
Abstract
The first known report of a patient with Lyme Disease-induced peripheral neuropathy resulting in bilaterally symmetrical “Charcot” changes of the midfoot is reported. An extensive review of the literature failed to produce any known cases of neuropathic osteoarthropathy that would be linked directly or indirectly with Lyme Disease-Induced peripheral neuropathy. The relationship between Lyme Disease, the secondary neurologic manifestations caused by the infection, and neuropathic osteoarthropathy are discussed.
Lyme Disease
Lyme Disease is the most common vector-borne infection reported in the United States. 1,2,3 The disease is caused by the spirochete Borrelia Burgdorferi which is transmitted by the deer tick Ixodes scapularis (I. dammini) and Ixodes pacificus. 4,5 Thus, the presence of Lyme Disease correlates well with local deer populations. 5 Nearly 90% of cases reported to the Centers for Disease Control and Prevention (CDC) in 1994 were from Massachusetts, Rhode Island, Connecticut, New York, New Jersey, Wisconsin, and Minnesota. 5 Although first reported in Wisconsin in 1970, the disease was not nationally recognized until 1976 in Old Lyme, Connecticut. 3,6,7 Lyme Disease affects males and females with equal frequency and has a bimodal age distribution. 4 The highest rates of infection are seen in children aged 5 to 9 years old and in adults over the age of 30. 4 Lyme Disease is manifested by a characteristic skin lesion referred to as erythema chronicum migrams (ECM) or “bull's-eye lesion” that develops within seven to 10 days after a bite from an infected tick. 1,4,5
Like its counterpart syphilis, Lyme Disease causes multisystem disease affecting the skin, nervous system, heart, and musculoskeletal system. 2,5,8 Some studies suggest that different clinical manifestations appear as a result of different strains of the spirochete with neurological disorders being caused by B. burgdorferi sensu lato and B. burgdorferi sensu stricto. 8 Generally, Lyme Disease has been classified into three clinically overlapping stages. 1,2,5,6,8 In the first stage the characteristic ECM lesion appears. However, only about one-fourth of infected persons are diagnosed, as most are unaware they have been bitten. 6 This may be attributed to only one fourth of infected persons ever recalling being bitten in the first place. 