
Abstract
The records of 104 patients who underwent reconstructive foot and ankle surgery for deformities secondary to rheumatoid arthritis were reviewed. The use of rheumatoid chemotherapeutic agents, age, sex, rheumatoid nodule status, and the number of concurrent surgical procedures performed was analyzed to determine any association with the postoperative outcome for wound healing and infectious complications. The 104 patients, ranging in age from 23 to 83 years, underwent 725 operative procedures. An overall 32% complication rate was recorded. Analysis of five specific rheumatoid chemotherapeutic agents (NSAIDs, steroids, methotrexate, hydroxychloroquine, gold), age, sex, number of operative procedures performed, and presence of rheumatoid nodules, either alone or in combination, failed to prove a statistical association with either a healing or infectious postoperative complication.
INTRODUCTION
Poor healing and infection are among the most dreaded complications for orthopaedic surgeons, and all too often associated with prolonged and serious morbidity. Rheumatoid arthritis patients are a select subset of patients who, by nature of their disease process and its medical management, have been long thought of being relatively compromised hosts that are at particular risk for postoperative infectious and wound healing complications. The foot and ankle deformities that result from the rheumatoid disease process very often require extensive simultaneous procedures to achieve balanced, long-lasting corrections (Figs. 1a, 1b). The purpose of this study is to evaluate the influence of several common anti-rheumatoid medications, patient age, sex, and the presence of rheumatoid nodules on postoperative healing and infectious complications in rheumatoid arthritis patients undergoing reconstructive foot and ankle surgery.

Preoperative photograph of forefoot deformities and multiple incisions required in a 65-year-old patient with rheumatoid arthritis. Operative soft tissue dissection is often extensive for the confines of the foot and ankle.

Postoperative photograph of same patient as in Figure 1a. Despite the use of multiple rheumatoid chemotherapeutic agents in the perioperative period, the postoperative course was without complications.
MATERIALS AND METHODS
This study was reviewed and approved by the Institutional Review Board. The medical record database was searched for patients with a diagnosis of rheumatoid arthritis, and cross-matched for patients who underwent foot and ankle surgery for a consecutive 10-year period. Demographic data collected included patient age, sex, and presence of comorbid medical conditions, such as diabetes, neuropathy and peripheral vascular disease, the presence of which were designated as exclusion criteria, by virtue of being confounding variables for this study. This data search, retrieval and exclusion process yielded records available for review and analysis in 104 patients.
Charts were reviewed for the number of individual procedures, the number of and the specific anti-rheumatoid arthritis chemotherapeutic agents in use in the immediate perioperative period, the presence of rheumatoid nodules, as well as the outcome after surgery. The outcomes analyzed were the occurrence of operative site infection and wound healing difficulties. Infection was broadly categorized as critical for an adverse outcome, which included either a microbiologically diagnosed infection, or a presumptive clinical diagnosis, based on wound drainage, erythema, pain, and laboratory evidence of a postoperative infection (persistent elevation of WBC, C-reactive protein). Superficial and deep infections (below fascial layer) were summed together. Healing problems included any difficulties with wound healing, ranging from simple delays in wound healing (surgical wounds not healed by three weeks) to a wound slough, as well as any osseous healing problems.
Patient profile data was analyzed by descriptive statistics. Patients were stratified into two outcome groups: those who did not experience a postoperative complication (Group 1), and those who experienced a postoperative complication (infection, wound problem, other) (Group 2). Chi-Square and the Fisher exact test were employed to statistically analyze nominal variables between patient groups. Variables examined included age, sex, the type and number of rheumatoid chemotherapeutic agents in use during the perioperative period, the presence of rheumatoid nodules, and the occurrence of a postoperative complication. Analysis of the influence of multiple variables on the postoperative outcome was analyzed via a logistic regression model. A statistician using SAS computer programs (Carey, NC) analyzed the collected data.
