
Abstract
The objective of this study was to determine in healthy individuals whether the Bledsoe Diabetic Conformer Boot reduces plantar pressures as well as a fiberglass total contact cast. Eighteen normal subjects, without any prior foot or ankle problems, were recruited for this study. Plantar pressures were measured using the Novel Pedar™ in-shoe pressure measurement system. The results of this study demonstrate that in individuals without foot deformities, the Bledsoe Diabetic Conformer Boot™ performs as well as, and in many parameters, even better than a fiberglass total contact cast with respect to reducing the forces and pressures on the plantar surface of the foot.
INTRODUCTION
The total contact cast (TCC) has been the standard for treating plantar foot ulcerations for a number of years. Several studies have shown that the TCC is a safe and reliable method for successful treatment of plantar ulcers. 3,8,15,16,18,20 There are several theories for the mechanisms of a TCC, but the most widely accepted rationale is that total contact casts reduce pressure over the wound by redistributing the weightbearing load over a greater plantar surface area.
Two studies 14 examined plantar pressures in casts on subjects with diabetes. The conclusion of these studies was that casts function by increasing the plantar weightbearing surface area, thereby lowering plantar pressures over any one particular area. Both short leg casts and TCCs reduced midfoot pressures, but only the TCC significantly lowered forefoot pressures. Neither type of cast reduced heel pressure significantly.
One major advantage of a TCC is that patient compliance is almost guaranteed, since removal of the cast is very difficult. However, TCCs are not entirely free of risks and complications, which include new ulcerations and areas of skin breakdown. There are many versions of the TCC and there is little consensus on what actually constitutes a total contact cast. In essence, it is a minimally padded version of the below-knee or “short leg cast,” and in which the toes are either padded or enclosed.
Removable walking boots have slowly been introduced into the diabetic ulcer-healing regimen in part to address some of these concerns and challenges with TCC. There are advantages to a removable walking boot which includes easier, less intimidating application, and less training time for medical personnel. The major disadvantage of removable walking boots is the uncertainty about whether the patient is consistently wearing the device.
Several recent studies have compared these removable walkers to TCC. A study in 1997 by Baumhauer 3 and colleagues tested the Aircast Pneumatic Walker™ against a total contact cast. The researchers measured plantar pressures during walking of 12 healthy subjects. They used force-sensing resistors over five distinct locations (first, third, and fifth metatarsal heads, fifth metatarsal base, and midheel) under the foot to quantify pressure. The authors concluded that the Aircast Walker effectively decreased peak plantar pressures and pressure-time integrals over all five locations under the foot at least as well as or better than the TCC. However, the authors only measured plantar pressures in five distinct locations under the foot, and reproduction of their results is prevented by the nature of the force-sensing resistor technology that restricts quantitative measurement. 19 In 1999, Armstrong and Stacpoole-Shea 2 compared a TCC against the Aircast Pneumatic Walker™ and the Centec DH Pressure Relief Walker™. They tested 25 patients with diabetes using the Novel Pedar™ in-shoe pressure measurement system. Researchers found that the TCC reduced peak pressures significantly better than the two removable walkers, but that the Centec walker performed better than the TCC and the Aircast walker in reducing pressure-time integrals. The pressure-time integral incorporates both impulse and contact area in one equation, and a 1999 study by Sauseng et al. 17 concluded that pressure-time integrals appear to be a valuable parameter for estimating the risk of ulceration in patients with diabetes.
The objective of this study was to evaluate in normal subjects the effectiveness of the Bledsoe Diabetic Conformer Boot™ in reduction of plantar pressures as compared to our technique of the TCC.
METHODS AND MATERIALS
Eighteen normal subjects, without any prior foot or ankle problems, were recruited for this study. There were seven females and 11 males, with an average weight of 85.6±21.9 kg and an average height of 176.5±12.7 cm. Plantar pressures were measured using the Novel Pedar™ in-shoe pressure measurement system (Novel, GMBH, Munich, Germany). Data were collected at 50 Hz using 2 mm thick capacitance insoles with 99 sensors per insole. Each insole also has an approximate sensor resolution of 1 sensor/cm 2 , which is dependent on the insole size. The same Pedar insole was placed inside of both the cast and the boot in any given individual.
The pressure maps of each insole were divided into three regions called masks: hindfoot, midfoot, and forefoot. Peak plantar pressure, maximum plantar force, average plantar pressure, plantar contact area, plantar contact time and pressure-time integral were analyzed in each foot and in each foot region defined by the masks.
Each subject walked with the Bledsoe Diabetic Conformer Boot™ (Fig. 1) and a TCC with a cast shoe (Fig. 2). The Conformer Diabetic Boot (Bledsoe Brace Systems, Grand Prairie, TX) is specifically designed for diabetic patients with plantar ulcerations. The device is designed to wrap the foot in a fully enclosed thick foam cocoon, which is placed onto an auto-molding innersole. This innersole embeds into a specially designed pre-molded mid-sole insert inside an aluminum-shell walking boot. Bledsoe Brace Systems only participation in the study involved providing the walking boots free of charge. The TCCs were all administered by the same casting technician using the same technique employed in our clinic to treat plantar diabetic ulcers of the forefoot. The procedure consists of the following: A 3-inch closely fitting cotton stockinet is rolled from below the toes to just below the knee. Wrinkles that develop in the stockinet at the dorsum of the ankle are eliminated by a slit cut from malleolus to malleolus. Two layers of cast padding are applied over the foot, ankle and leg, with felt padding applied over the anterior tibial crest and the malleoli. The cast is applied from just below the tibial tubercle to the tips of the toes, while holding the ankle, hindfoot, and MTP joints in neutral position. This is done with four-inch rolls of Delta-Lite Conformable Casting Tape™ (Johnson & Johnson). Once the fiberglass has dried completely, a cast shoe is attached to the bottom of the cast (Texas Orthopaedic Products and Services, Rowlett, TX). The Pedar™ insoles were placed directly adjacent to the skin of the foot in both the boot and TCC.

