
Abstract
The Flexor Hallucis Syndrome has been associated with ballet and sports activities. It has been thought to represent over use with attendant tenosynovitis of the tendon in the fibro-osseous tunnel extending from the ankle to the midfoot. We report a patient with an accessory flexor digitorum longus who presented with classical clinical features of the syndrome. The patient's disabling symptoms persisted despite a year and a half of nonoperative treatment. They were finally relieved when the accessory muscle was excised. In addition to the previously described clinical features of the Flexor Hallucis Syndrome, the physical exam included abnormal fullness between the Achilles tendon and the tibia. When the ankle was held in dorsiflexion, there was limited dorsiflexion of the lateral toes, which were tethered by the “cork-in-a-bottle” effect of the distal muscle mass of the accessory flexor digitorum longus muscle at the flexor retinaculum and fibro-osseous canal of the flexor hallucis longus. The MRI examination confirmed the presence of an abnormal muscle mass extending distal to the ankle joint with the foot in neutral. The study also demonstrated fluid in the ankle joint and fibro-osseous canal of the flexor hallucis, and marrow edema within the body of the talus consistent with chronic inflammation. Follow-up MRI six months after excision of the muscle revealed some scar formation at the site of the previously excised muscle and complete resolution of the joint effusion, fluid in the tunnel of the flexor hallucis, and marrow edema.
INTRODUCTION
The accessory flexor digitorum longus (AFDL) of the foot is found in up to 8% of lower extremities. The anatomy of this anomalous muscle is variable in both origin and location of the musculotendinous unit in relation to the flexor hallucis longus. 2,3,5,8,22,23,29,33 This accessory muscle had not usually been considered a source of symptoms or functional impairment, although Nathan 22 speculated that it might be a cause of tarsal tunnel syndrome because of the anatomy. More recently, Sammarco described several patients in whom the accessory muscle was thought to be a cause of tarsal tunnel syndrome. 27 We describe a patient in whom the accessory flexor digitorum longus was the apparent cause of symptoms of the Flexor Hallucis Syndrome.
CASE Report
The patient was a 15-year-old female with a history of one and one-half years of pain in the posterior medial aspect of her left ankle radiating into the medial aspect of the forefoot. She related the onset of her symptoms to an event while playing soccer when her left foot was acutely dorsiflexed and everted. She was initially treated by her family physician for foot strain with rest and guarded weight-bearing. Because of persistent pain and inability to play soccer, she received several referrals for evaluation and treatment which included an orthosis, physical therapy modalities, rest, and cast application, all without benefit. She denied any snapping or locking of the foot or toes and had no foot paresthesias or other sensory complaints. Her pain when walking normally was less severe, although still bothersome.
On physical exam she was noted to have minor swelling and tenderness in the posterior medial aspect of the left ankle. There were no superficial signs of inflammation. There was a fullness in the interval between the Achilles tendon and the tibia greater than one usually sees in this region. This fullness was also present in the contralateral asymptomatic limb. There was tenderness along the flexor hallucis as it passed beneath the sustentaculum of the talus. She experienced acute pain with dorsiflexion of the foot and then dorsiflexion of the great toe. There was limited dorsiflexion of the lateral four toes in both feet with the ankles in slight dorsiflexion. Toe motion was normal when the ankles were placed in plantarflexion. Maximal plantarflexion of the foot did not produce any subjective complaints. There was no pain beneath the first metatarsal head. There was no sign of any triggering of the foot or toes.
