
Abstract
The purpose of this study was to evaluate the biomechanical properties of commonly used autogenous transplants for the surgical stabilization of chronic lateral ankle instability. We dissected the transplants (peroneus longus, peroneus brevis, Achilles and plantaris tendon, periosteal flap, fascia, corium) and the anterior talofibular ligament from 13 fresh anatomic specimens. After laser-assisted measurement of the transplant diameter, we assessed their biomechanical properties with a universal testing device. Biomechanical stability of the peroneus longus, peroneus brevis, and Achilles tendons was significantly higher than the other transplants. The stability parameters of the periosteal flap were in the range of the anterior talofibular ligament but inferior to the tendons. The application of a transplant with low biomechanical stability, such as the periostal flap, requires more postoperative immobilization as in a strong orthosis or cast.
INTRODUCTION
Rupture of the lateral ankle ligaments is one of the most common injuries with an incidence of 1/10000 athletes per day. 24,26 In spite of adequate diagnosis and therapy, 4 to 5% of these patients develop chronic post-traumatic lateral ankle instability. 5,6,18,22,24 Operative stabilization of the ankle is recommended if instability symptoms last for more than six months after injury and ligament laxity can be demonstrated by clinical or radiographic examination, and adequate physiotherapy has failed. 13 Functional instability, i.e. proprioceptional deficits, pain and peroneal muscle weakness, have to be carefully excluded before surgery is indicated. 1,10,16,20
More than 50 different procedures have been described in the literature for operative ankle stabilization. 4,24 They are divided into anatomic techniques (using an autograft according to the anatomic position of the anterior talofibular and fibulocalcaneal ligament) and tenodeses techniques, which are designed to statically limit hindfoot inversion. The aim of our study was to assess the primary biomechanical properties of the most commonly used autografts for lateral ankle stabilization surgery. The different surgical techniques of intraoperative graft fixation and the biology of graft healing are not considered in this study.
METHODS
The transplants were harvested from 13 fresh anatomy specimens (five female, eight male) which were then stored refrigerated without embalming fluid. They were all without macroscopic abnormality or previous ankle surgery. The mean age was 43 (19 to 61) years. Specimens with infectious diseases were excluded from the study. The mean height was 170 cm (SD 8.35; 157 to 186 cm), the mean body weight was 82 kg (SD 20.5, 63 to 140 kg). The respective transplants were obtained following the original description of the surgical procedures (Table 1). The anterior talofibular ligament was harvested as a bone-ligamen-tum-bone-complex. The specimens were wrapped in normal saline-soaked sponges and kept at 4°C until the experiment started. This was within 24 hours following the explantation. This avoided structural damage by deep freezing and limited the autolytic process of the tissue until mechanical testing. 19 The crossectional area of each specimen was determined as described by Lee and Woo 15 using a laser system (303 SP, LAP-inc., Lüneburg, Germany) at a wavelength of 670 nm. The smallest area of each specimen was used for subsequent analysis.
Biomechanical testing was performed on the most commonly used autogenous transplants for surgical ankle stabilization.
Biomechanical testing was performed using a universal testing device (Zwick 1445, Germany). We used a specially designed cylindric tissue clamp to obtain secure fixation of the transplants and to avoid mechanical tissue damage (Fig. 1). The testing started at 10 N to align the fibers at the clamps. 3 After determination of the length, the transplants were loaded until rupture at 10 mm per minute. During testing all data were continuously stored in a personal computer and subsequently analyzed in a statistics program (SPSS version 7.5, SPSS Inc., Chicago IL).