The Bledsoe Diabetic Conformer Boot.

Fiberglass Total Contact Cast with cast shoe. The wire coming out from the top of the cast is connected to the Pedar insole inside the cast.
The subjects were randomly assigned to the order of testing for the two conditions. The subjects were initially allowed to walk with each device, the total contact cast, and the Conformer Walking Boot™ until they felt acclimated to the device. They then walked at a self-selected speed down a 10-meter walkway several times and 20 to 25 steps for each condition (cast vs. Boot) were collected for averaging and statistical analysis. Statistically, paired t-tests were used to compare between the results of the cast trial and the boot trial. An alpha level of 0.05 was used for all statistical tests.
RESULTS
The total contact times in the total contact cast (736.5±88.8 msec) and boot (725.8±101.5 msec) were no different, which translates to similar walking velocities for the two conditions. The total contact area was slightly increased in the boot (153.1±34.6 cm 2 ) as compared to the cast (148.2±33.5 cm 2 ), but this was not statistically significant.
The maximum force (Fig. 3) was significantly reduced in the boot as compared to the cast under the forefoot by 21%, p=0.008 (353.5±124.7 N vs. 446.9±184.0 N). The maximum mean pressure (Fig. 4) was consistently lower in the boot, but not statistically significant.

Graph depicting the maximum force under the three mask regions as well as the entire foot, with the fiberglass cast (white bars) and the Bledsoe Diabetic Conformer Boot (black bars).
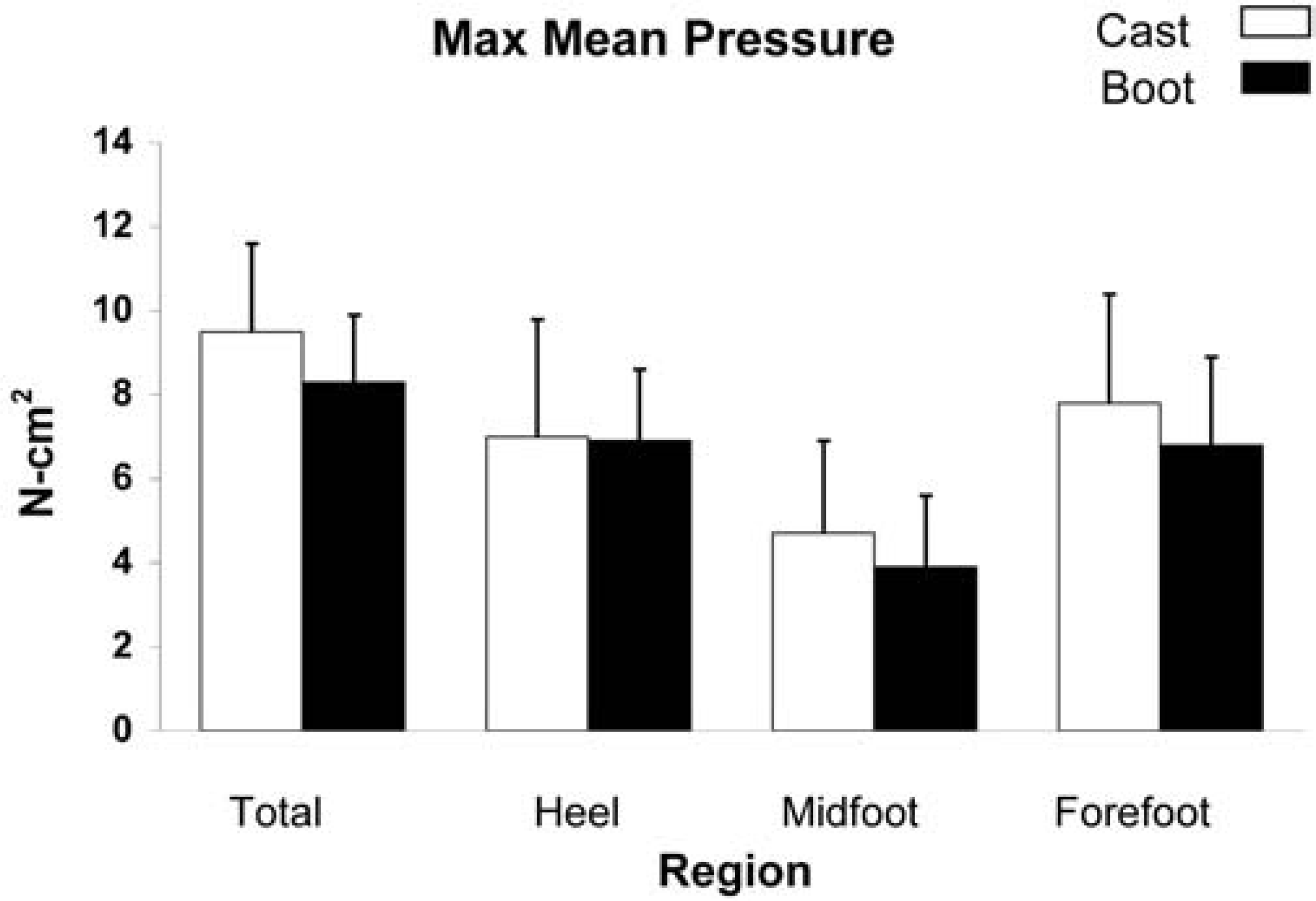
Graph depicting the maximum mean pressure under the three mask regions as well as the entire foot, with the fiberglass cast (white bars) and the Bledsoe Diabetic Conformer Boot (black bars).
