
Abstract
Twenty-four patients with displaced ankle fractures awaiting surgery were randomized to a study (n = 11) or a control group (n = 13). In the study group, patients had a pulsatile cold compression (PCC) device applied to their ankle, and remained at bed rest with the extremity elevated while awaiting surgery. In the control group patients remained in a posterior molded splint instead of the PCC device. Baseline circumferential measurements of the ankle were obtained, followed by measurements at 24-hour increments to evaluate edema resolution. In addition, patient satisfaction with use of the PCC device was evaluated with a scale ranging from 1 to 4. The median decrease of circumference in the study group compared to the control group was 0.5 cm vs. 0.1 cm at 24 hours (p=0.005), 0.9 cm vs. 0.4 cm at 48 hours (p<0.001), and 1.2 cm vs. 0.5 cm at 72 hours (p=0.009). The ratio of the decrease in circumference relative to the circumference of the normal ankle was significantly higher in the PCC group compared to the control group at all time points. All patients in the PCC group were satisfied with the device (median satisfaction score = 4). The PCC device was well tolerated and resulted in a significantly greater reduction of ankle circumference at 24, 48, and 72 hours after its application, compared to splinting and elevation alone. The PCC device facilitates edema resolution following ankle fractures.
INTRODUCTION
Soft tissue injury and swelling complicate all ankle fractures. The level of soft tissue swelling is often the determinant factor for the timing of open reduction and internal fixation (ORIF) of these fractures. Although in low-energy ankle fractures urgent surgery can be performed before swelling develops, it is not uncommon for the procedure to be delayed up to two weeks while awaiting edema resolution. It is vitally important for the surgeon to delay surgery until the swelling subsides sufficiently, since wound edge necrosis, skin slough, and postoperative infections can be the consequence of a prematurely performed ORIF. This is especially true in high-energy ankle fractures, where a compromised soft tissue envelope with extensive edema, fracture blisters, and ecchymosis may be present.
A number of interventions have been studied in an effort to expedite edema resolution. Cryotherapy and compression control edema, reduce pain, and their pre- and postoperative usefulness has been documented by several studies. 5,12,13,14,15 A device that combines pulsatile circumferential compression and cryotherapy, thus providing a theoretical advantage over simple ice packs and compressive splints, is available for use in ankle and foot trauma. The effectiveness of such a device for reducing postoperative edema and pain has been demonstrated after knee arthroscopic procedures and total joint replacement. 9,16,17 However, the concurrent use of intermittent pulsatile compression with cryotherapy for reduction of preoperative edema on ankle fractures has not been studied to our knowledge. Thus, the purpose of this study was to evaluate whether preoperative use of a pulsatile cold compression (PCC) device would facilitate resolution of edema after acute fractures of the ankle.
MATERIALS AND METHODS
Twenty-four patients were enrolled in the study. The PCC group consisted of 11 patients, eight male and three female with a mean age of 29 years. There were six Weber B and five Weber C fractures, which resulted from a sport injury in six cases, and a fall/twisting injury in five cases. The mean delay from the time of injury to enrollment was three days. The control group consisted of 13 patients, 10 male and three female with a mean age of 33 years, who sustained five Weber B fractures, five Weber C, 2 Weber A, and one medial malleolus fracture, following a sport injury in seven cases, a fall/twisting injury in three, a motor vehicle accident in two, and an assault in one case. The mean delay from the time of injury to enrollment was three days. Mean body weight was 76 kg in the PCC group and 73.5 kg in the control group and there was no significant difference in the circumference of the contralateral normal ankle between the PCC group (mean 22.5 cm) and the control group (mean 22.2 cm).
The inclusion criteria for the study were closed ankle fractures that required ORIF in adult patients. The exclusion criteria included unstable injuries (ankle fractures with greater than 1 cm lateral displacement of the talus or ankle dislocations) to minimize patient discomfort during measurements, open fractures, multiple trauma, pediatric patients, and cold intolerance. We also excluded patients with congestive heart failure, renal insufficiency, and lower extremity lymphedema to avoid the compounding effect of conditions predisposing to lower extremity edema.
Institutional Review Board approval was obtained. Upon signing the informed consent, patients were randomized into either a pulsatile cold compression (PCC) group or a control group. Randomization was performed by choosing a sealed envelope with the method of treatment enclosed. Patients in the PCC group were placed into a Cryo/Cuff compression device with an AutoChill pump (Aircast Incorporated, New Jersey) after removal of their long leg casts and remained at strict bed rest with the extremity elevated until surgery. The patients were not charged for the device, which was provided by the manufacturer. Patients in the control group remained in their bi-valved long leg cast and were otherwise similarly treated with bed rest and extremity elevation.