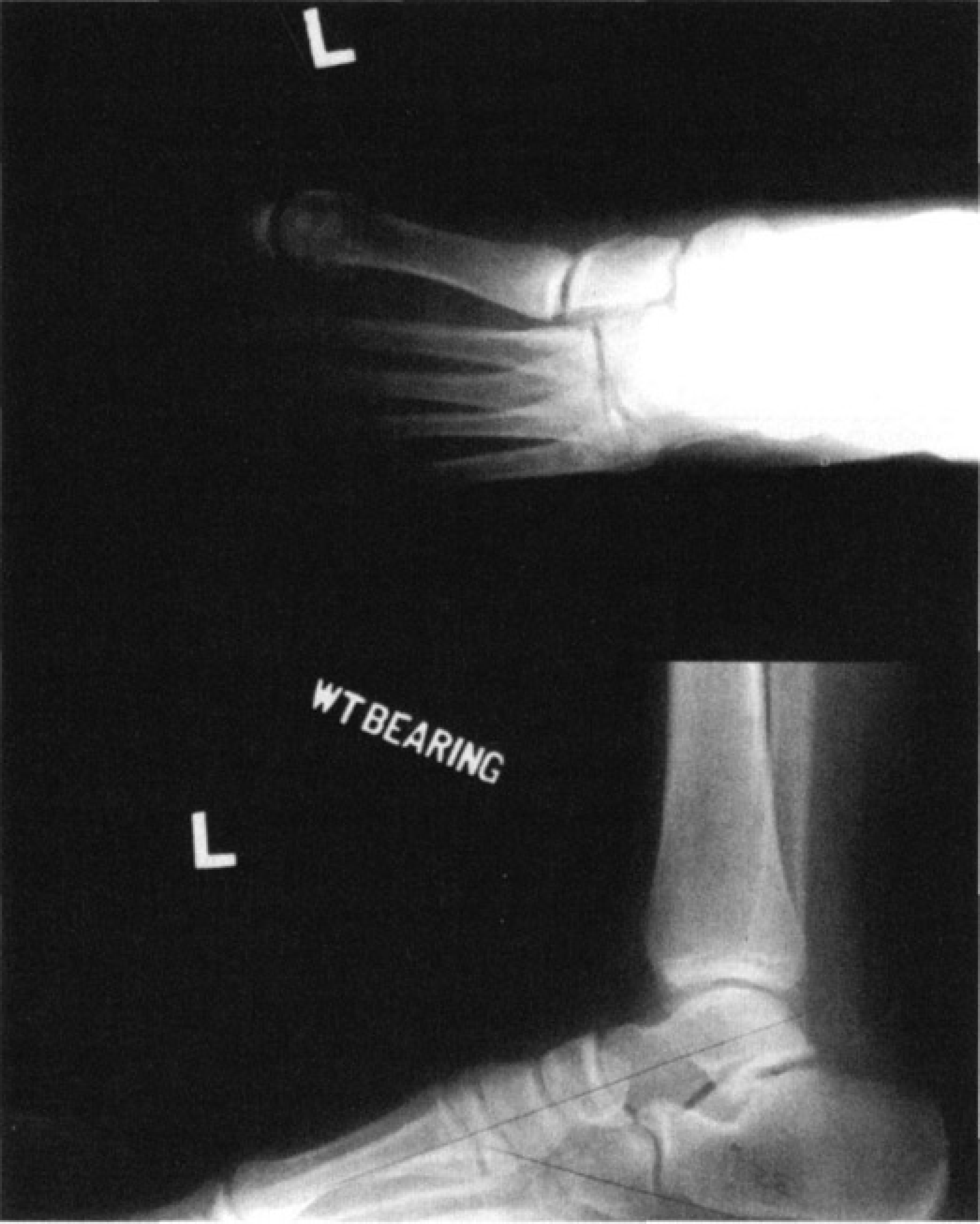
Films of left foot pre-op demonstrating bipartite seamed.
Her X-rays were normal except for a bipartite seamed on the left (Fig. 1). There was no ossification in the region where one would expect to see an os trigonum. There was no separation of the bipartite sesamoid with acute dorsiflexion of the great toe, and the bone scan was negative.

MRI demonstrating marrow edema in the talus and fluid in the flexor hallucis sheath and ankle joint.
