronal images were obtained from the calcaneal tuberosity to the level of the 1st tarsometatarsal joint.
Measurements
A number of measurements that we felt would best represent hindfoot varus/valgus alignment were determined, and applied to each of the subjects. The first measurement was made on the axial image at the level of the ankle joint (Fig. 1). The angle formed between the long axis of the dome of the talus (Fig. 1, line 1) and a line bisecting the posterior dome of the talus and the Achilles tendon (Fig. 1, line 2) was termed the Talus-TendoAchilles Angle, or TTA. A decrease in this value was felt to reflect greater hindfoot varus as the Achilles tendon moved closer to the midline.
The second measurement was made from axial images comparing the long axis of the talar dome to the long axis of the calcaneus (Figs. 1, 2). An angle was obtained comparing each axis (Fig. 1, line 1; Fig. 2, line 3) against a line across the posterior aspect of each Achilles tendon. Using the posterior reference marker on the scanner it was possible to transcribe the axis from one image to the other image. The difference between these two angles was then calculated to give an angle called the Talo-Calcaneal Angle (TCA). A greater angle we believe reflects a greater degree of varus and/or cavus of the hindfoot.
The third and fourth measurements reflected the alignment of the long axis of the calcaneus in relation to other anatomical points in the hindfoot and midfoot. The third angle, called the Calcaneal-Cuboid angle (CCA), measured the angle formed from the long axis of the calcaneus (Fig. 2, line 