
Abstract
The membranes present at the implant-bone interface were retrieved from two patients with titanium single stem hallux implants that had failed. Both patients had pain and valgus deformity of the hallux, and radiographs showed a radiolucent shadow around the implant stem, with thinning of the dorsal cortex of the proximal phalanx in one patient. After removal of the implants, arthrodesis of the first metatarsophalangeal (MP) joint was performed. Histologic analysis of the membrane tissue at the implant-bone interface showed a synovial-like appearance. There was a fibrous tissue stroma adjacent to the bone surface, with multiple regions of scalloping covered by mononuclear cells. Fine metallic debris was seen throughout the fibrous tissue. Multinucleated foreign body giant cells were sparsely observed associated with fine particulate metallic wear debris similar to observations from failed total hip arthroplasties. The histologic appearance is evidence that foreign-body granulomatous infiltration associated with metallic wear debris may be a causative factor of peri-implant osteolysis leading to aseptic loosening and failure of titanium single stem hallux implants.
INTRODUCTION
Various surgical treatment options for hallux rigidus have been described, including open or arthroscopic debridement, cheilectomy, resection arthroplasty, arthrodesis, and prosthetic replacement. 5,6,9,11,17 –19,25,27,28,38,40,42,43 First MP joint implant arthroplasty gained popularity after results with silicone rubber implants were reported. 40 Subsequently, various implant designs have been developed, 1,3,5,9,17 –19,23,27,28,38 including the titanium hallux MP implant consisting of a tray replacing the joint space and a single stem in the proximal phalanx. 3,23 Reported advantages of implant arthroplasty include pain relief and preservation of joint motion and length. 1,3,5,17,18,23,42 Complications of implant arthroplasty include joint stiffness, joint instability, transfer lesions, implant loosening and failure, silicone synovitis, soft tissue foreign body reaction, and progressive shortening of the hallux. 20,24,32,38,43
The transformation of intact implant material into particulate debris, and the capacity to induce a foreign-body granulomatous membrane response, are important in the development of osteolysis leading to aseptic loosening of other orthopaedic implants such as total hip prostheses. 7,8,15,16,26,29,30,33,37,44 However, there is no available information about the synovial-like membrane at the implant-bone interface of failed titanium single stem hallux implants. In this study, we analyzed the membrane retrieved from two failed titanium single stem hallux implants to evaluate the hypothesis that metallic wear debris may cause a foreign-body reaction that may result in osteolysis and implant loosening.
CASE REPORTS
CASE 1
A 71-year-old woman with a history of gout, currently treated with colchicine, had had left first MP joint titanium single stem implant arthroplasty 2.6 years earlier at another institution. She had had open treatment of an ipsilateral left calcaneus fracture eight months ago. She currently developed acute pain at the left hallux with associated bruising, without recent trauma. The left hallux proximal phalanx was tender, and the hallux was in more valgus alignment than previously. Radiography showed that the MP joint implant was in dorsiflexion relative to the proximal phalanx, with the tip of the stem abutting against the thinned and expanded dorsal cortex of the proximal phalanx. There was a zone of radiolucency around the implant stem inside a surrounding sclerotic rim (Fig. 1).