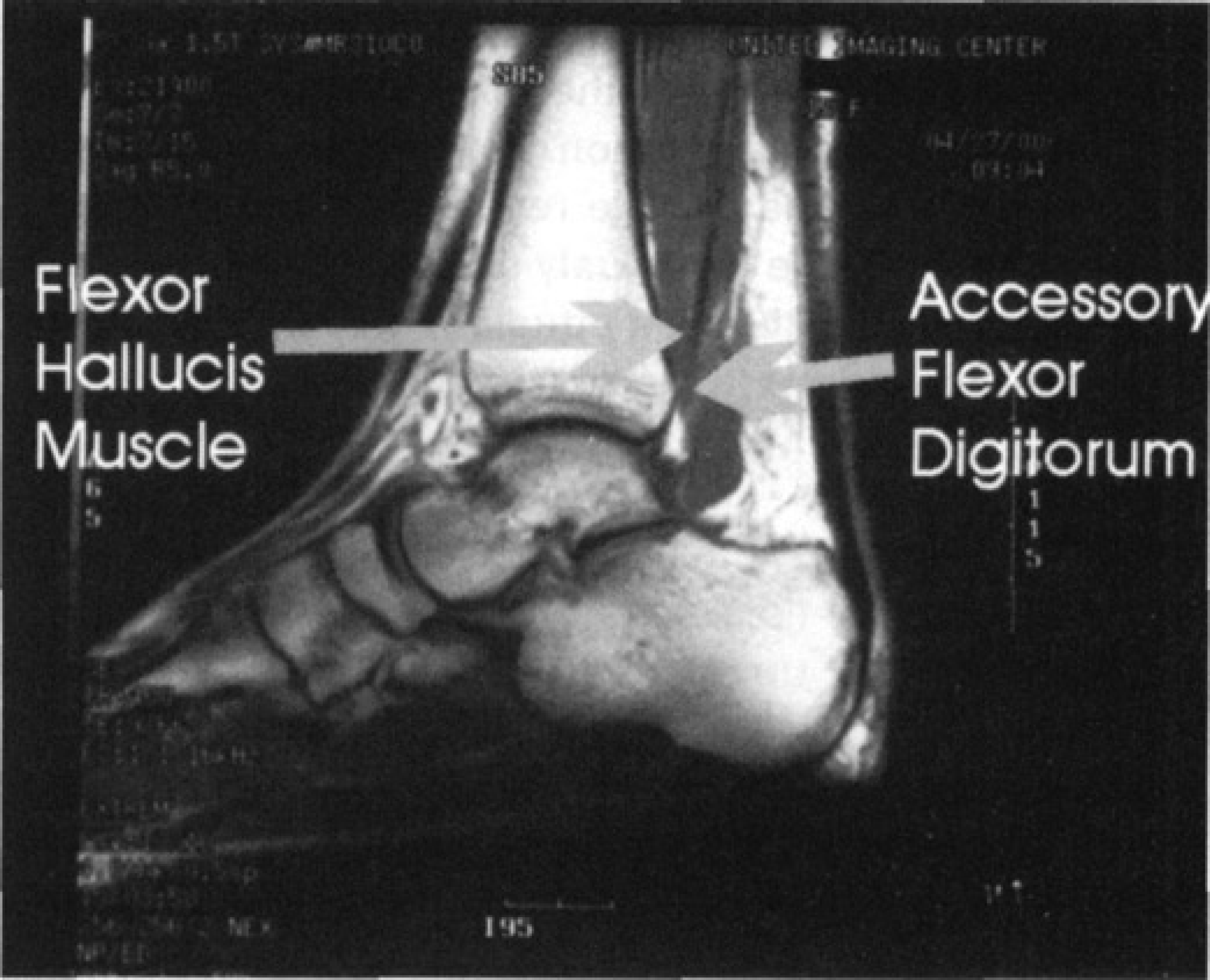
MRI demonstrating abnormal muscle posterior and lateral and distal to the flexor hallucis longus.
We prescribed continued rest, ice, and non-steroidal anti-inflammatories for pain. Because of the failure of these and other nonsurgical measures to relieve her symptoms, we obtained an MRI scan. This demonstrated extensive signal abnormality involving the talus. There was a small ankle joint effusion with some fluid present in the sheath of the flexor hallucis longus (Fig. 2). An abnormal muscle was present superficial and lateral to the flexor hallucis muscle and tendon which extended more distally than the flexor hallucis (Fig. 3–4). This muscle was thought to represent either an abnormality of the flexor hallucis or an accessory flexor digitorum communis (longus). In view of the positive findings on MRI and the persistence of her disabling symptoms despite extensive nonoperative management, we recommended surgical exploration of the posterior medial ankle.
