
Abstract
Proximal osteotomy and distal soft tissue correction is recommended for correction of severe hallux valgus deformity. Basal closing wedge osteotomy is inherently unstable, and there is a tendency for dorsal displacement of the distal fragment. This has led many surgeons to attempt a variety of fixation techniques to counteract this instability, including AO-cortical and cancellous screws, K-wires, and shape-memory staples. 1 –3
The Acutrak® screw (Acumed. Inc., Beaverton, Oregon) has been used to fix tibial spine avulsions and scaphoid fractures 5 but was not previously reported in hallux valgus surgery. We used a modified closing wedge basal osteotomy technique with Acutrak cannulated compression screw in order to add stability to the osteotomy.
Proximal osteotomy and distal soft tissue correction is recommended for correction of severe hallux valgus deformity. Basal closing wedge osteotomy is inherently unstable, and there is a tendency for dorsal displacement of the distal fragment. This has led many surgeons to attempt a variety of fixation techniques to counteract this instability, including AO-cortical and cancellous screws, K-wires, and shape-memory staples. 1 –3
The Acutrak® screw (Acumed. Inc., Beaverton, Oregon) has been used to fix tibial spine avulsions and scaphoid fractures 5 but was not previously reported in hallux valgus surgery. We used a modified closing wedge basal osteotomy technique with Acutrak cannulated compression screw in order to add stability to the osteotomy.
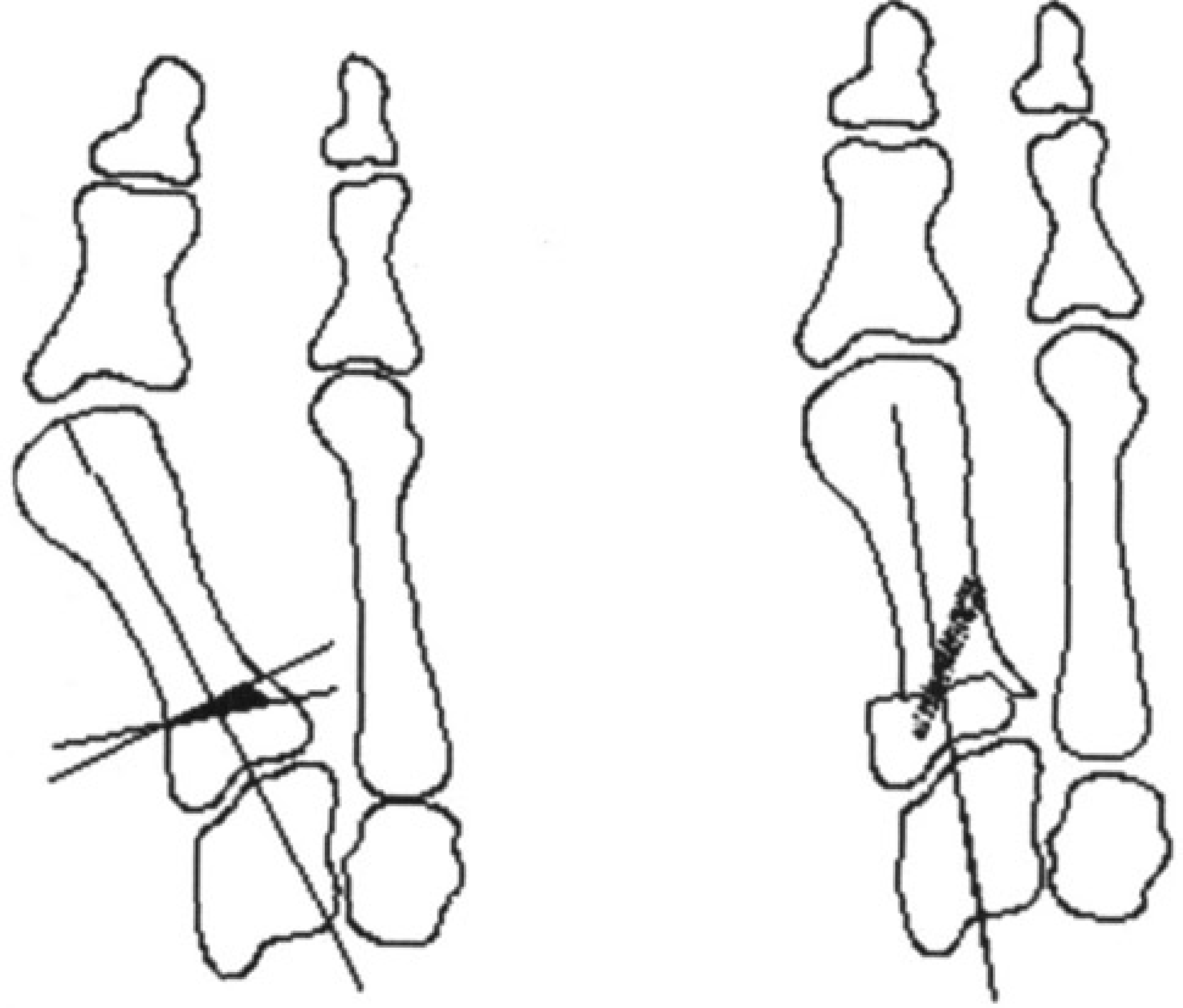
The laterally based closing wedge osteotomy.