The Cryo/Cuff device is a gravity-controlled compression dressing attached to an ice-water cooler and an electrical pump (Fig. 1). The Cryo/Cuff cooler was lifted 15 inches above the ankle causing the compression dressing to fill with ice water and apply 30–35 mm Hg of compression of the foot and ankle. Once the Cryo/Cuff compression dressing was filled, the activated AutoChill pump provided a pulsatile effect by intermittently pumping the same volume of ice water in and out of the cuff while cooling the extremity to 50 to 60°F. To avoid the risk of localized frostbite, one layer of ABD dressing was applied around the ankle and foot. The ice water was changed every six to eight hours. The AutoChill pump remained on during the day and was turned off at night to allow the patient to sleep. The device was used in the PCC study group until the time of surgery.

A photograph of a patient's foot with the Cryo/Cuff compression dressing applied. The device is attached to an ice-water cooler and the AutoChill pump.
Data collection for both groups included measurements of ankle circumference using a standardized technique to minimize errors. A circumferential mark was made with an indelible black marker 5 cm proximal to the medial malleolus to ensure a consistent location for measurements. A measuring tape was placed such that its upper edge was in contact with the circumferential mark. Baseline circumferential ankle measurements of the affected extremity were made at the time of enrollment (day zero), and every 24 hours thereafter (day one, day two, day three) until surgery. We found this technique to be reliable, since measurements performed by two observers were found to be in agreement, and we preferred it to volume displacement measurements in order to minimize patient discomfort. A satisfaction score was documented before every measurement based on a scale ranging from 1 to 4 with 4 being very satisfied, 3 satisfied, 2 dissatisfied, and 1 very dissatisfied.
Median changes between day zero (baseline) and each of the subsequent days were compared between the two groups, using the Mann-Whitney U test for the statistical analysis, since data were not normally distributed. All tests were two-sided and significance was set at p<0.05.
RESULTS
The Cryo/Cuff device with the AutoChill pump was well tolerated by all PCC study patients, who were all satisfied or very satisfied with the device. The median satisfaction score was 4. Specifically, seven patients (64%) were very satisfied and four (36%) were satisfied. No patient in the PCC group had any complaint or complication associated with the device. All patients stated they preferred the PCC device to the plaster long leg splint, which had been worn prior to study enrollment, due to its compactness and light weight.
On average, patients were evaluated four times, with one baseline and three additional measurements before surgery. Two patients in each group did not complete the day three measurements because they underwent surgery before this time point.
The median differences in ankle circumference between day zero and subsequent time points (day one, day two, and day three) for the two groups are presented in Table 1. At day one there was a median circumference decrease of 0.5 cm in the PCC group, compared to a decrease of 0.1 cm in the control group. The difference was statistically significant (p=0.005, Mann Whitney U test). At day two, the median decrease in circumference was 0.9 cm vs. 0.4 cm (p<0.001, Mann Whitney U test). Similarly at day three, a statistically greater reduction of ankle circumference was observed in the PCC group (1.2 cm vs. 0.5 cm, p=0.009, Mann Whitney U test). In addition, the ratio of the decrease in circumference relative to the circumference of the normal ankle was significantly higher in the PCC group compared to the control group at all time points (Table 1).
Median ankle circumference decrease (in cm) and ratio of decrease relative to the normal ankle circumference at 24-hour intervals in the pulsatile cold compression (PCC) and the control group.
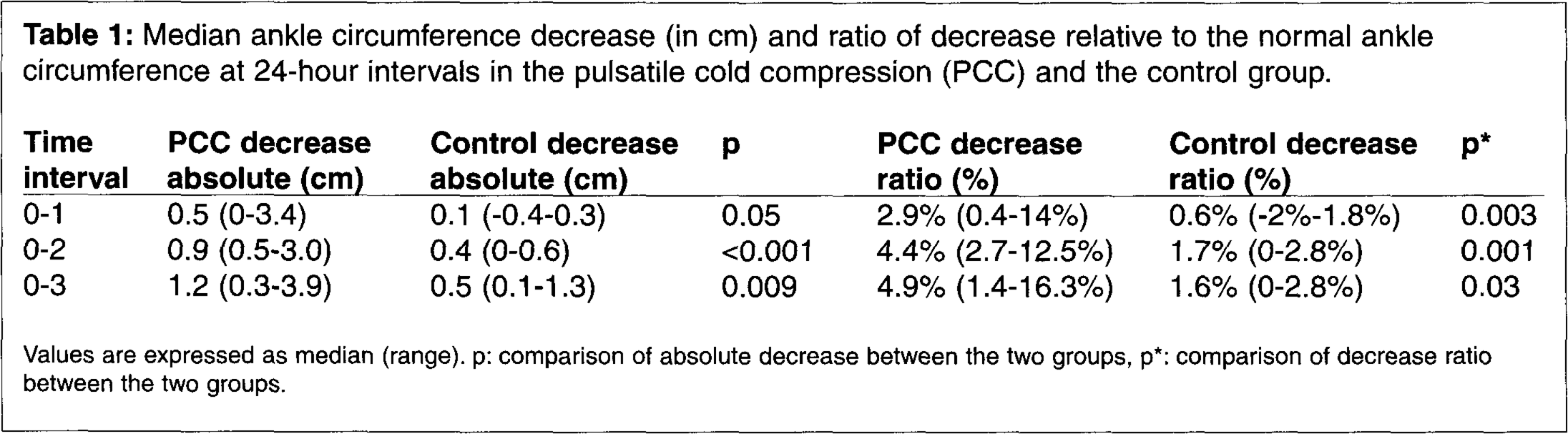
Values are expressed as median (range). p: comparison of absolute decrease between the two groups, p*: comparison of decrease ratio between the two groups.