3) vs. a line across the two most posterior points along the cuboid articular surface (Fig. 2, line 5). An increase in this angle was felt to represent increased hindfoot varus. The fourth angle measured was that between the long axis of the calcaneus (Fig. 2, line 3) and a line from the midpoint of the posterior surface of the calcaneus to the midpoint of the 1st metatarsal head (Fig. 2, line 4). This angle was termed the Calcaneal Metatarsal Angle (CMA). An increased value was felt to reflect an increase in cavus/ adduction of the forefoot.
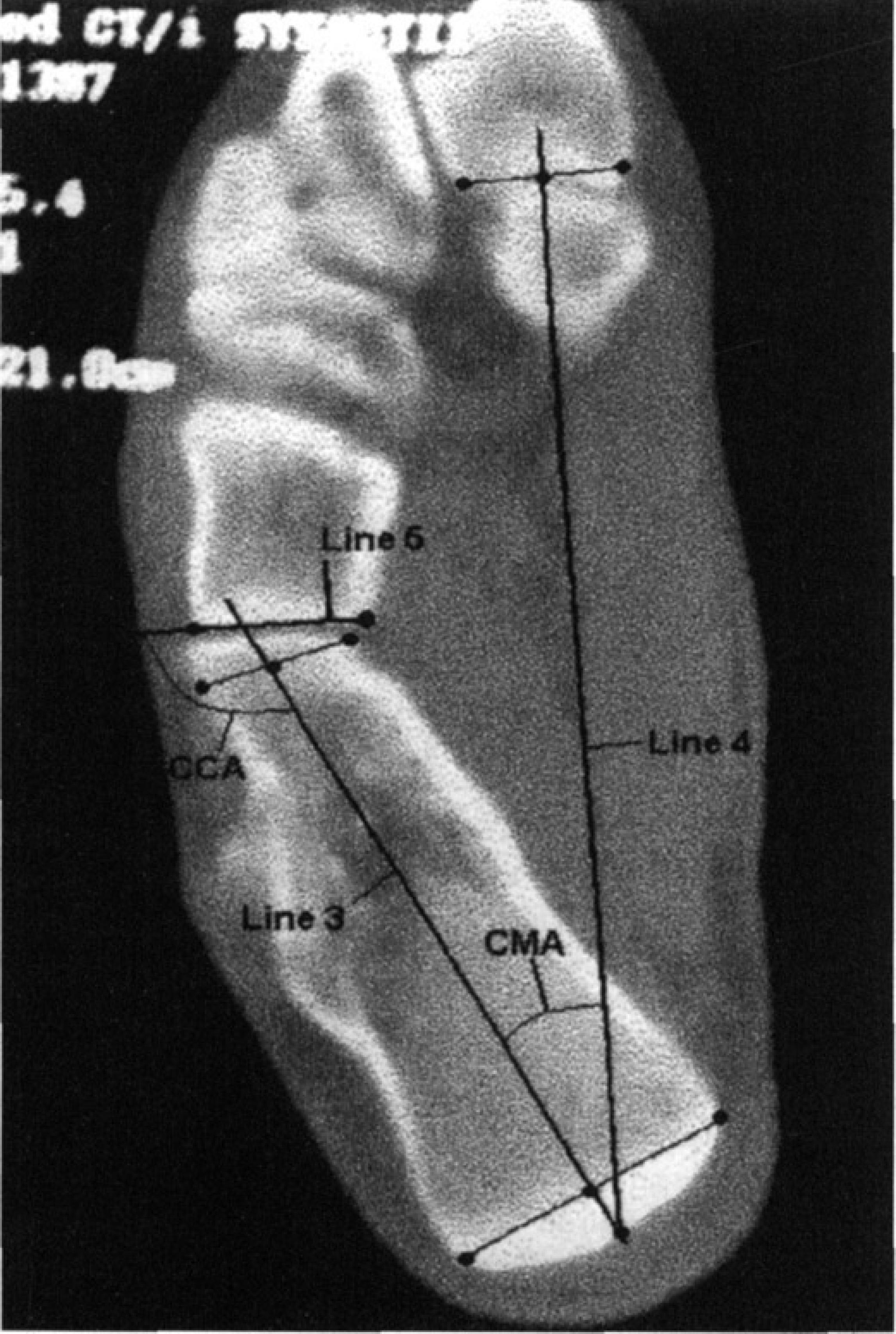
Axial image of calcaneal long axis.
The final measurements were obtained from coronal images at the posterior aspect of the subtalar joint and the calcaneal tuberosity (Fig. 3). Two measurements assessing the varus alignment of the calcaneus were determined. Each of these measured the long axis of the calcaneus against the horizontal, the first measuring along the medial wall of the calcaneus (Fig. 3, line 7)—the Medial Calcaneal Varus Angle (MCVA)—and the second using the central axis (Fig. 3, line 6)—the Central Calcaneal Varus Angle (CCVA). Increased values were thought to reflect increased hindfoot varus.
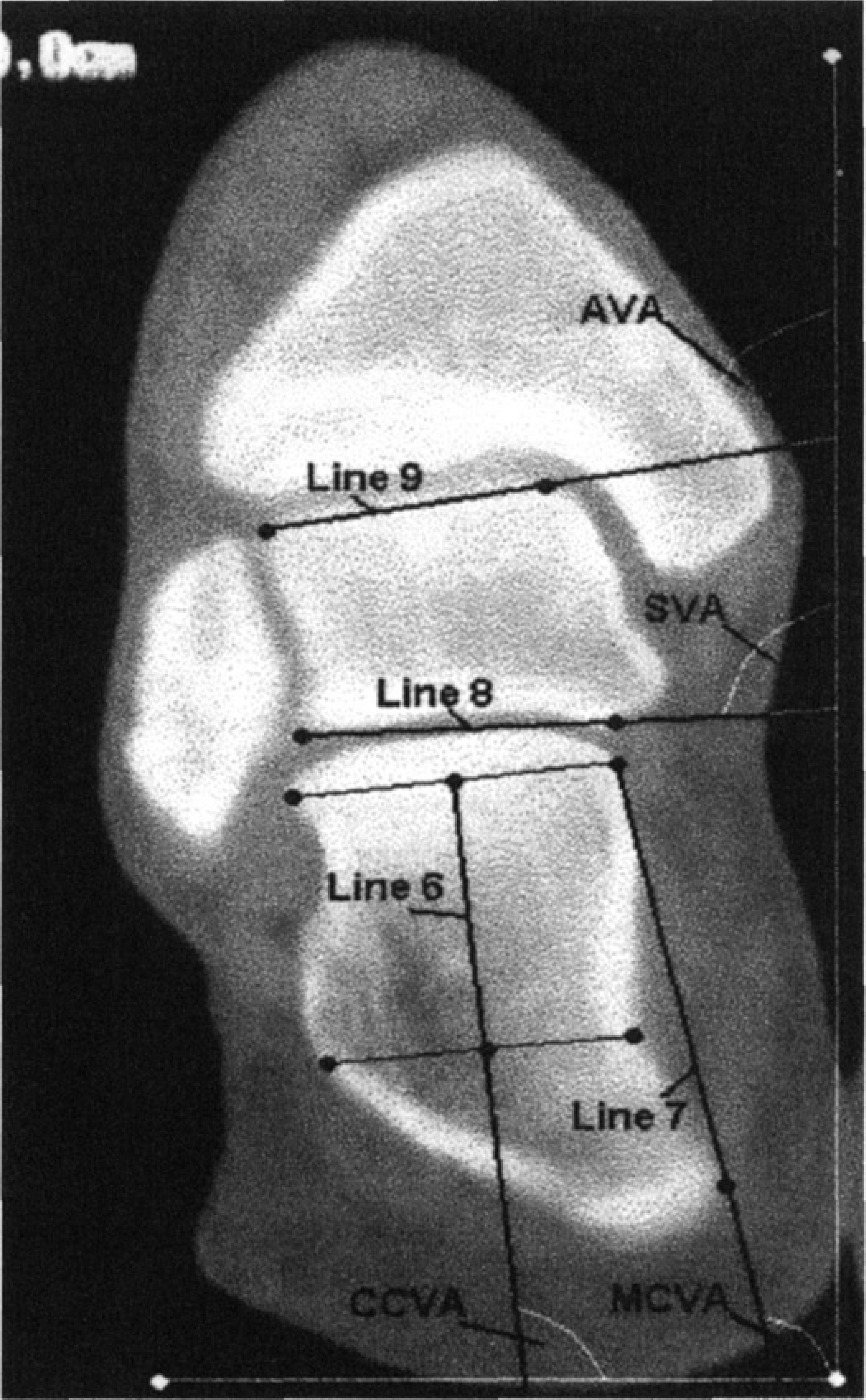
Coronal image of calcaneal vertical axis (note: the white lines represent the measured vertical and horizontal axes).
The seventh angle was formed comparing a line across the posterior facet of the subtalar joint (Fig. 3, line 8) with the vertical—the Subtalar Vertical Angle (SVA). The eighth angle compared the superior aspect of the talar dome (Fig. 3, line 