RESULTS
One hundred and four patients satisfied the study inclusion criteria. Eighty-seven patients were female, 17 were male, ranging in age from 23 to 83 years of age. Seventy-one patients did not experience a complication (68%) and were assigned to Group 1. Thirty-three patients experienced a complication (32%) and were assigned to Group 2. Thus, an overall 32% patient complication rate was observed. Among these 104 patients, a total of 725 operative procedures were performed, yielding a 5% complication per procedure rate. Chi Square analysis demonstrated no statistical difference between Groups 1 and 2 in regard to the mean age, sex distribution, number of surgical procedures, frequency of rheumatoid nodules, or number of medications used in the perioperative period (Table 1).
Comparison of Group 1 (No Postoperative Complications) and Group 2 (Postoperative Complications) Patients

statistical significance considered at p≤0.05; results are not statistically significant
SD=standard deviation
Group 1 (no complications group) consisted of 71 patients, 60 females and 11 males. The mean age of Group 1 patients was 53 years (range, 23–82). Females averaged 52 years (range, 23 to 79), while the male age averaged 56 years (range, 29 to 82). Rheumatoid nodules were present in 32 patients (45%). A mean of two anti-rheumatoid arthritis medications was actively administered in this group without complications. A total of 467 procedures were performed in this group, averaging 6.6 procedures per patient (Table 2).
Characteristics of Group 1 (No Postoperative Complications Group) and Group 2 (Postoperative Complications) †

P=0.6727, Fisher exact test, no statistical difference in demographics between groups
F=female; M=male; Rh nodule=rheumatoid nodule
Group 2 (complications group) was comprised of 33 patients, with mean age of 58 years (range, 30 to 79). Females (n=27) had a mean age of 60 years (range, 30 to 79), while males (n=6) had a mean age of 52 years (range, 57 to 75). A mean number of two anti-rheumatoid arthritis medications were actively administered perioperatively in Group 2. Thirteen patients (39%) possessed rheumatoid nodules. A total of 258 procedures were performed in this group, averaging eight procedures per patient. A total of 42 individual complications occurred in these 33 patients (mean of 1.3 complications per Group 2 patient) (Table 2). In group 2, there were 16 infections: 14 superficial and two deep. Ninety-four percent of infections responded to oral antibiotics or parenteral antibiotics with debridement. There were 23 healing complications: 19 with a delayed healing of the surgical incision, and four arthrodesis nonunions (two ankle nonunions, two forefoot nonunions). Three nonunions were painless, and required bracing and symptomatic treatment. One recalcitrant infected ankle nonunion required a below knee amputation. There were no wound sloughs. The remaining three complications consisted of one sural neuroma, one hematoma, and one recurrence of a rheumatoid nodule.
Accurate records for rheumatoid chemotherapy were available in 67/71 patients in Group 1 (94%), and for 31/33 Group 2 patients (94%). Five anti-rheumatoid arthritis medications were identified as being administered to a sufficient number of patients to facilitate statistical analysis. These medications included the nonsteroidal anti-inflammatories (NSAIDs), steroids, methotrexate, hydroxychloroquine and gold. Statistically, there was no difference between Groups 1 and 2 regarding the perioperative administration of all of these medications. Combination pharmacotherapy (greater than one agent) did not prove to statistically increase the risk of a complication (Table 3). An insufficient number of patients were receiving tumor necrosis factor-α (TNF-α) inhibition therapy (etanercept [Enbrel®], infliximab [Remicade®]) in the current study to allow meaningful analysis.
Rheumatoid Chemotherapeutic Agents

statistical significance considered at p≤0.05; results are not statistically significant
NSAIDs=nonsteroidal anti-inflammatory agents
The number of surgical procedures performed per patient did not pose a statistically significant increased risk for a complication (p=0.126, Fisher exact test). The difference in frequency of rheumatoid nodules between Groups 1 and 2 was also not statistically significant (p=0.6727, Fisher exact test).