At the time of surgery it was noted that she did have an accessory flexor digitorum communis which passed beneath the flexor retinaculum with the flexor hallucis tendon and into the fibro-osseous tunnel of the flexor hallucis longus (Fig. 5). The accessory muscle mass was quite large at the level of the ankle and distal to where the flexor hallucis becomes tendon. When one pulled on it, the lateral toes flexed. When the foot was dorsiflexed, we were able to observe the accessory muscle mass pulled into the fibro-osseous tunnel of the flexor hallucis like a cork into a bottle, and further dorsiflexion of the toes was limited by this tether effect. The flexor hallucis tendon itself was intact, but its color was yellowish and there appeared to be mild degenerative changes in the paratenon and strands of tissue in the sheath. The anatomically normal flexor digitorum communis was tested, and it was normal. The accessory flexor digitorum muscle was then excised to include its tendon as distally as possible through a posterior medial incision (Fig. 6). The flexor retinaculum and sheath of the flexor hallucis were partially excised approximately two centimeters towards the sustentaculum. The origin of the anomalous muscle was from the fascia between the tibia and fibula and from the posterior aspect of the tibia itself. There was no separate sheath for the tendon of the accessory muscle, as it was immediately adjacent and lateral to the flexor hallucis longus.
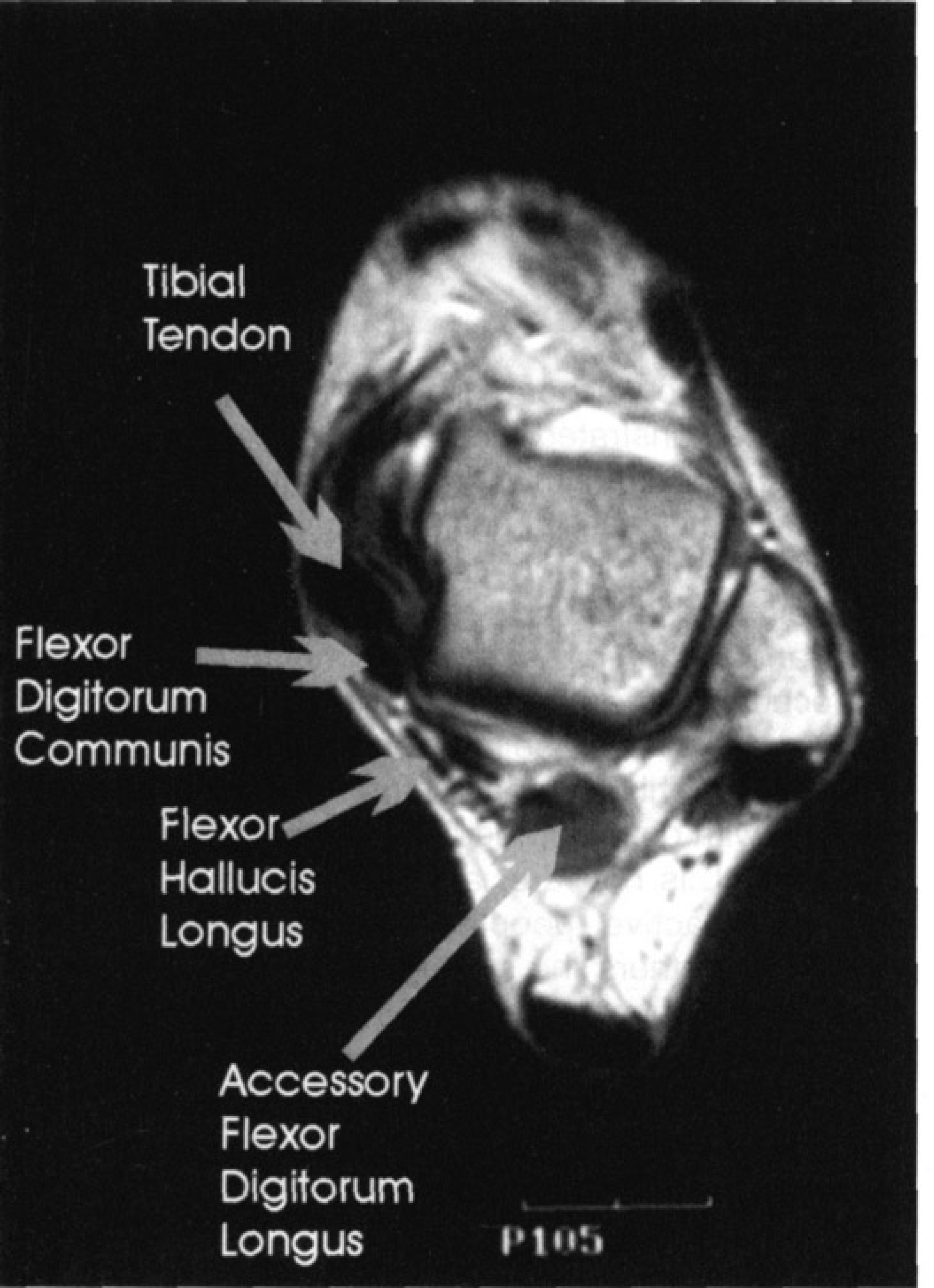
Axial section on MRI demonstrating the distal and lateral position of the accessory flexor digitorum longus.
