
Abstract
Stress fracture of the medial malleolus is rare and not reported in children. We report a case of a 15-year-old elite gymnast with open physes sustaining a medial malleolar stress fracture. The patient was treated initially by rest and gradually returned to sport with full recovery. Two months later she developed a complete fracture of the medial malleolus of the same side. This was treated surgically by open reduction and internal fixation with a cancellous screw and soon after the operation she returned to full activities. Emphasis is given to the suspected mechanism which led to this unique fracture and to the hormonal aspects in the professional adolescent gymnast.
We recommend surgical treatment of stress fracture of the medial malleolus especially for elite athletes, leading to early recovery and return to sports activities.
INTRODUCTION
Stress fractures of the lower extremities tend to occur in the distal tibia and fibula. 5 In patients with closed growth plates, the exact location of these stress fractures is usually the posteromedial-concave side of the tibia. 6 However, in adolescents, the distal tibial physis begins closure centrally and continues medially, often leaving the lateral side unclosed at the time of injury. This is probably what causes the lateral aspect of the distal tibia to be susceptible to injury. 13 This fracture in adolescent children has been termed the juvenile fracture of Tillaux, after the French surgeon who described it. 13 In this case report, a unique stress fracture, which was complicated leading to complete fracture of the medial aspect of the distal tibia in a 15-year-old elite gymnast is described.
CASE REPORT
A 15-year-old elite gymnast presented to our department with the complaint of intense pain of the left ankle felt after a dismount. Discomfort in the ankle was noted for two weeks previous to the competition but was experienced only during training. Regular activities caused no pain. The patient stated at the completion of the dismount the ankle struck the surface in a dorsiflexion, inversion position. Physical examination showed moderate tenderness medially over the left distal tibia with full range of motion. A diagnosis of a stress fracture was made based on the physical examination, radiograph examination and bone scan. The fracture started at the tibial plafond and extended vertically just below the level of the fused growth plate. The lateral epiphysis was still open (Fig. 1).
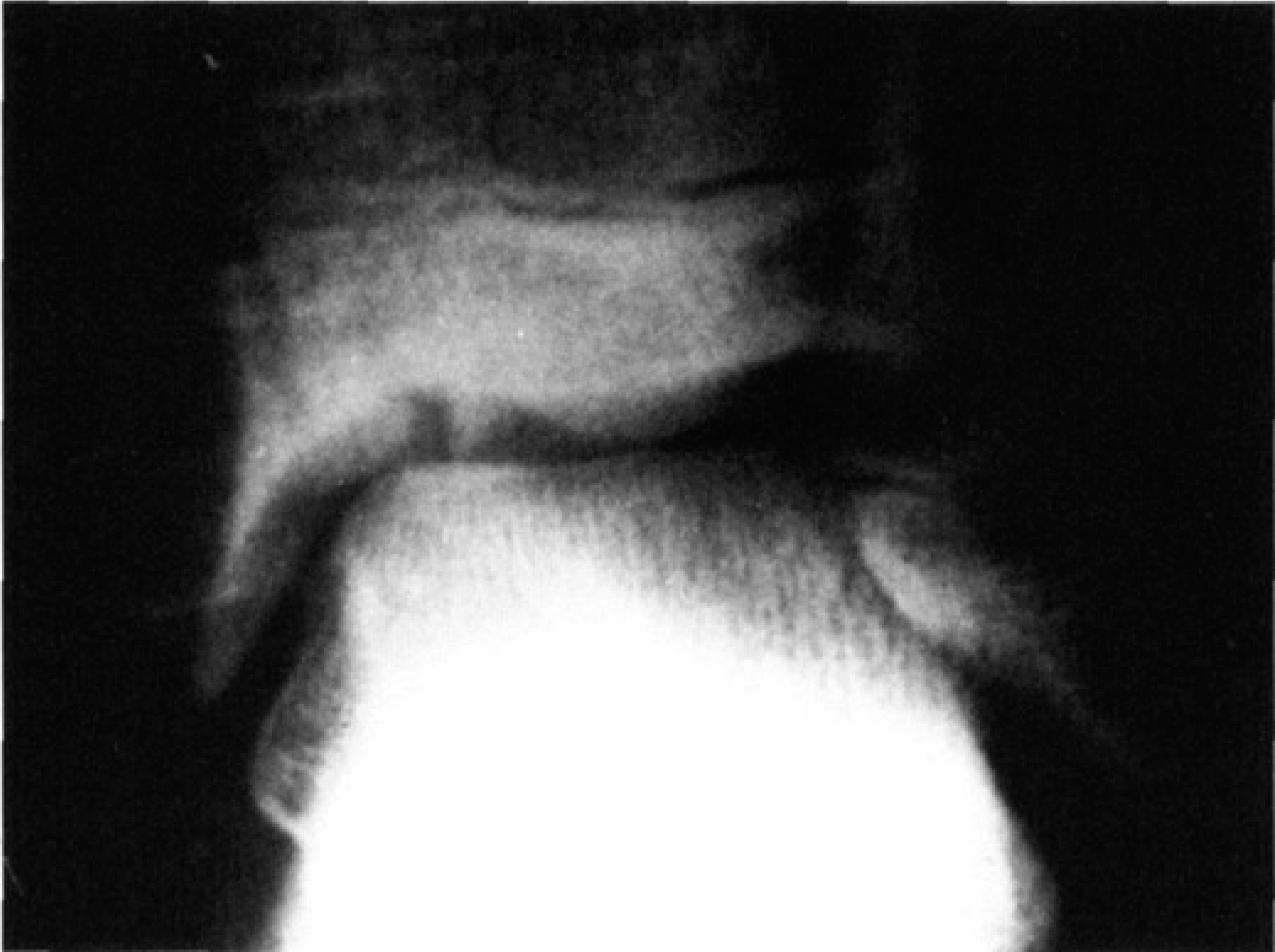
Plain radiograph of the ankle (AP view), showing a vertical medial malleolus fracture.