Logistic analysis of age greater than 55 plus any of the three most common medications or the presence of rheumatoid nodules demonstrated no statistical significance of the factors toward the development of a complication (Table 4).
Analysis of Multiple Variables on Outcome Groups
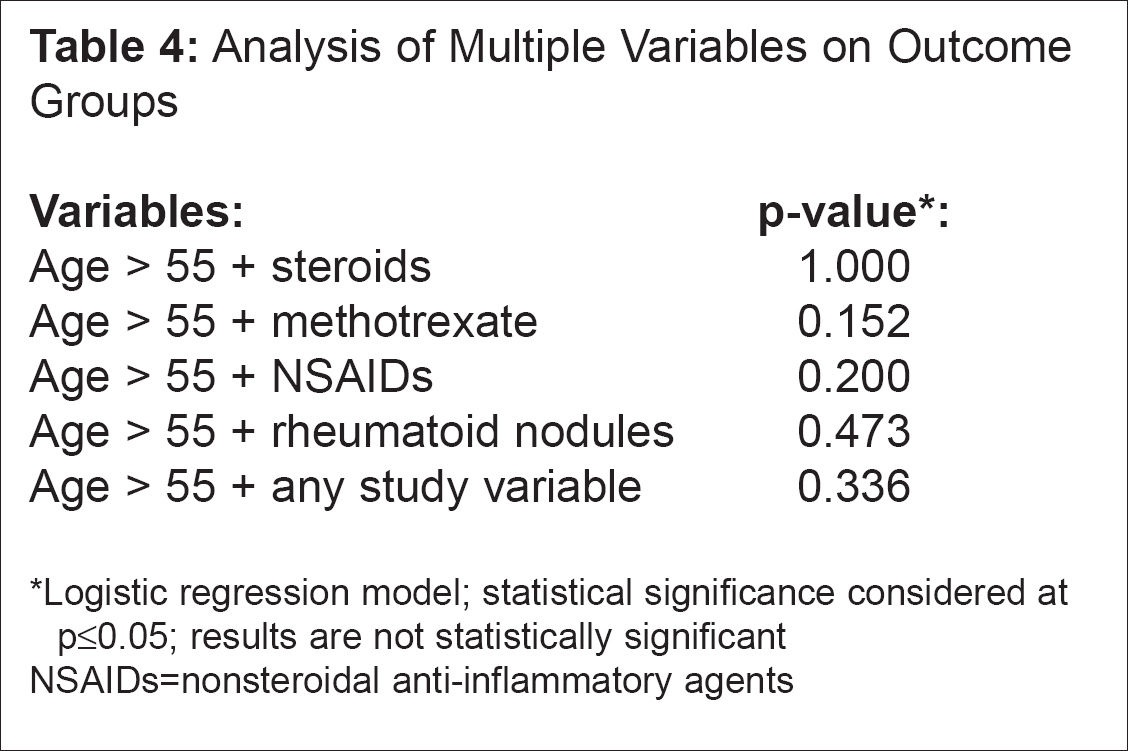
Logistic regression model; statistical significance considered at p≤0.05; results are not statistically significant
NSAIDs=nonsteroidal anti-inflammatory agents
DISCUSSION
Rheumatoid arthritis affects approximately 0.3 to 1.5% of the North American population, with a peak incidence within the fourth to sixth decades. 6 Many patients with rheumatoid arthritis suffer from crippling deformities of the foot and ankle. To obtain long-lasting, balanced correction, these patients often require a large number of operative procedures during a single surgical setting. Furthermore, foot and ankle operative procedures often require multiple incisions and soft tissue dissections without the luxury of large bridges of undisturbed soft tissue planes, which carry inherent risks for healing complications (Figs. 1a, 1b). Thus, traditional teaching has been the voice of limiting dissections as well as the number of simultaneous regional procedures. Rheumatoid arthritis patients have also been long regarded as relatively compromised and prone to postoperative infectious and wound healing complications. 1,2,8,14,16,19 This belief is in part due to the use of a large number of rheumatoid chemotherapeutic agents that by virtue of their anti-inflammatory effect results in a blunting of the normal immune response required for wound healing, 13 the inhibition of collagen synthesis, and lowered infectious surveillance. 13 In particular, steroids, methotrexate, D-penicillamine, cyclophosphamide, azathioprine, cyclosporine, and enantercept have been implicated as agents that contribute to postoperative complications. 16,19,21 Laboratory evidence also exists for a potential role of several NSAIDs contributing to conditions that could result in a delay in wound healing. 12 Clinically, reports pertaining to the increased risk of postoperative complications posed by anti-rheumatoid arthritis medications are variable. Several recent reports have examined the risk posed by continued perioperative methotrexate therapy. These studies have focused on hip, knee and hand surgery, and lend support in favor of not discontinuing methotrexate in the perioperative period. 7,9,17,18 There is little data pertaining to postoperative complications in foot and ankle surgery during continuous perioperative rheumatoid chemotherapy. The present study expands on these data, providing evidence that methotrexate, steroids, NSAIDs, gold, or hydroxychloroquine, alone or in combination, do not pose an increased risk for postoperative infectious or healing complications in foot and ankle surgery (Table 3). In our study population, insufficient numbers of patients were receiving TNF-α inhibition therapy for valid analysis. A study specifically addressing TNF-α inhibition therapy and postoperative complications is currently being performed at the lead author's institution.