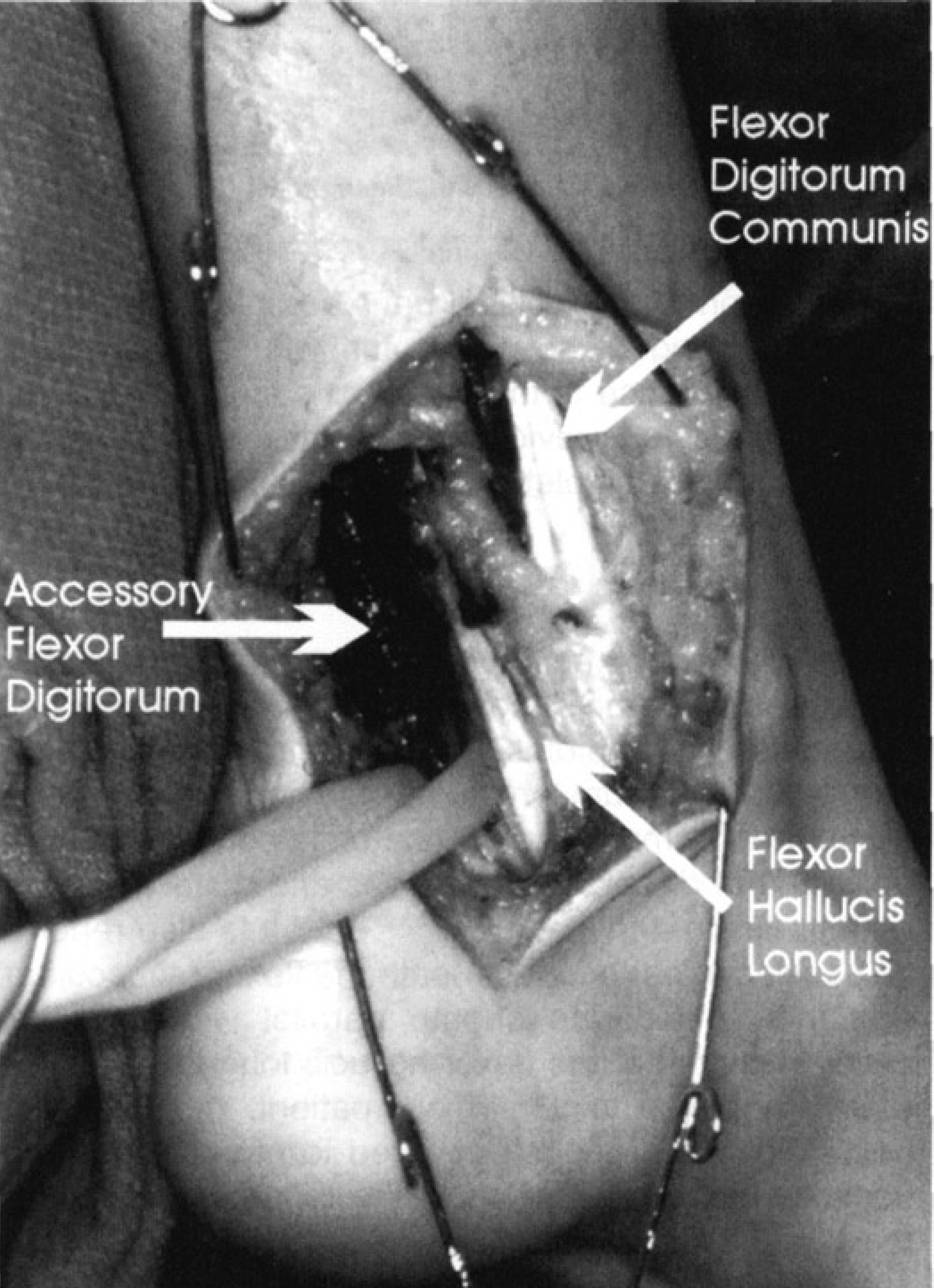
Surgical exposure of the ankle demonstrating the distal muscle mass of the accessory flexor digitorum longus.