1 A review of 200 consecutive patients by Berger, showed that 76% of lesions were seen on either the trunk or lower extremity. 2 In stage II the disease is manifested by neurological and/or cardiac abnormalities that may develop weeks to months after onset of the ECM lesion. 6 Stage III causes the development of rheumatological manifestations and may occur anywhere from several weeks to many years after the initial infection. 6 These multiple overlapping stages have led to the referencing of Lyme Disease as the “great imitator” by primary care physicians. 6 The neurological components of Lyme Disease can occur alone or in combination resulting in Bell's palsy, peripheral neuropathies (mononeuritis multiplex, radiculoneuritis, or diffuse peripheral neuropathy), radiculopathies, myelopathies, encephalitides, meningitides, Guillain-Barré-like demyelinating neuropathy, chorea, cerebellar ataxia, and pain syndromes. 1,2,5,6 Neurological abnormalities often present as a characteristic triad of cranial nerve palsies, meningitis, and peripheral radiculoneu-ropathy. 5 Some reports have indicated that if left untreated, neurological manifestations of Lyme Disease will develop in 15% to 20% of those infected. Evidence suggests that this nervous system involvement is a result of a direct invasion by the spirochete and not so much related to the patient's immune response to it. 9 A recent study of over 100 patients during a two-year period by Halperin et al., showed an average age of 40 5 years with an average duration of symptomatic Lyme Disease of 30 months. The study also showed that the presence of neurophysiologically demonstrable neuropathy correlated strongly (p<0.0005) with the presence of intermittent limb paresthesias and that the presence of significant peripheral nerve abnormalities exist in 40% to 50% of patients with late disease. 9 These findings show that often times when a clinical diagnosis of peripheral nerve pathology cannot be made, an underlying etiology often exists. Most studies agree that if antibiotic treatment is properly introduced in a timely manner, most nervous system abnormalities are readily reversible. 4,9
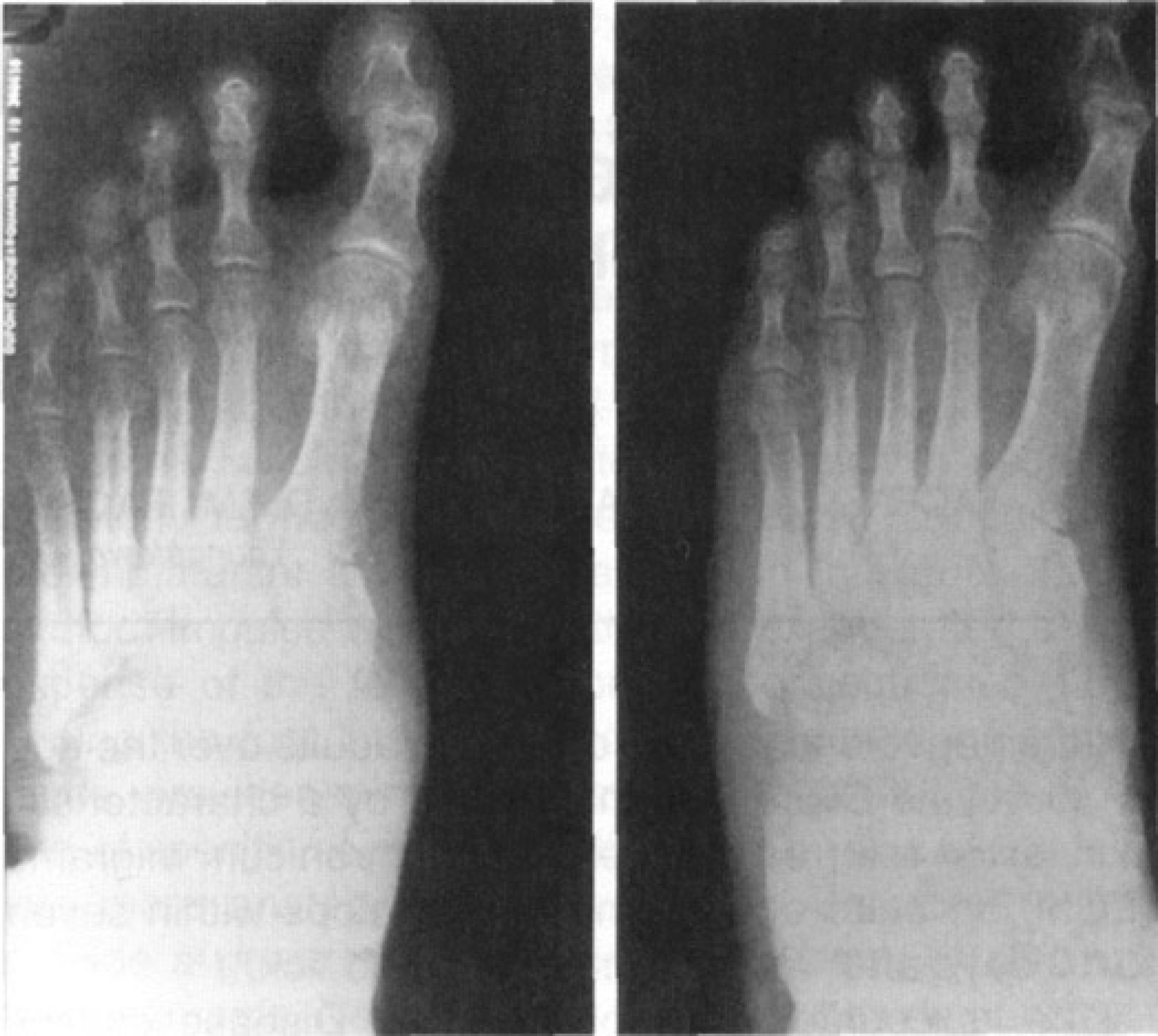
AP view of the foot showing moderate degree of bony eburnation and resorbtion of metatarsals, cuboid, and cuneiforms, at the level of LisFranc's joint bilaterally.