DISCUSSION
Cryotherapy and the application of compression have been used in the initial management of acute injuries. Musculoskeletal trauma is followed by the immediate release of vasodilators and inflammatory precursors that result in the clinical findings of swelling, increased warmth, pain, and edema.
Cryotherapy lowers the temperature at the injury site and results in capillary constriction. Thus, it decreases permeability, hemorrhage, tissue metabolism, and reduces the adverse sequelae of musculoskeletal trauma. 3,11 In addition, cryotherapy impedes pain signal transmission from injured muscle and decreases spasm by dampening the responsiveness of muscle spindles. 3,7,11 The postoperative benefits of cryotherapy have been documented in clinical studies. 9,16,17 Levy and Marmar in a prospective randomized study reported a reduction in blood loss, swelling, analgesic use, and improvement of range of motion following total knee replacements. 9 Webb et al. observed an improvement in postoperative blood loss and pain control but with no influence in swelling after total knee arthroplasty. 16 Whitelaw et al. in a prospective randomized study, found less analgesic use in a group of patients using a cryotherapy device vs. an elastic bandage and ice following knee arthroscopy. 17 These studies used similar Cryo/Cuff compressive devices for the knee but did not add the intermittent pulsatile function.
The addition of compression augments the effectiveness of cryotherapy by increasing the extracellular hydrostatic pressure, thus decreasing edema formation. Pedal compression devices have been used for both deep venous thrombosis prevention and edema control. 2 These devices increase the venous and lymph return from the extremity by intermittently compressing, or “pumping,” the plantar venous plexus of the foot. Additionally, the release of endothelial relaxing factors is thought to play a role in relieving pain and decreasing venous congestion. 4,12 The benefits of intermittent pedal compression without the use of cryotherapy for the preoperative treatment of foot and ankle fractures has been investigated in two prospective randomized trials by Thordarson et al. 14,15 In both studies, a significant decrease in edema was documented in patients with operative ankle and calcaneus fractures awaiting surgery and rebound edema, a potential complication of rapid edema resolution, was not a problem. Other authors have similarly found pedal compression to be effective in relieving edema following foot and ankle trauma. 5,12 Stockle et al. compared compression vs. cryotherapy and observed that intermittent pedal compression reduced edema faster compared to continuous cryotherapy or ice packs. 13
This study is the first, to our knowledge, to evaluate the role of cryotherapy combined with intermittent pulsatile compression in edema resolution in operative ankle fractures. A significantly greater decrease in ankle circumference at 24, 48, and 72 hours after application of the device was observed, compared to a splint and elevation alone. The device was well tolerated by all patients and all patients were satisfied.
Our study only investigated the effectiveness of pulsatile cold compression in edema resolution and did not evaluate if the reduction in swelling resulted in any clinical benefit. Further clinical evaluations are necessary to determine the potential impact on clinical outcome with the more rapid edema resolution. It can be argued that although the Cryo/Cuff device improved edema resolution, the additional circumference reduction compared to the control group was small and measured 0.4 cm, 0.5 cm, and 0.7 cm at 24, 48, and 72 hours, respectively. However, the device was applied at a mean time of three days following injury due to late patient presentation to our institution, thus missing the opportunity to reduce edema formation immediately following injury. Despite the delay in application, pulsatile cold compression was able to improve edema resolution. We hypothesize that more timely application would result in a greater improvement. In our study we did not include high-energy ankle fracture-dislocations. Measurements would be uncomfortable and inclusion of these fractures would lead to a non-homogeneous group of fractures. However, in high-energy fractures that are associated with increased swelling the device could prove even more useful. Further studies are needed to evaluate if PCC application, especially in the immediate post injury period would allow for greater reduction in swelling.
It should be noted that discharging patients in a compressive, posterior splint with instructions for rest and elevation and having them return when their swelling has subsided is the standard practice in the community, and hospitalization is not necessary. However, in our institution the high volume of patients prevents immediate surgery, and many patients do not have the social and financial resources to remain compliant with instructions following discharge.
The limitations of the device studied include its requirement for ice water changes every six to eight hours, the availability of only a “one-size-fits-all” compression dressing that may not conform on all of the patients' extremities, and the application of compression preferentially over the dorsum of the foot and ankle compared to the plantar aspect of the foot. The Cryo/Cuff device has a limited capacity for immobilizing fractures, so its use should be restricted to more stable patterns of injury. Moreover, the cost of the Cryo/Cuff with the AutoChill system is approximately $150.00. 17
In summary, we found that the Cryo/Cuff compression dressing and AutoChill system significantly decreased edema in ankle fractures before surgery compared to splintage and elevation alone. In addition, all patients tolerated the device well and were satisfied with it.