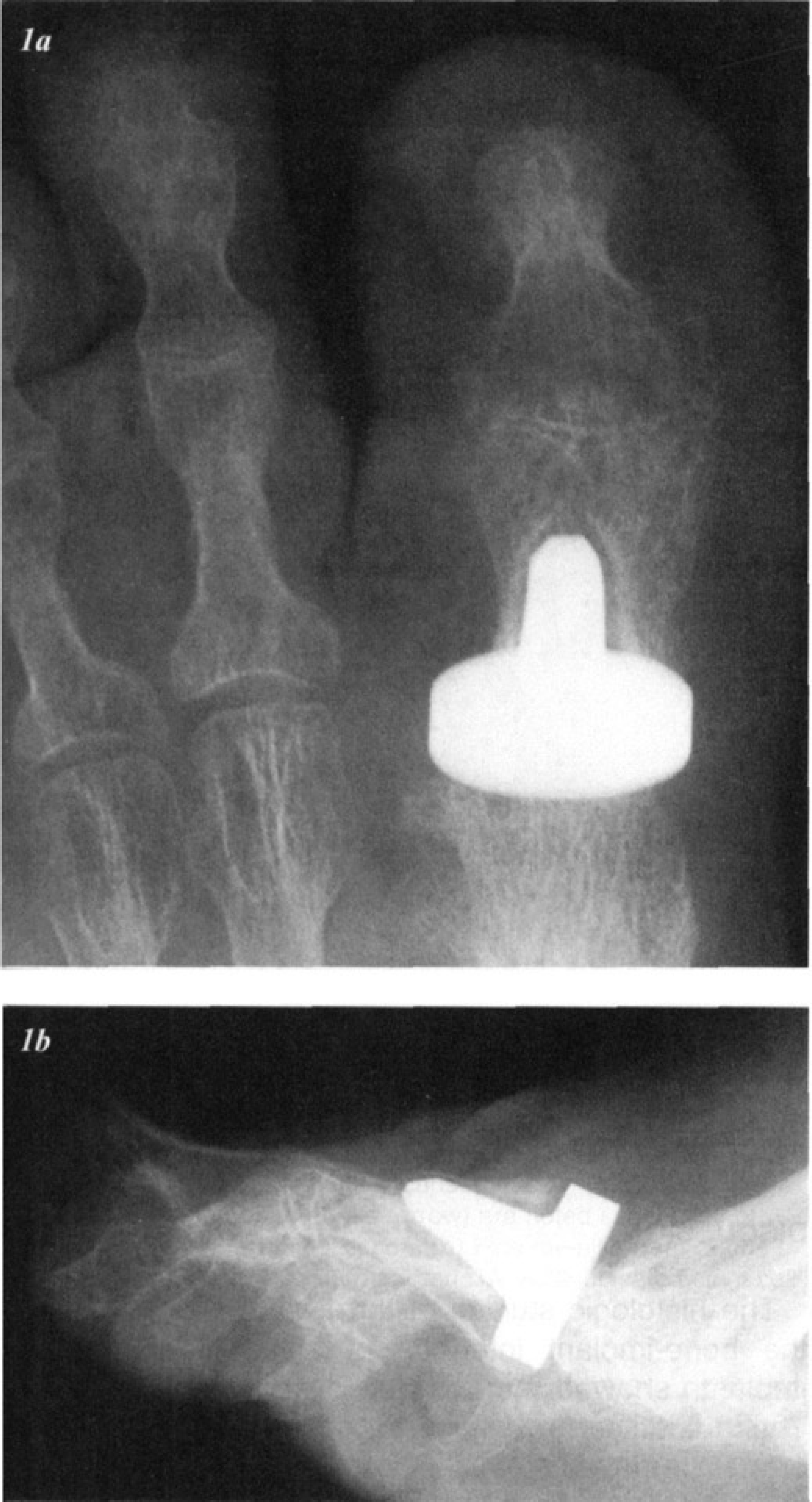
Preoperative radiographs of the left hallux in a 71-year-old woman, 2.6 years after titanium single stem first MP implant arthroplasty (case 1).
CASE 2
A 65-year-old woman had had first MP joint titanium single stem implant arthroplasty 3.9 years earlier at another institution. She currently presented with a six-month history of progressively increased hallux valgus deformity and pain at the first and second MP joints. Examination showed hallux valgus deformity and pain with limited motion of the first MP joint. There was tenderness of the second MP joint, distal migration of the plantar fat pad, and an intractable plantar keratosis under the second metatarsal head. The valgus hallux was dorsal to the medial edge of the second toe. Radiography showed radiolucency around the prosthetic stem on all views with a surrounding sclerotic rim; the first metatarsal was shorter than the second metatarsal, and the hallux proximal phalanx was in valgus relative to the implant stem.