9) against the vertical—the Ankle Vertical Angle (AVA). The two angles were then subtracted to produce a ninth measurement, the lateral slope, or shape, of the talus. This was termed the Talar Slope (TS). Increased values for the SVA and the AVA were felt to reflect increased hindfoot varus at the level of the subtalar and ankle joints respectively. A decrease in the difference between the two—or decreased Talar Slope (TS)—was felt to reflect increased overall hindfoot varus.
Inter- and intra-observer reliability
Two observers read the images on two occasions to determine the inter- and intra-observer reliability of the measurements. Four copies of the images were made with all identification marks removed. The images were assigned random numbers and read in order. Repeat randomization was performed for the second reading. The observers were trained in the technique for reading the measurements prior to commencement of the study.
ANALYSIS
The reliability measurements were analyzed using regression analysis and the intra and inter observer reliability for each measurement determined and quoted as an R 2 value. Analysis was performed for both paired and unpaired data.
Paired
Statistical analysis was performed using paired analysis of variance (ANOVA) for each measurement with the patients age- and sex-matched to corresponding controls. As there was 14 symptomatic ankles in the study group, there were 14 paired analyses performed.
Overall R 2 values for all measurements
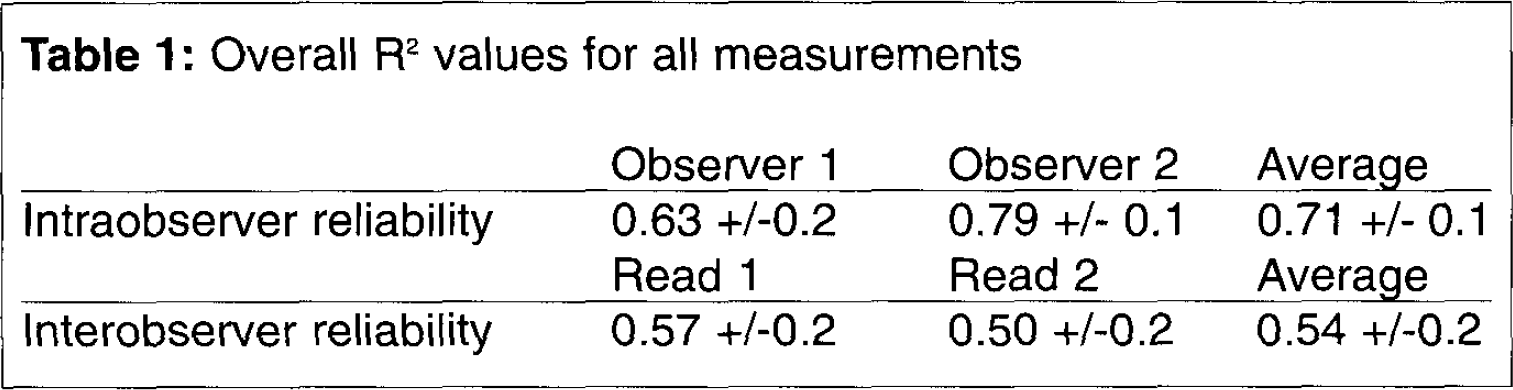
Mean R 2 values for each of the nine measurements (both patients and controls).