The patient was placed in an elastic bandage and counseled to avoid training for six weeks. After six weeks the patient returned gradually to a full training regimen. This decision was made on clinical grounds in the absence of symptoms.
Two months later, the patient developed pain on the medial side of the left ankle during a dismount at a competition. On physical examination, a severe tenderness over the medial aspect of the ankle was noted. Plain X-rays and CT scan confirmed an undisplaced fracture of the medial malleolus (Fig. 2).
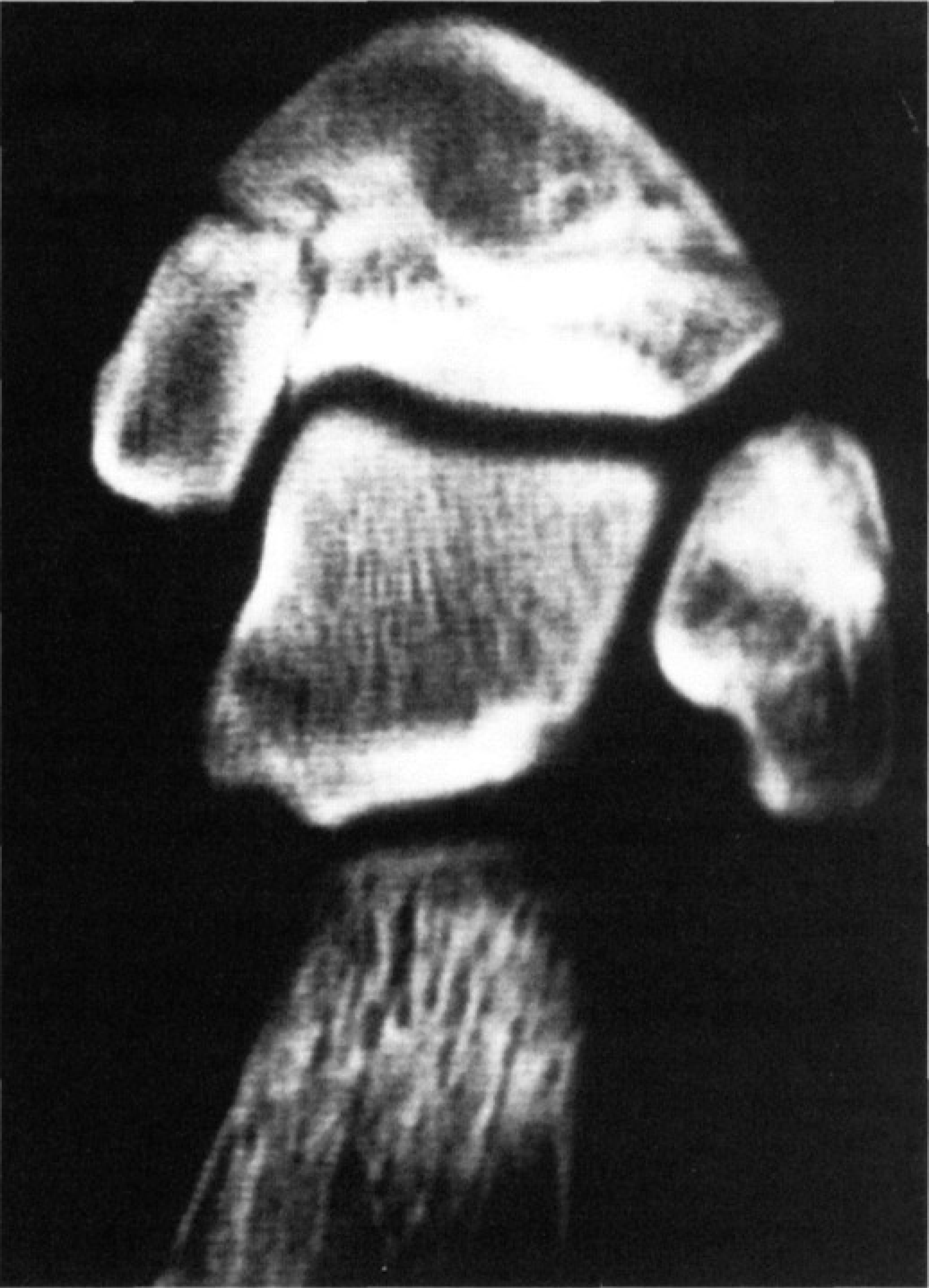
CT of the left ankle region, showing undisplaced fracture of the medial malleolus.
The patient was amenorrheaic and only started her menses during the break in training. She therefore underwent full endocrinological evaluation, including bone mineral density (BMD), which was found to be normal.
The fracture was treated by open reduction and internal fixation using a cancellous bone screw for the medial malleolus (Fig. 3). The patient was immobilized in a cast for two weeks, followed by a gradual return to a full training regimen. In routine follow-ups no pain or limitation in range of motion were noted and radiographs showed complete healing. At two year follow-up the patient has no limitation in her fully demanding activities, and she continues to take part in international competitions.