Operative Findings and Treatment
Implant removal and arthrodesis of the first MP joint was done. Indications for surgery included pain from implant failure with osteolysis, progressive deformity, and impending fracture of the proximal phalanx cortex. Operative findings in both cases included a grossly loose, intact single stem implant (Swanson Titanium Great Toe, Wright Medical Technology, Arlington, TN) without any visible evidence of corrosion or discoloration of surrounding tissues (Fig. 2). There was a dense, white, fibrous membrane between the implant tray and the first metatarsal head. The canal of the proximal phalanx was lined with a thick, white, fibrous membrane between the implant stem and the bone. In the first patient, the dorsal cortex of the proximal phalanx was egg-shell thin and dorsally expanded; in the second patient, the implant stem was loose within the nonexpanded proximal phalanx shaft. Operative cultures showed no evidence of infection. After the implant was removed and the fibrous membrane excised, the proximal phalanx canal was curetted and packed with cancellous distal tibial bone graft, 31 and the arthrodesis was fixed with a dorsal mandibular plate and screws. 4,34 Aftercare included non-weight-bearing for the initial six postoperative weeks and protection with a wooden postoperative shoe or removable cast boot until consolidation of the arthrodesis was confirmed by 12 weeks after surgery. Satisfactory pain relief was achieved in both patients.
Histology
Tissue specimens from the bone-implant interface of both patients were evaluated. The fibrous tissue membranes with attached bone fragments were excised from the proximal phalanx cavity after implant removal. The specimens were fixed in 4% paraformaldehyde (two days) and then decalcified in 14% EDTA (two weeks), washed in graded ethanol solutions, and stored overnight at 4°C in 100% ethanol. The specimens were then transferred to xylenes and embedded in paraffin. Tissue sections were cut, stained with hematoxylin and eosin, and examined under a microscope.
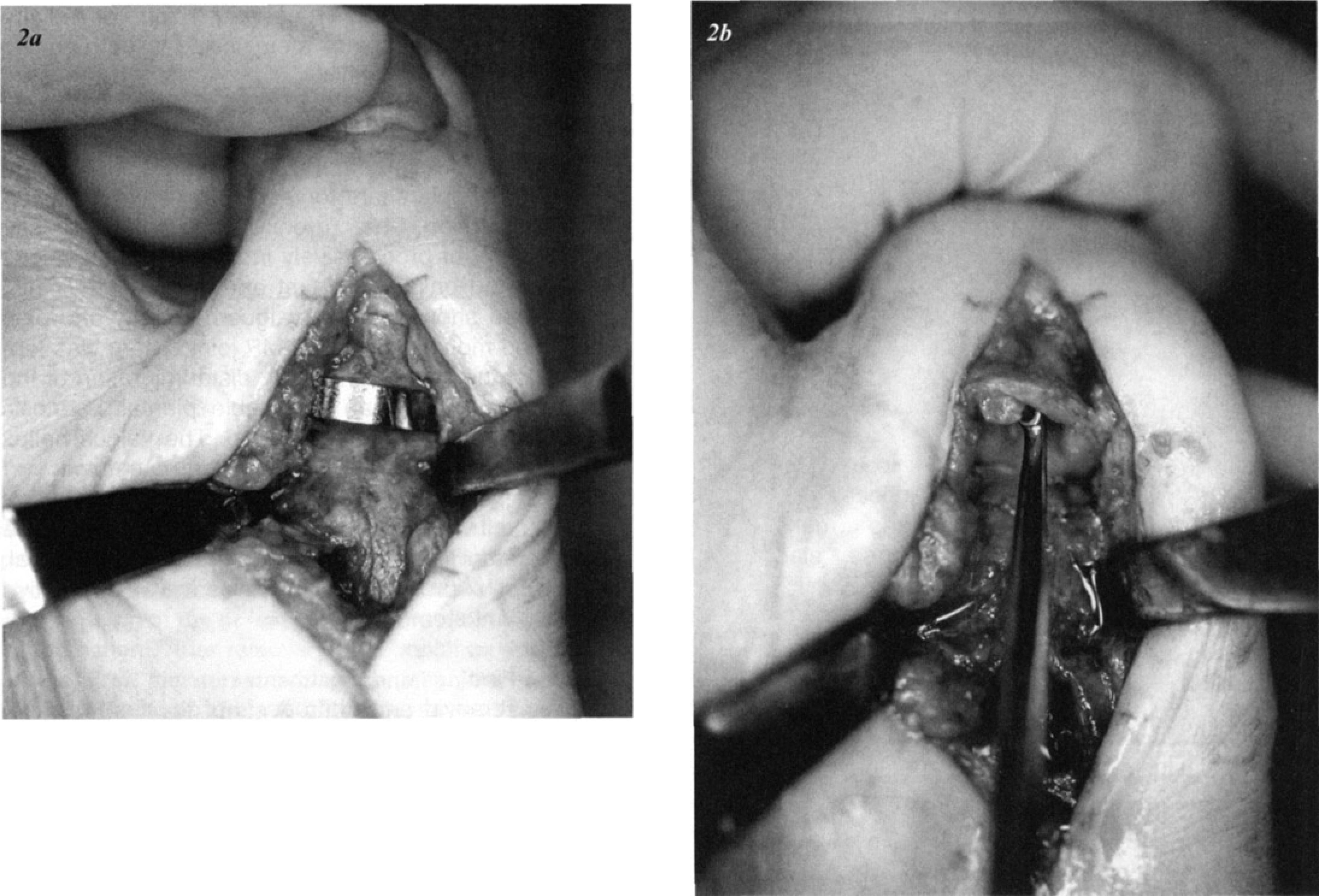
Intraoperative appearance of failed titanium single stem first MP implant arthroplasty (case 1).