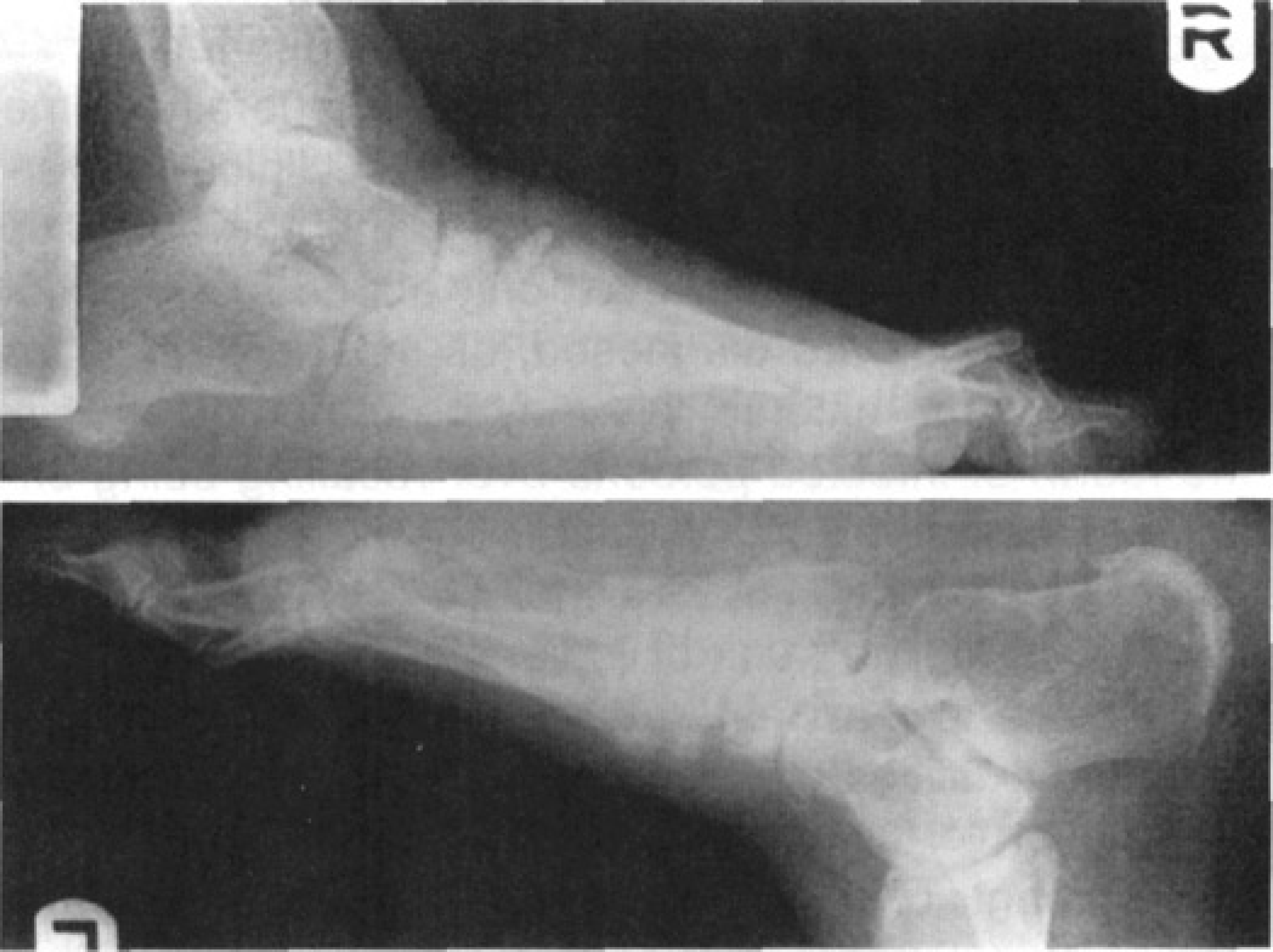
Lateral view of the foot showing extensive destruction of the midfoot joint bilaterally.