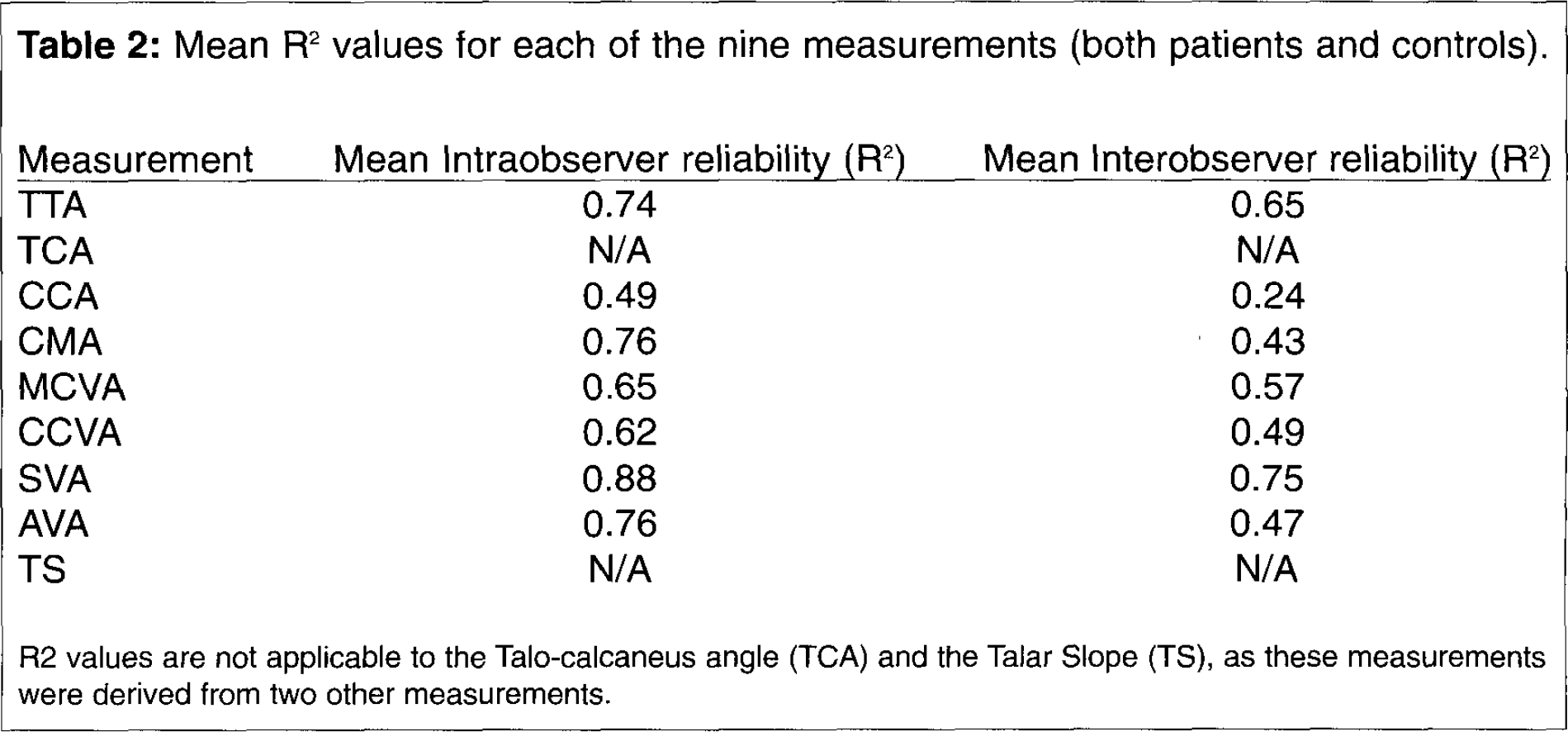
R2 values are not applicable to the Talo-calcaneus angle (TCA) and the Talar Slope (TS), as these measurements were derived from two other measurements.