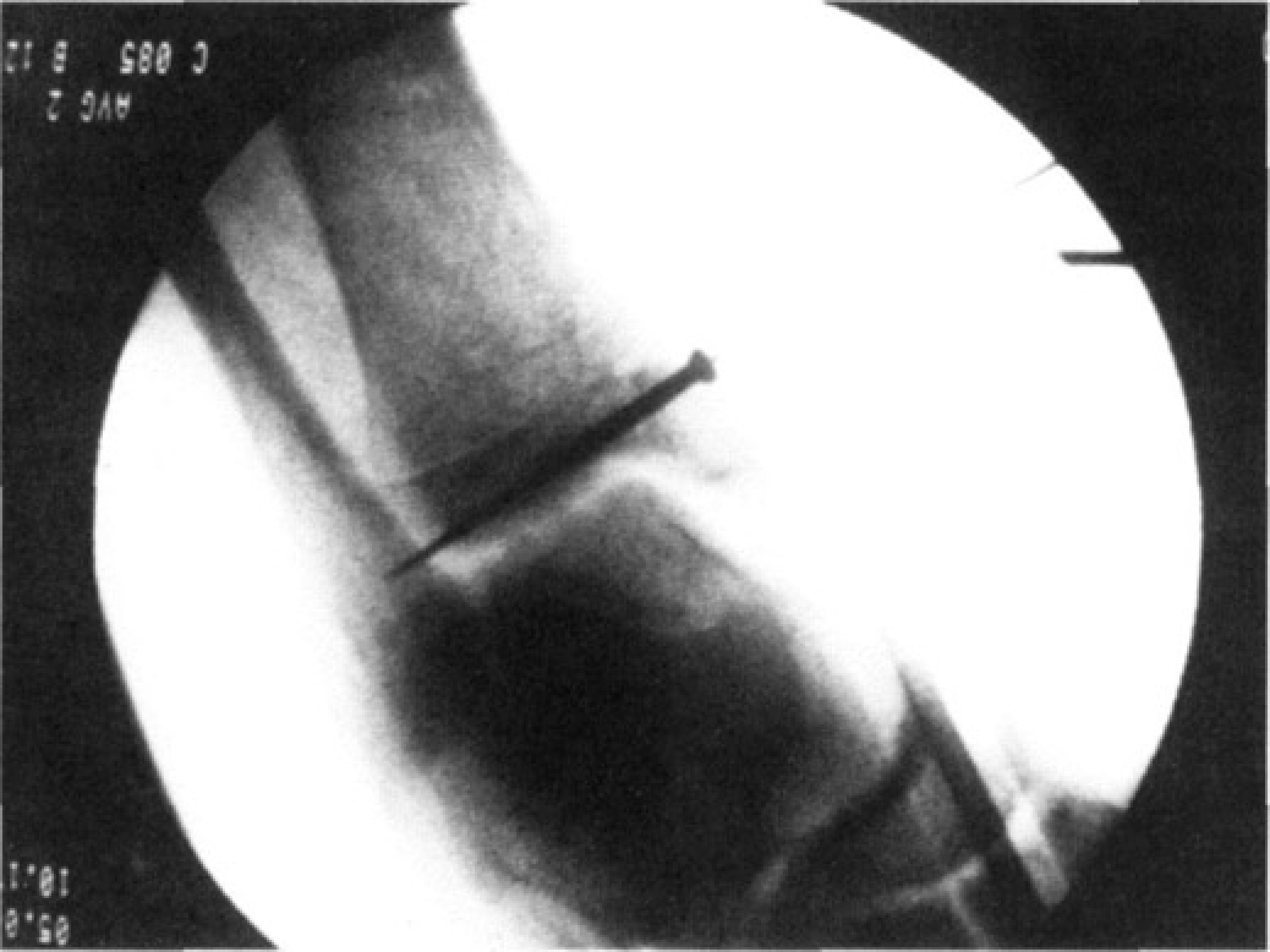
Intra-operative fluoroscopy of the ankle in the mortise view after fixation of the fragment with a cancellous screw.
DISCUSSION AND LITERATURE REVIEW
Twenty-two cases, including the present report, described in four papers from 1988 to 1995 comprise this survey. 7,10,11,12
Shelbourne and co-workers published what they thought to be the first series of stress fractures of the medial maleolus.
12
They established three basic criteria for the evaluation of stress fractures:
tenderness over the medial malleolus and a joint effusion, pain during activities before an acute episode, and a vertical line from the tibial plafond.
Of the six cases they reported, one was female, an 18-year-old basketball player with a presumed closed physis. No adolescents were reported.