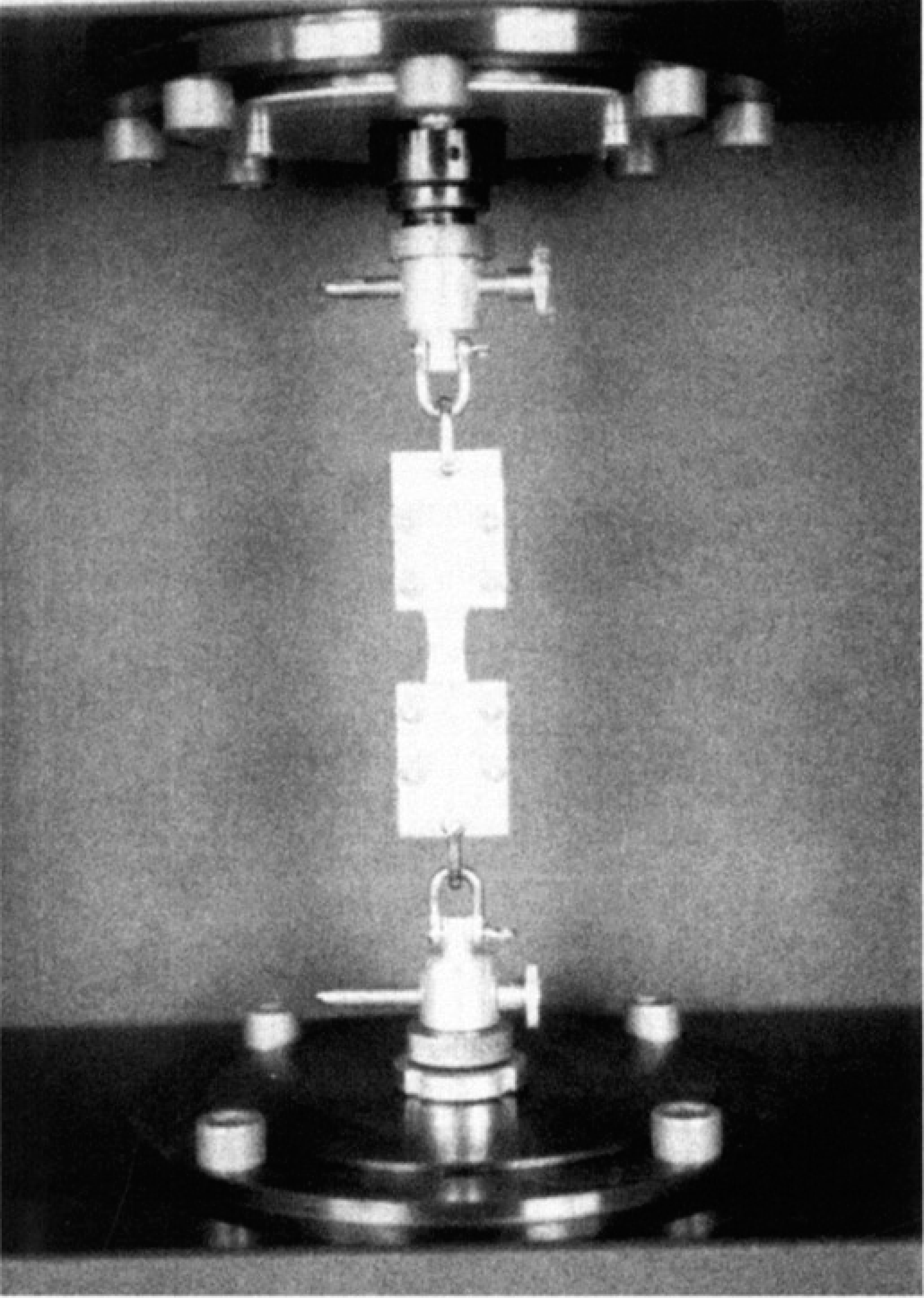
Biomechanical testing of an achilles split tendon autograft fixed in tendonclamps.
The biomechanical properties were calculated as follows 25 : The ultimate load (N) was defined as the maximum load before rupture is a biomechanical parameter to define the stability of the entire specimen (Fig. 2). The tensile strength (N/mm 2 ) characterizes tissue stability independent of its crossectional area (Fig. 3). Stiffness (N/mm) is defined as the load to lengthen the material 1 mm whereas the absorbed energy (J) is the total necessary energy until rupture. Ultimate strain (%) is a measurement of the elongation of the tested tissue until rupture related to its original length. The modulus of elasticity (N/mm 2 ) is lengthening divided by strain, i. e., the load per unit area, to lengthen the tested material.