Histologic analysis of the tissue from both patients revealed fibrous tissue stroma adjacent to the bone surface, which showed multiple regions of scalloping, covered by mononuclear cells (Fig. 3, 4). Fine metallic debris was seen throughout the fibrous tissue. A mild monocytic infiltrate was present, but polymorphonuclear leukocytes were absent. Multinucleated foreign-body giant cells were sparsely observed associated with fine metallic wear debris.
DISCUSSION
The histologic studies of the tissue membrane from the bone-implant interface of failed titanium hallux implants showed metallic debris and cellular reaction. These findings are similar to those observed in membranes retrieved from the implant-bone interface and the iliopsoas bursa of total hip arthroplasties complicated by aseptic loosening and osteolysis. 7,8,15,16,26,29,30,33,35,37,44,45 A similar reaction had also been observed in association with a loose custom total-knee titanium prosthesis. 39 Information about the mechanism of failure and technique for salvage of failed titanium hallux implant arthroplasty should be useful because this procedure continues to be recommended by some practitioners 36 and is currently used in approximately 1,500 joints annually in the United States. 14
Radiolucent lines may occur adjacent to well-fixed total hip prostheses without a fibrous layer as a result of peri-implant osteoporosis. 21 Furthermore, reaction to titanium may occur in a well-fixed total hip replacement as a result of wear debris from the prosthetic femoral head 2,22 or screws 22 or cell-mediated immunity to titanium. 22 However, the hallux prostheses in the current study were noted at surgery to be grossly loose and were associated with a fibrous membrane. The macrophages and multinucleated giant cells observed (Fig. 3, 4) are characteristic of a foreign body granuloma caused by the metallic debris. Scalloping of the bone surface with mononuclear cells is consistent with osteolysis resulting from active bone resorption by inflammatory cells. Cell cultures of the retrieved membranes from hip implants have shown that this tissue may produce a variety of substances, including prostaglandin E2, collagenase, interleukin-1, and tumor necrosis factor, 7,8,29 that may contribute to bone resorption and osteolysis. 7,8,12,29 The absence of polyethylene from the hallux MP implants excludes this polymer—commonly used in total hip prostheses—as a potential source of inflammation in the current cases. Therefore, the histologic findings about the failed titanium hallux MP implants support the hypothesis that aseptic loosening of the implants, with osteolysis at the bone-implant interface, was caused by a foreign-body granulomatous inflammatory reaction associated with metallic debris, similar to that observed in aseptic failed total-hip arthroplasties.