The technique offers several advantages. The lateral spike on the distal fragment of bone, the fully threaded, variable pitch, and tapered outside profile design of the screw (Fig. 2) provide additional stability to the osteotomy. The screw is headless which reduces problems with soft-tissue irritation and out of the 32 screws we used, only one had to be removed because of infection (Fig. 3).
SURGICAL TECHNIQUE
A single incision is made over the dorsomedial aspect of the first metatarsal. A medial J-shape capsular flap is raised and the medial eminence is removed. Adductor hallucis tenotomy and release of the 1st MTP lateral collateral ligament are performed. Through the proximal part of the incision, a transverse wedge is made sparing the lateral cortex, where a spur of bone is left intact for stability (Fig. 1). The laterally based volar wedge is removed from the distal fragment and the distal fragment is displaced laterally until the spike rests on the lateral cortex of the proximal fragment and the wedge is closed (Fig. 1). A temporary guide pin is inserted from the dorsal-lateral surface of the distal segment to the plantar-medial surface of the proximal segment and the length of the pin inside the bone is measured. A cannulated drill/reamer is used to make the screw hole, the self-tapping screw is inserted over the pin, and the guide pin is removed. Medial capsular reefing is performed and a fiberglass slipper cast is applied for six weeks.
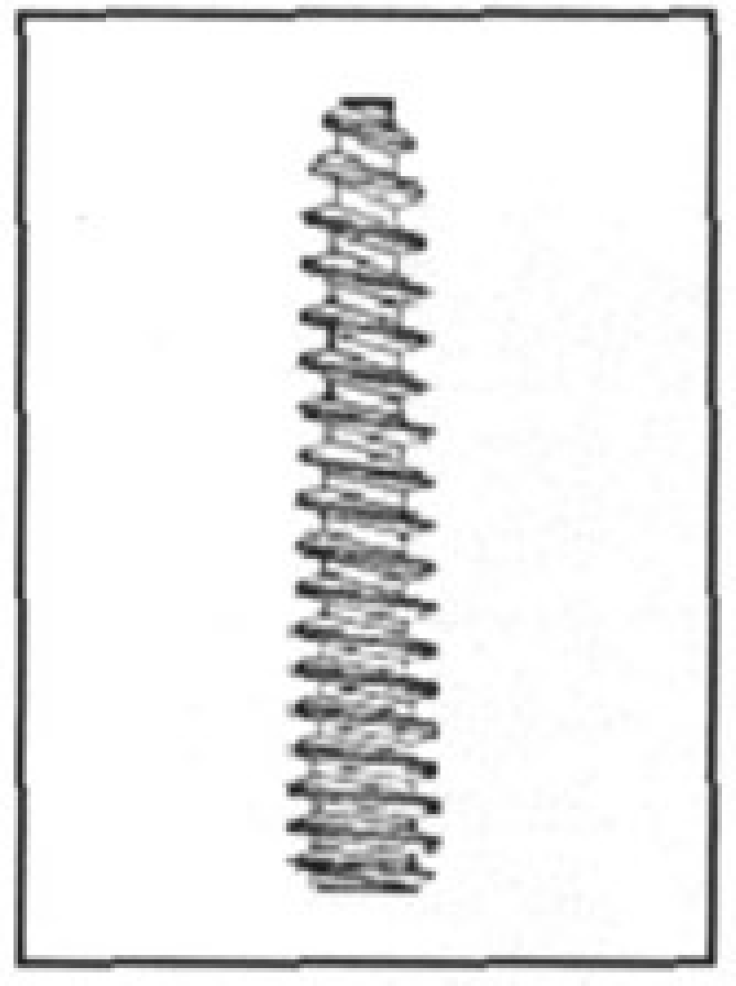
Acutrak screw.

AP weight-bearing radiograph showing a healed osteotomy, six weeks post surgery.
Footnotes
ACKNOWLEDGEMENT
We wish to thank Mr. Ian Christie at the University of Dundee for his valuable help with the illustrations.