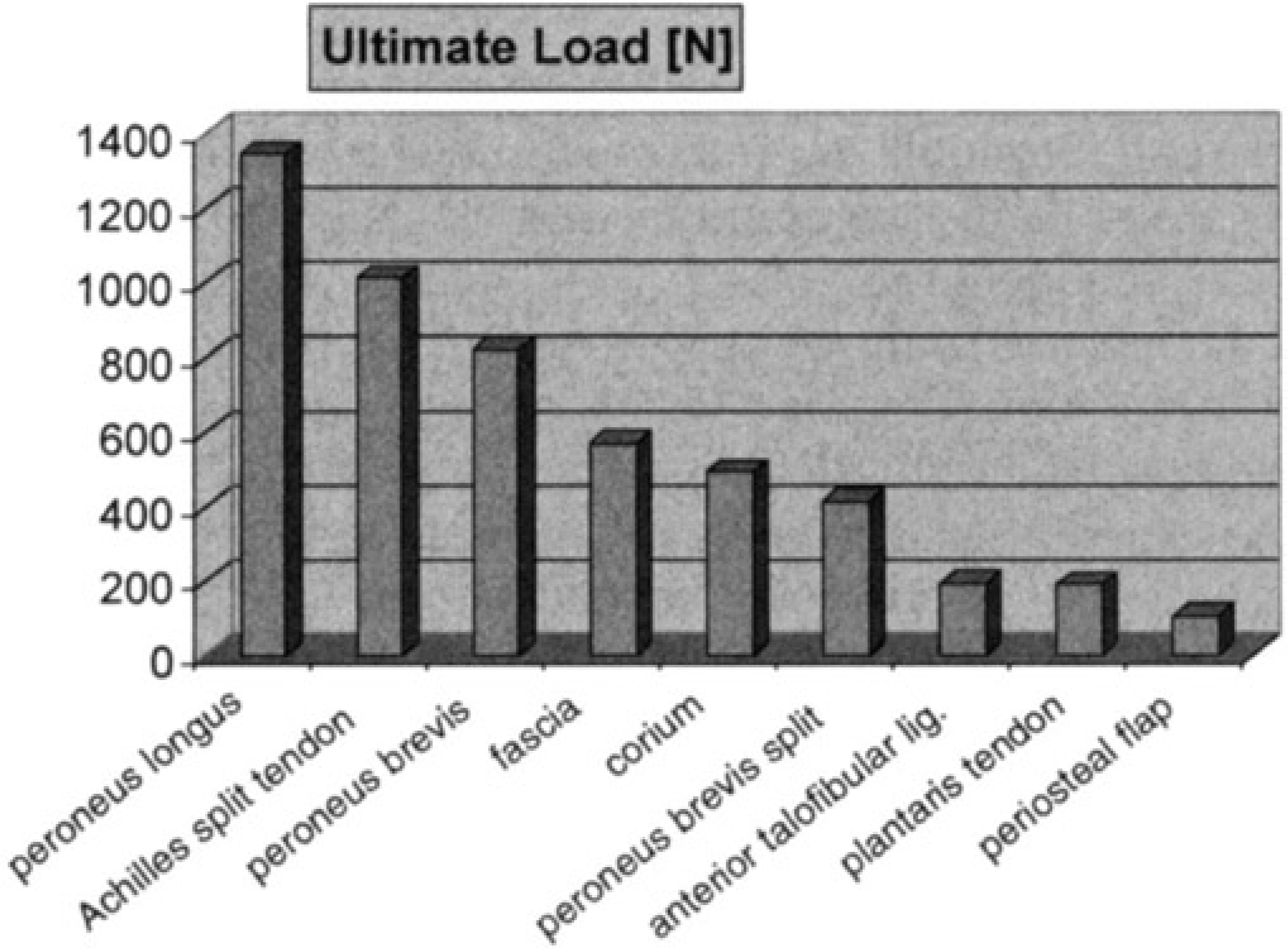
The mean ultimate load for each transplant at the biomechanical testing.
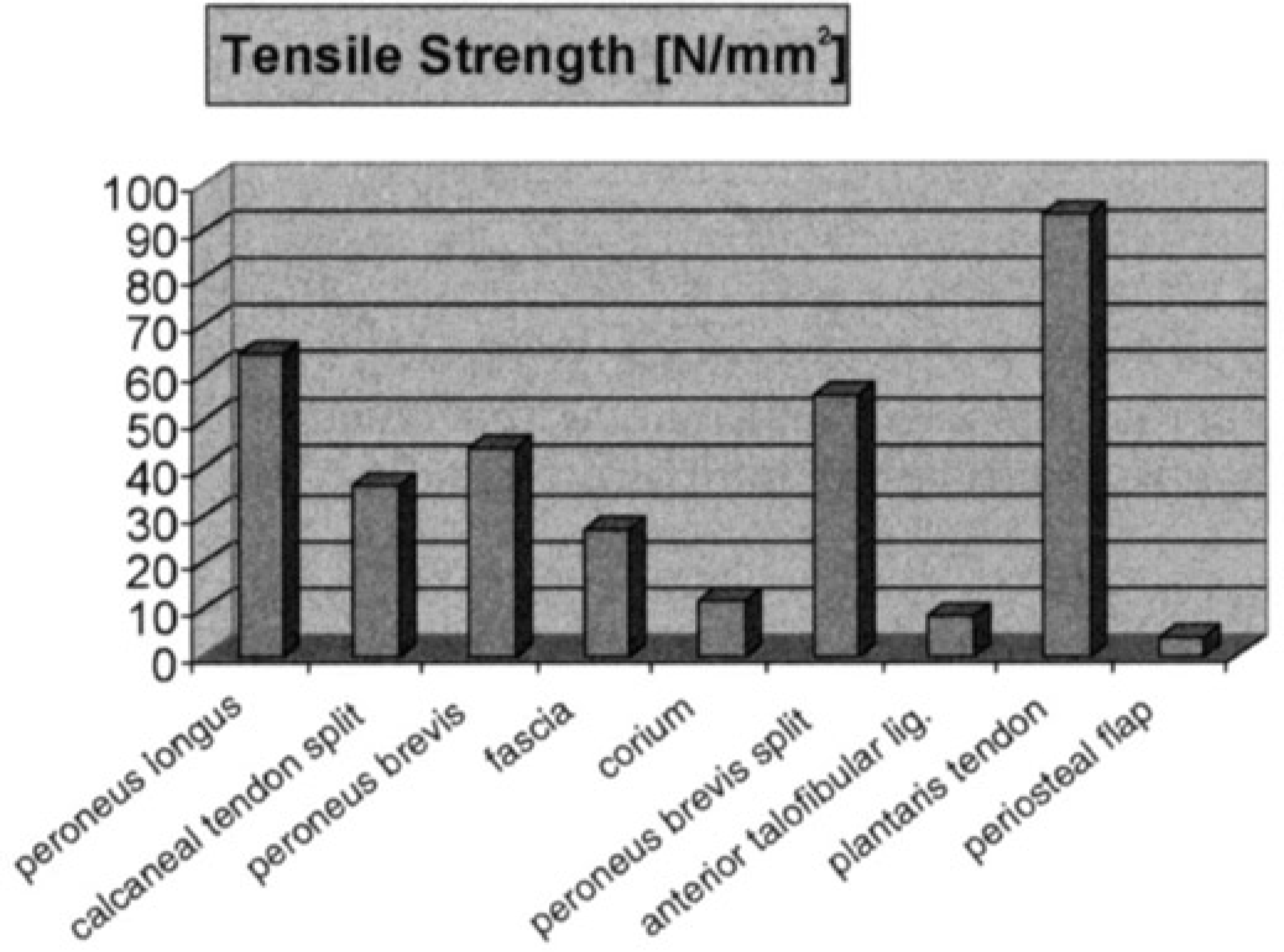
The mean tensile strength for each transplant (ultimate load correlated to the crossectional area).
RESULTS
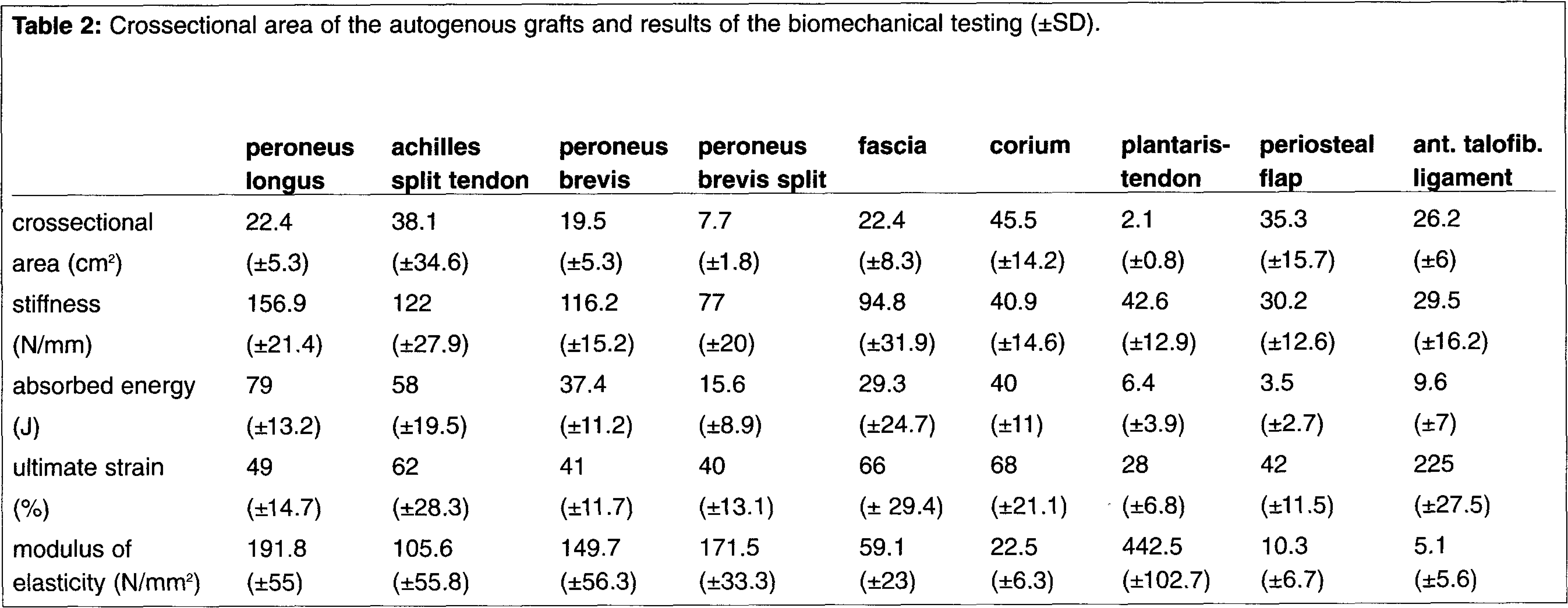
The peroneus longus tendon was the most stable autograft with an ultimate load of 1342±135 N (p = 0.003). The plantaris tendon had the highest tensile strength (93.8±14.9 N, p < 0.001). The peroneus brevis split tendon had only half the ultimate load but a higher tensile strength compared to the entire tendon, both transplants had a considerably higher biomechanical stability than the anterior talofibular ligament. The split achilles tendon had a high ultimate load (1013±278 N) and an intermediate tensile strength (35.9±11.3 N/mm 2 ) compared to the peroneal tendon grafts and the plantaris tendon. Fascia and corium had an intermediate ultimate load (569±265 N / 494±122 N) and a low tensile strength (26.8±11.2 N/mm 2 / 11.5±2.5 N/mm 2 ) compared to the tendon autografts. The biomechanical stability of the anterior talofibular ligament and the periosteal flap were significantly inferior to all the other tested specimens. Except the higher ultimate strain of 255±28% versus 42±12% (p < 0,001) there was no significant difference between the ligament and the periosteal flap for all evaluated biomechanical