After surgery, the patient was protected with a short leg cast for wound healing for 10 days and then allowed to start ankle motion. She was non-weight-bearing for a period of about six weeks, during which time she regained much of her normal ankle motion. Her pain was completely gone after four weeks, and when she began weight-bearing at six weeks she remained asymptomatic. During the course of the next several months, she reported that her symptoms were completely resolved, although she had not participated in any competitive athletics. When she finally did return to competitive soccer, she developed posterior ankle pain in the region of the incision but was able to participate fully, managing these symptoms with Motrin.® There was no recurrence of the disabling pain which she had been treated for previously, and after soccer season she again was completely asymptomatic.

The excised accessory flexor digitorum longus.
DISCUSSION
Previous reports have pointed out the anomalous distal extension of the flexor hallucis longus muscle belly as a cause of symptoms at the ankle. 1,6,10,21,26 The accessory flexor digitorum longus muscle has been previously reported primarily as an anatomic curiosity found in up to 8% of dissected extremities and quite variable in both its origin and insertion. 2,3,5,22,23,29,33 It is also reported as passing into the foot beneath the flexor retinaculum 13 and into a separate sheath parallel with the fibro-osseous tunnel of the flexor hallucis longus and immediately adjacent to it. 23 In our patient, the accessory flexor digitorum longus appeared to pass into the foot beneath the same portion of the retinaculum and into the fibro-osseous tunnel as the flexor hallucis longus, and lateral to the flexor hallucis longus tendon. We have been unable to find a reference describing the accessory digitorum longus as a cause of ankle pain or flexor hallucis longus tenosynovitis. There have been two papers identifying the accessory flexor digitorum longus as the cause of tarsal tunnel syndrome. 1,2,27 At surgery it was noted that the flexor hallucis longus tendon had some mild degenerative changes but there were no findings of tears, longitudinal disruptions or nodular swelling. 1,4,7,9 –11,14 –21,24,25,28,30 –32 The tendon of the accessory flexor digitorum longus was normal in its appearance with no degenerative changes. The only inflammation was in proximal portion of the retinaculum at the ankle and at the musculotendinous junction of the accessory flexor digitorum longus. In our patient the symptoms of flexor hallucis longus tenosynovitis were completely relieved by excision of the accessory muscle, although she did have some persistent incisional pain with competitive sports. Her symptoms in the incisional area have improved with exercise and the passage of time. We demonstrated a similar accessory muscle in MRI of the opposite ankle, but there were no signs of inflammation in the study and to date she has remained asymptomatic on that side. On the side treated surgically, her range of lateral toe motion is now normal and not affected by the position of her ankle. We suspect that at the time of her injury she tore the septum between the flexor hallucis and the sheath of the anomalous flexor digitorum and that the two tendons in the same sheath probably created an adverse environment for the flexor hallucis.
CONCLUSIONS
The accessory flexor digitorum longus (AFDL) muscle can be demonstrated with an MRI scan which would reveal an abnormal muscle mass that extends distal to the ankle joint and immediately adjacent to the flexor hallucis tendon. Symptoms may be caused by impingement of the distal muscle mass under the flexor retinaculum and in the fibro-osseous tunnel of the calcaneus. A procedure to remove the impingement of the accessory muscle in our case relieved the patient's symptoms completely. This anomaly must be kept in mind in patients with posterior medial ankle pain. The presence of an AFDL is not rare, and may cause symptoms in physically active people and particularly athletes because it tethers the toes when the foot is placed in acute dorsiflexion.