Unpaired
Unpaired statistical testing using the values for both ankles of all the patients in the study group (22 ankles in 11 patients) versus all the values for the control group (24 ankles in 12 subjects) was performed using unpaired ANOVA. Although patients may have been symptomatic in only one ankle, true anatomic differences in hindfoot alignment would be seen in both ankles. Therefore, unpaired analysis comparing all the values for patients in the study group with all the values for the control group was performed.
As at least five different measurements were compared, p was considered significant at < 0.01.
RESULTS
Reliability data for all measurements combined and for each individual measurement is shown in Tables 1 and 2.
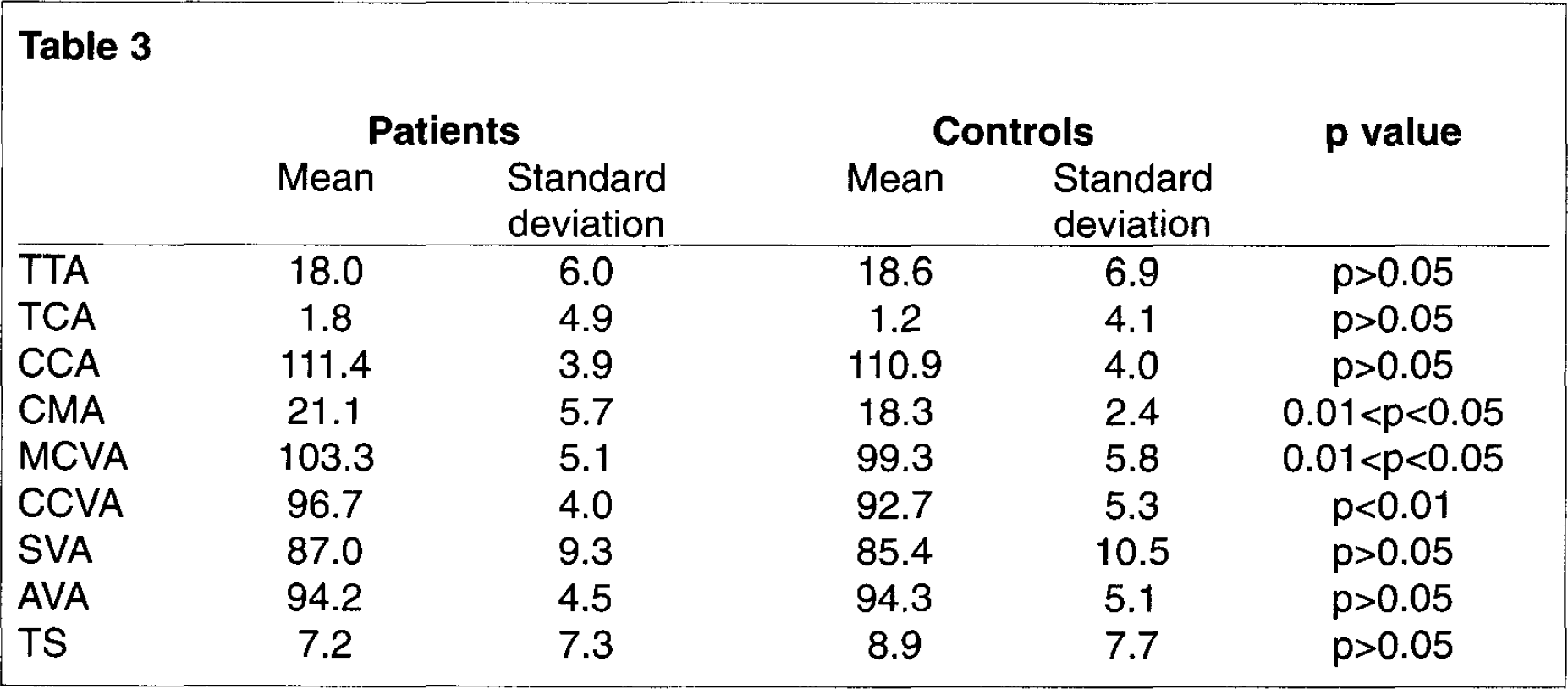
Unpaired Data
22 ankles in 11 patients and 24 ankles in 12 controls were scanned and included in the analysis. Table 3 shows the mean values and standard deviations for each of the nine measurements for both patients and controls. A statistically significant difference was seen in the CCVA, with an increased value demonstrating increased varus of the hindfoot.