parameters. There was a significant negative correlation of age to the mean ultimate load (p = 0.031), the mean stiffness (p = 0.037) and the mean tensile strength (p = 0.016) of the periosteal flap. We found a significant positive correlation of the body height to the mean ultimate load (p = 0.019), the mean crossectional area (p = 0.025), the mean stiffness (p = 0.039) and the mean absorbed energy (p = 0.046) of the plantaris tendon.
The results of the biomechanical testing can be found in Table 2. There was no significant influence of the sex of the specimens on the biomechanical properties of the autografts.
Crossectional area of the autogenous grafts and results of the biomechanical testing (±SD).
DISCUSSION
The incidence of chronic symptoms after treatment of acute lateral ankle injuries is approximately 10% to 30%. 1,7,23 More than 50 different procedures for ankle ligament reconstruction have been described, which indicate that no single method has been entirely successful. 4,24 Anatomic reconstruction is favored against nonanatomic reconstruction by most authors as no functionally relevant tissue is sacrificed and no tenodesis effect is created. 2,10,12 This investigation describes the biomechanical tissue characteristics of the most commonly used autografts (Table 1).
We found the greatest biomechanical stability for the tendon specimens, especially the peroneus longus- and peroneus brevis tendon and the achilles split tendon. All had a much higher tensile strength and ultimate load than the anterior talofibular ligament. In comparison, the plantaris tendon had a much lower ultimate load whereas its tensile strength was high, due to its small crossectional area.
The biomechanical properties of the periosteal flap were inferior compared to tendon autografts, but there was no significant difference to the primary stability of the anterior talofibular ligament. The literature reports excellent or good clinical results in 73% to 90% for the anatomical reconstruction of lateral ankle ligaments using a regional periostal flap. 8,11,14,21,22 This is due to the histological transformation of the periosteum from a template to fibroblastic tissue replacing the ligament. 17 Therefore, in addition to the biomechanical properties, other things need to be evaluated for the selection of the appropriate procedure. The possible structural damage or functional deficit following the harvest of an autograft, the stability of the transplant fixation, and the biomechanical and histological changes during the transplant healing process all have to be taken into account.
If one uses a periosteal flap on grafts with low biomechanical stability we recommend postoperative immobilization in a strong in-shoe orthosis or a cast. This insures transplant healing by prevention of hindfoot inversion and limitation of ankle motion.