Neuropathic Osteoarthropathy
Neuropathic osteoarthropathy occurs as a secondary manifestation of diseases which cause loss of or impairment to sensory input from joint and muscle receptors, as well as control of surrounding vasculature flow. 14,15 The resultant disease processes are characterized by distal bone and joint subluxation, dislocation, and destructive resorption together with hypertrophic periosteal reaction, often affecting weight-bearing joints. 1,6,14,12 Some of the more common disease processes resulting in neuropathic osteoarthropathy include but are not limited to; diabetes, alcoholism, tabes dorsalis, syringomyelia, multiple sclerosis, Charcot-Marie-Tooth disease, peripheral nerve lesions, polio, leprosy, and congenital insensivity to pain. 1,6,7 Recent reports have also mentioned neuropathic osteoarthropathy as a complication following elective foot surgery. 13
CASE Report
A 48-year-old female presented with plantar calluses, numbness, and pain to both feet. She recently noted a progressive flattening of her arches with a prominence developing on the lateral aspect of both feet, as well as an increase in her hammertoe deformity bilaterally. Past medical history is significant for hypertension, hypothyroidism, asthma, arthritis, foot and leg cramps, depression, and Lyme Disease. The patient's Lyme Disease was confirmed by the presence of antibodies at a level of 256 (reference range is zero to 64) as per VDRL assay. The patient's current medications include Zoloft, Synthroid, Neurontin, Demodex, Hydrochlorothiazide (HCTZ), Ativan, Advil, Glucoseamine, and an asthma inhaler. Patient denies having any tobacco or ETOH use.
Vascular examination revealed palpable pedal pulses bilateral with a capillary fill time of less than three seconds. Neurological examination utilizing a 5.07 monofilament showed areas of absent protective sensation to the plantar aspects of both feet. Musculoskeletal examination revealed a decreased range of motion of all midfoot and ankle joints bilateral. Radiographs showed a moderate degree of bony eburnation and resorption of metatarsals, cuboid, and cuneiforms, at the level of Lisfranc's joint of both feet (Figs. 1, 2). Increased talar declination was apparent, as was plantar subluxation of the 4th metatarsal base bilaterally.
Review of clinical and radiographic findings revealed classic changes consistent with neuropathic osteoarthropathy or “Charcot arthropathy.” Peripheral neuropathy was confirmed by sural nerve biopsy. After exclusion of all known causes of peripheral neuropathy, the cause of the patient's neuropathic osteoarthropathy was then believed to be the result of a long-standing history of Lyme Disease-induced peripheral neuropathy. The patient had no other identifiable causes or risk factors which would result in peripheral neuropathy and subsequent neuropathic osteoarthropathy. Thus, it was determined to be the result of her Lyme Disease.
Treatment options for this patient were limited from the standpoint of the bilateral nature of the disease. The patient was informed of the need for strict non-weight-bearing in attempt to slow or stop progression of the deformity. The patient was reluctant to non-weightbearing options and elected for a more supportive approach with the knowledge that the disease process may continue to progress and worsen. The patient was treated with accommodative footwear initially and subsequently fitted for orthotics in an attempt to support the medial arches. After eight months from initial visit, the patient's midfoot changes still show signs of slow progression. This would be expected in a patient who continues to ambulate. The patient is mildly improved with some continual pain in the lower extremity at this time.
CONCLUSION
The association of Lyme-Disease-induced peripheral neuropathy resulting in neuropathic osteoarthropathy changes in any joint have not been reported until now. Some original studies of the disease were associated with a patient population predominately having tertiary syphilis, thus putting the two disease processes in the same category of spirochete-induced neurological manifestations. The process of Treponema-pallidium-induced peripheral neuropathy has been reported in previous literature as a possible cause of neuropathic osteoarthropathy. 11,15 This is the first reported presentation of a very similar process in conjunction with the spirochete Borrelia burgdorferi. All too often when the term “Charcot deformity” or “neuropathic osteoarthropathy” is mentioned we immediately think of a patient with diabetes mellitus, when in fact we should consider that the patient may have a peripheral neuropathy secondary to a separate etiology.