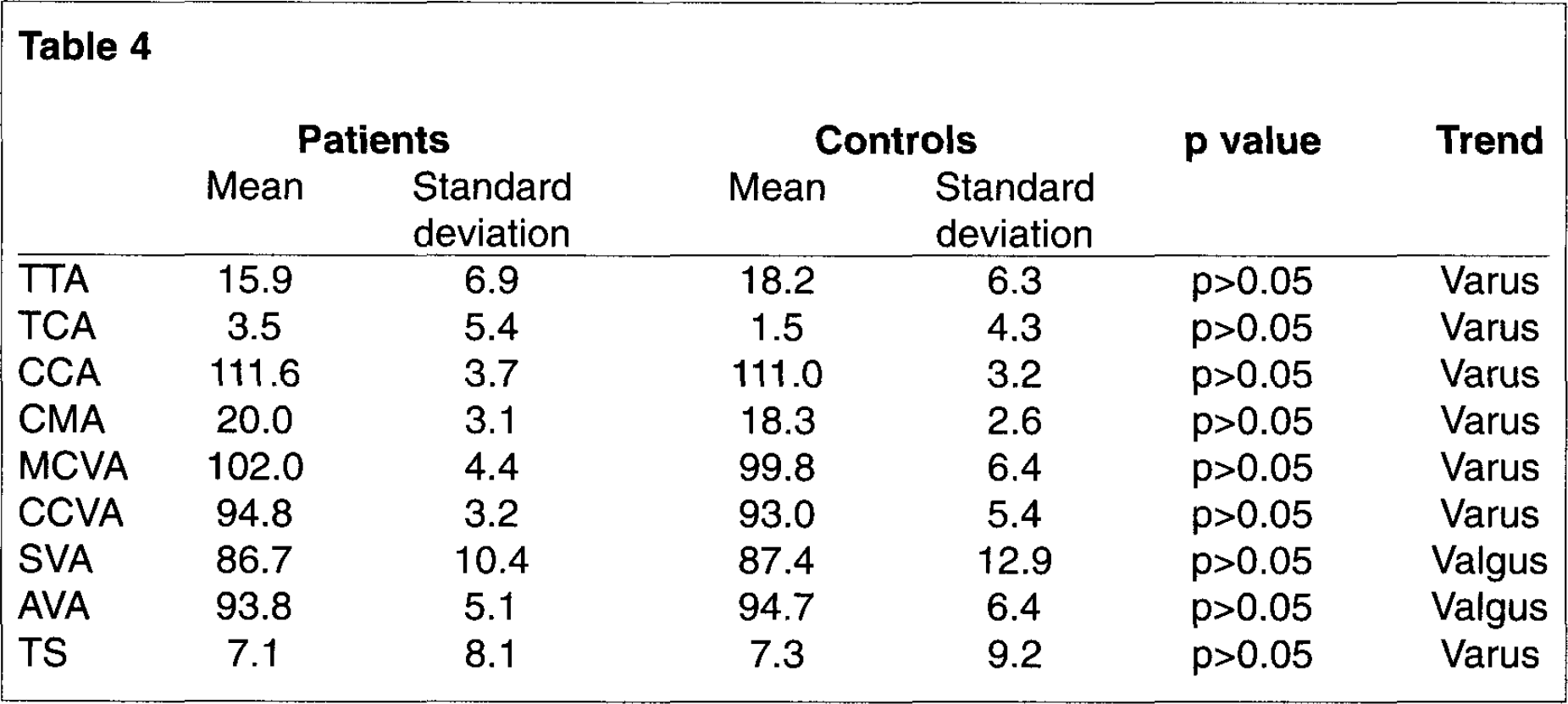
Paired Data
All values studied for paired ANOVA failed to show a statistically significant difference between patients and controls. There was, however, a trend towards increased varus (i.e., a greater value) in all measurements except the SVA and the AVA. The results are shown in Table 4.