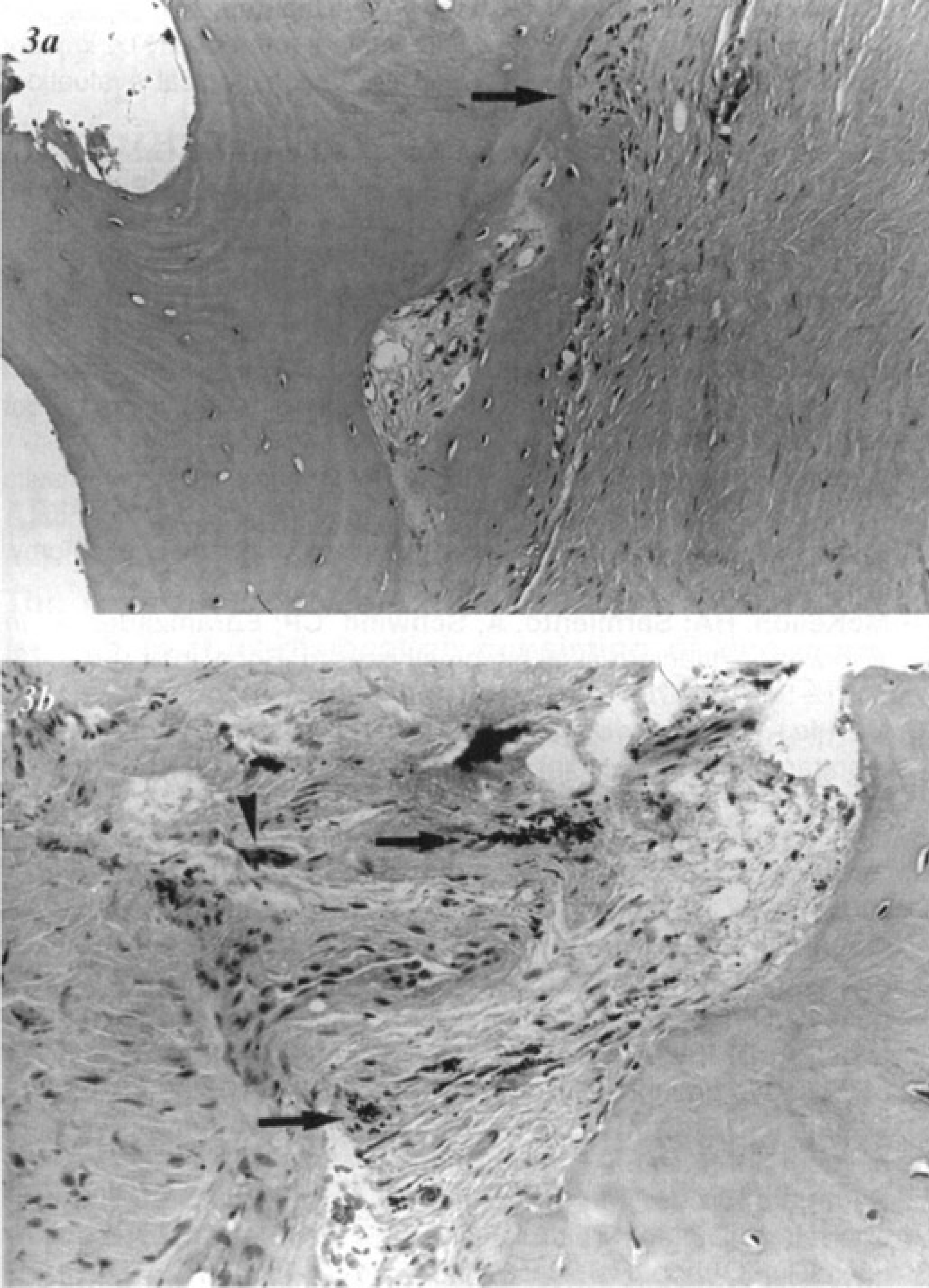
Microscopic appearance of the membrane-bone interface excised from the proximal phalanx canal (case 1).