Advancing age has been thought to adversely impact wound healing, 3,4,5,15 posing a theoretical compounded risk to postoperative complications in rheumatoid arthritis patients. Our data did not identify age as a risk for a postoperative complication. Moreover, logistic regression analysis failed to identify any combinations of variables (age, rheumatoid chemotherapy agent, rheumatoid nodules) to be statistically associated with increased risk for the development of a postoperative healing or infectious complication (Table 4).
Rheumatoid nodules are reported to be present in approximately 20% of patients, and are thought to be a marker of more advanced clinical disease (Clinical Progression Stage III). 10 Rheumatoid nodules are the result of a local vasculitic process, 20 thus, may be interpreted as a signal to the potential for postoperative wound healing difficulties. 11 We found that rheumatoid nodules were present overall in 43% of patients. The difference in frequency of rheumatoid nodules between Groups 1 and 2 was not statistically significant (p=0.6727, Fisher exact test) and therefore, in our estimation, was not a reliable clinical predictor for the development of postoperative complications. However, in our study population, the group experiencing no complications had a slightly higher incidence of rheumatoid nodules than did the group of patients experiencing a complication (36% vs. 29%, respectively). Additionally, even an age greater than 55 plus the presence of rheumatoid nodules did not increase the risk for a postoperative complication.
CONCLUSION
Based on our data, we conclude that the use of methotrexate, steroids, NSAIDs, gold, or hydroxychloroquine do not contribute to the development of postoperative healing and infectious complications in rheumatoid arthritis patients undergoing reconstructive foot and ankle surgery. Thus, the administration of these agents may be safely undertaken in the perioperative period. Further, we found that age, sex and the presence of rheumatoid nodules, either alone, or in conjunction with the above named medications, not to be predictive of a postoperative healing or infectious complication after rheumatoid foot and ankle surgery. The overall complication rate (32%) in this series of rheumatoid arthritis patients was high, and does point to a word of caution in surgically managing rheumatoid arthritis patients. Ostensibly, the rheumatoid arthritis disease process imparts an intrinsic liability to complications as compared to the “normal population”; however, the risk factors examined in this study did not prove to be statically associated with an increased risk for complications. Finally, based on our data, we believe that extensive foot and ankle reconstructive efforts may be safely undertaken in rheumatoid arthritis patients taking multiple rheumatoid chemotherapeutic agents without appreciably increasing the risk of healing or infectious complications.