Orava et al. reported a series of eight cases. 7 All their patients were involved in some type of sporting activities with running and jumping being the most common. Among these eight cases only one female was reported, a 60-year-old recreational athlete. 7 Another study reported one case of nonunion of a medial malleolar stress fracture found in a 21-year-old college football player. 10 Schils and co-workers described the clinical and radiographic findings in a series of seven patients with medial malleolar stress fractures. 11 Two female patients, a 31-year-old and a 16-year-old (the youngest in this series), with a simultaneous stress fracture of the homolateral navicualr bone, were included in their series. Though the exact participation in sport activity was not mentioned for each one of the patients, it was stated that six out of the seven patients were involved in running and jumping athletic activities. 11 Two of the stress fractures progressed to complete fractures of the medial malleolus, similar to our case. Our patient met these criteria in the two episodes. She had pain and tenderness over the medial malleolus, and a typical plain X-ray and CT scan.
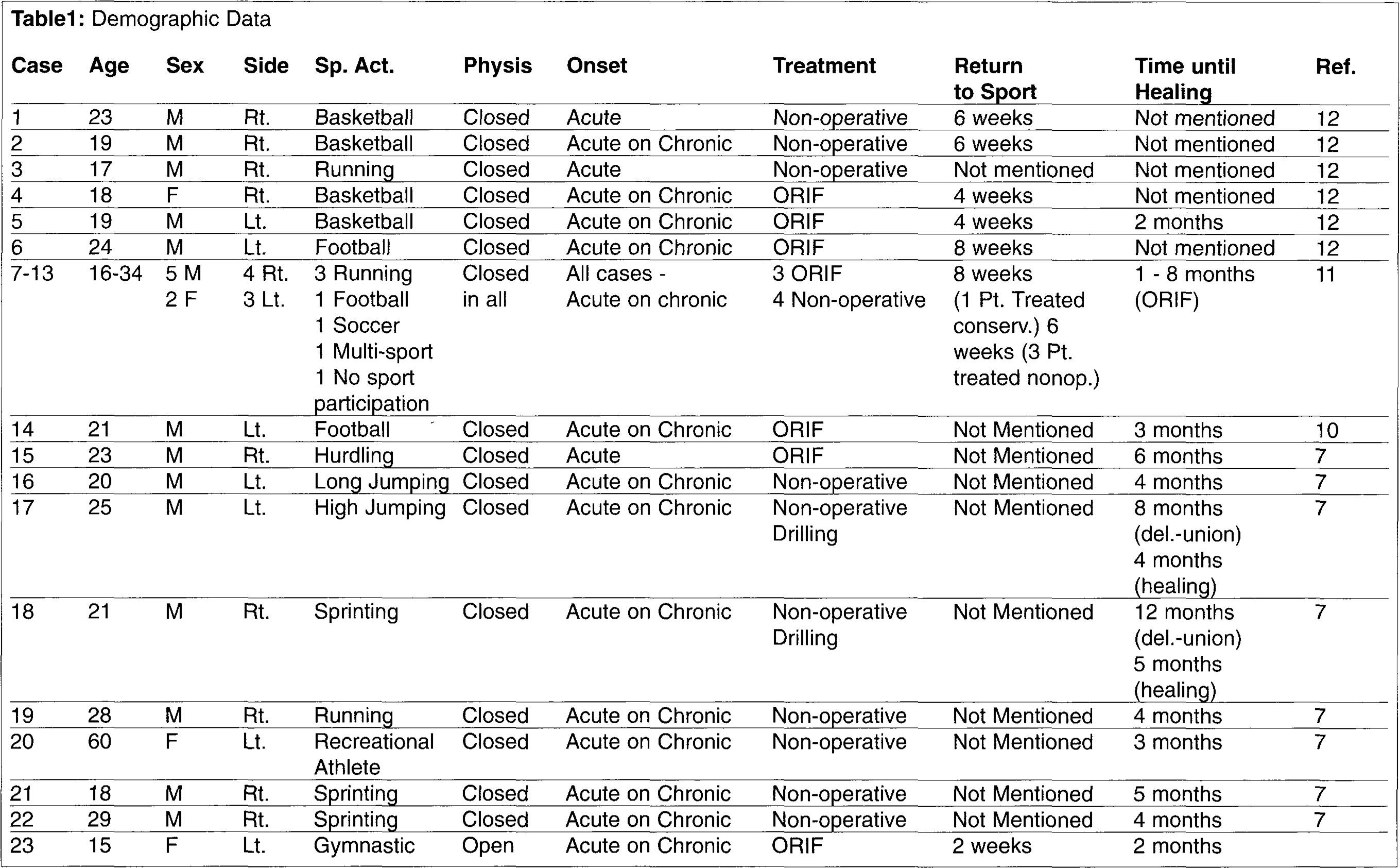
The data of the 23 patients reviewed are summarized in Table 1.