DISCUSSION
Factors that predispose an individual to chronic lateral ankle instability are not well described in the literature. Colville states that “ligament reconstruction in patients with an unstable ankle and a varus hindfoot may fail due to severe inversion forces created by mechanical malalignment.” 5 He suggests that calcaneal osteotomy to correct the varus may be required in these patients. Based upon our observations, patients with chronic lateral instability seem to have relatively more varus malalignment of the hindfoot than patients without lateral instability. Our goal in this study was to determine an accurate and reproducible measure of hindfoot alignment and determine if a sample of patients with chronic instability had more varus than controls.
There are few references in the literature dedicated to techniques of hindfoot varus/valgus measurement. Clinical measurement of hindfoot using goniometers has been reported, 1 but other authors have pointed out the unreliable nature of this measurement technique. 19 Plain films have been utilized to determine hindfoot alignment. There are a number of radiological references to a diagnosis of instability using stress views (talar tilt and anterior drawer sign). 5,6,14 A recent paper by Saltzman, 18 utilizing a modification of the technique described by Cobey, 4 described the normative data for hindfoot alignment based upon radiography of the hindfoot in a group of healthy volunteers. This paper established a reproducible and reliable method for evaluating hindfoot alignment. There are certain inherent errors in this technique that were acknowledged by Saltzman. These include the fact that plain radiography cannot overcome the overlap of various soft tissue and bony structures leading to decreased detail. In addition, external rotation of the tibia will lead to an appearance of increased varus on plain X-ray. Saltzman controlled for this by measuring and standardizing the amount of tibial rotation. 18 The technique provides a true weight-bearing view, as opposed to CT measurements that cannot be weight-bearing due to limitations of the gantry. Although the technique of Cobey has been used for many years and has been shown to be reproducible, test-retest reliability has not been demonstrated for this or the CT scan technique.
According to Martinez 16 the detail and accuracy of computed tomography provides the best method for evaluating hindfoot pathology and alignment. We agree with this view; however, the literature is very scant with respect to measuring hindfoot alignment using computed tomography. The only reported series is that of Seltzer, et al. in which the “heel valgus angle,” among other measurements, was calculated for 17 patients and 10 controls. 20 This angle was measured between the estimated long axis of the tibia and the long axis of the calcaneus on coronal image at the level of the posterior facet of the sub-talar joint. This technique has obvious advantages over the plain radiography of Saltzman, in that overlap is eliminated and the effects of rotation can be controlled. However, an obvious disadvantage of the CT technique is the fact that subjects are not weight-bearing (only “simulated”), and that the gantry of the scanner does not allow an adequate length of the tibia to be imaged for accurate estimation of its true long axis.
Due to these inherent flaws, we felt that different measurements comparing the intrinsic alignment of the tarsal bones and their relationships to the tibia and to each other were needed. The measurements we have outlined above have reasonable reliability within and between observers, are reproducible, and do not depend on the long axis of the tibia to determine relative varus of the hindfoot. This is particularly advantageous for use in coronal CT scans in which the true long axis of the tibia cannot be visualized.
Although the number of subjects in the study was small, a statistically significant difference between patients and controls was demonstrated for the CCVA at a relatively stringent p value of <0.01. This suggests that hindfoot varus is more common in patients with chronic lateral ankle instability compared with normal controls. Interestingly, this measurement was similar to that reported by Seltzer, et al. (“the heel valgus angle”). 20 Although the CCVA was not the most reliable measurement among the nine values we calculated, a statistically significant result was still seen, suggesting that true varus alignment does exist.
Our other measurements did not reach statistical significance at p < 0.01; however, there was a trend towards increased hindfoot varus in the patient group for each of the measurements except the AVA and the SVA (Table 3, 4). The fact that paired data failed to show a significant difference suggests that more numbers would be required to demonstrate a difference.
Colville has stated that a calcaneal osteotomy may be required for patients with chronic lateral ankle instability and hindfoot varus alignment in order to prevent the ligament reconstruction from failing due to mechanical malalignment. 5 We are not aware of any clinical studies assessing the role that calcaneal osteotomy may play in the treatment of this condition, nor are there studies comparing outcome after ligament reconstruction with or without calcaneal valgus osteotomy. Our results support the notion that hindfoot varus malalignment is more prevalent in patients with ankle instability compared with controls, and lends credence to the theoretical advantage of correcting hindfoot varus with an osteotomy in addition to reconstructing the damaged ligaments in the treatment of chronic lateral ankle instability. Nonetheless, until further clinical studies support the role of calcaneal osteotomy in this population, we feel that this procedure is experimental for this condition, and should be reserved for patients known to have excessive hindfoot varus on CT scan or Cobey views.