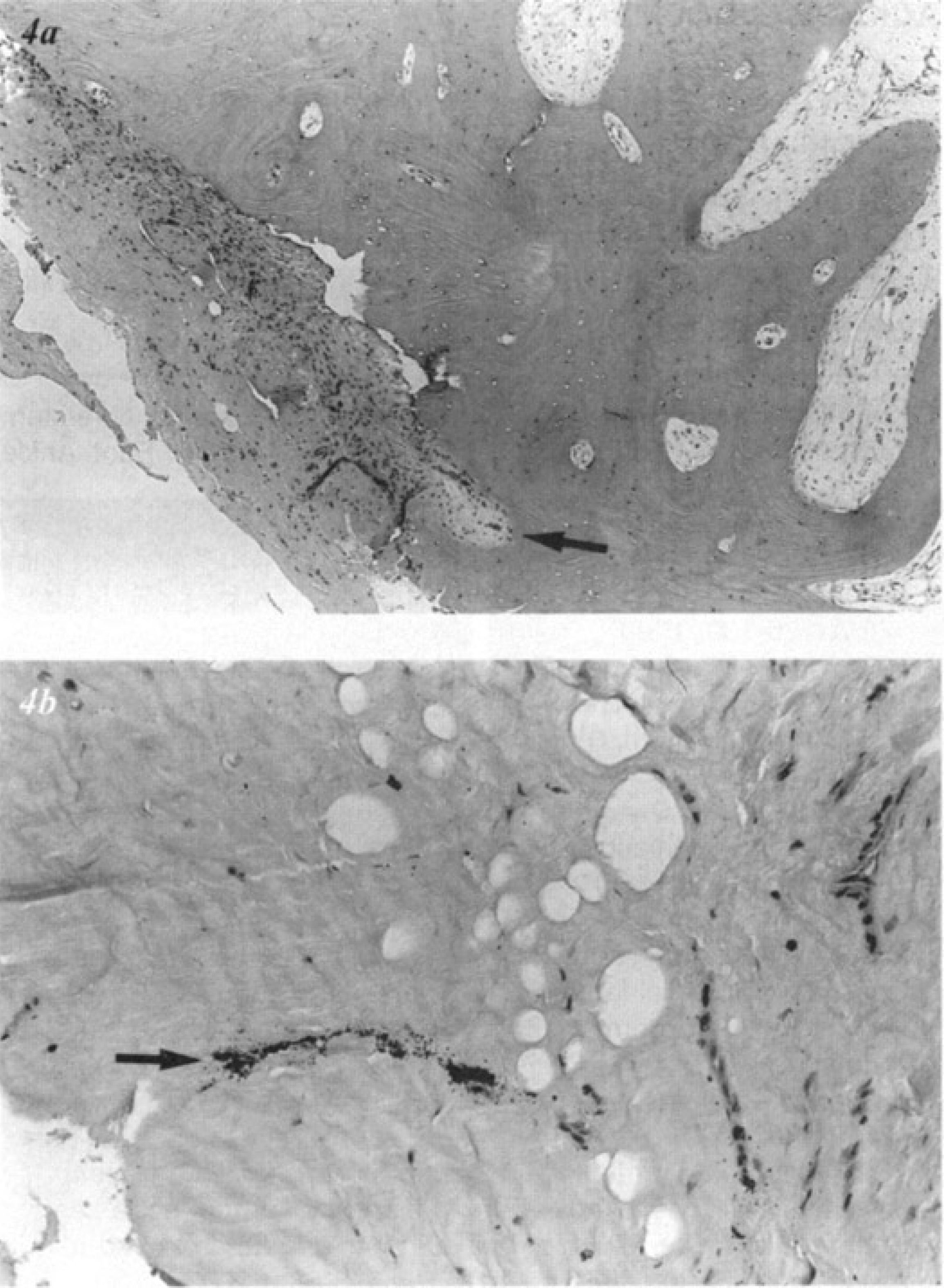
Microscopic appearance of the membrane-bone interface excised from the proximal phalanx canal (case 2).
Titanium has been used in joint arthroplasty because of favorable characteristics including low density, high tensile strength, excellent resistance to fatigue, superb ductility and formability, low modulus of elasticity, remarkable anticorrosive properties, and superior biocompatibility. 13,35 In contrast, the known liabilities of titanium may include poor resistance to wear, notch sensitivity, and potential toxicity. 33,41 The gross black staining previously observed in the membranes adjacent to failed total-hip implants had been attributed to metallic debris contained within histiocytes and giant cells. 7,8,29,33 The absence of gross black staining of the tissues about the hallux implants is consistent with the histologic finding that the inflammatory cellular reaction was sparse, perhaps attributed to factors such as implant size, duration of implantation, and local tissue vascularity.
Footnotes
ACKNOWLEDGEMENTS
S.R.G. is supported by grants R01-AR-45472 and R01-DK-46773 from the National Institutes of Health. Fellowship support to A.N. from the John Charnley Trust (UK) is gratefully acknowledged.