In four published articles on medial malleolar stress fractures, 7,10,11,12 including our case report, there were 18 males and five females aged between 15 and 60 years (mean: 24 years). All patients, except one, were involved intensively in sport activities, and most of them were reported to be professional. In all previously reported cases the physis of the injured ankle was not reported to be open, and it is assumed that it was closed by the time of injury (the youngest reported case is a 16-year-old female). In our case, the physis in a 15-year old female was still open. The onset of the injury was divided into two categories. Acute phase was referred to as a fracture without predisposing symptoms, while acute on chronic was referred to as a fracture which was accompanied by a duration of gradual onset of pain and discomfort over the ankle (Table 1). In three of the patients an acute onset was noted, while for the 20 remaining patients an acute on chronic episode was reported. Twelve patients were treated by cast (non-weight or weightbearing) or air-cast for different periods of time, and then gradual return to sport. Nine patients were treated operatively by open reduction and internal fixation, and two patients were treated initially conservatively, followed by drilling procedure because a delayed union of the fracture was noted. Return to sport activities was mentioned for 10 of the patients, and was between two and eight weeks. This return was performed gradually, and was six weeks for the five patients and eight weeks for one patient treated non-surgically, compared to 4.5 weeks on average for the four patients treated operatively. The time elapsed until complete healing of the fracture was mentioned for 12 patients and ranged between two and eight months (for two patients drilling was performed eight and 12 months, respectively, after a delayed union). Healing was considered after the drilling procedure. Among these 12 patients five underwent open reduction and internal fixation and complete healing was reported after 4.2 months on average, while for seven patients treated non-surgically (including the two patients that eventually underwent drilling) it took 6.7 months on average.
Demographic Data
The sport of gymnastics is unique in promoting bone density. Several studies have documented gymnastics as superior when compared to other sports regarding bone formation. Female gymnasts were compared to runners and swimmers and were shown to have significantly greater BMD. The high impact nature of gymnastics, producing acute strains on bone, was suggested as the reason for the increased BMD. 1,2,14 Low levels of BMD, especially in elite athletes, is considered to be one of the reasons for stress fractures. 8 Our patient had normal BMD. This measure is compared to the average population and probably represents a lower level in our patient due to her high activity needs. Our patient did not have any other contributing factors to stress fractures like menstrual irregularities (although her menses started late), dietary factors or prior history of stress fractures. 8
In our patient and literature review the time to complete fracture healing was shortened in this entity by open reduction and internal fixation. In the elite athlete there is a tendency to move more quickly to operative treatment. However, operative risks and potential complications should be explained in detail to the athlete, or his/her parents in case of a minor.
CONCLUSION
We comprehensively reviewed the literature of patients with medial malleolar stress fractures. This was found to be almost exclusively in athletes who were involved in sports activities, mainly jumping and running. It is our opinion, based on our literature review and on our personal case, that surgical treatment yields better results and more rapid return to sports activities than non-surgical. Because of this we feel surgical treatment should be considered earlier in the treatment of elite athletes. Non-surgical treatment may lead to prolonged healing and recurrent stress fractures.