The peak pressure was significantly reduced in the boot as compared to the cast in the forefoot (p=0.00002) as well as the foot as a whole (p=0.00001) (Fig. 5). The total peak plantar pressure was reduced on average by one-third in the boot as compared to the cast. Pressure-time integrals (Fig. 6) were also significantly reduced in the boot as compared to the cast under the total foot, p=0.0005 (7.2±1.6 N-sec/cm 2 vs. 8.9±2.1 N-sec/cm 2 ) and under the forefoot, p=0.04 (5.1±1.4 N-sec/cm 2 vs. 6.1±2.2 N-sec/cm 2 ).

Graph depicting the peak pressure under the three mask regions as well as the entire foot, with the fiberglass cast (white bars) and the Bledsoe Diabetic Conformer Boot (black bars).

Graph depicting the Pressure-Time Integral under the three mask regions as well as the entire foot, with the fiberglass cast (white bars) and the Bledsoe Diabetic Conformer Boot (black bars).
DISCUSSION
This study compared the effect of a new diabetic walking boot on the reduction of plantar pressures in the foot compared to a total contact cast in healthy individuals. Walking velocity was not controlled in this study, which could have been a variable for plantar pressures; however, the results demonstrated that the total contact times in the two conditions were similar, indicating that this was not a factor. Even though the difference in the total contact area, which was slightly increased in the boot, was not significant, the addition of the measuring PEDAR insole may have reduced the effect of the auto-mold material in the walking boots, reducing the true contact area, thus possibly underestimating the diminution in pressure in the boot.
The peak pressure, maximum force, and pressure-time integrals were all reduced in the boot as compared to the cast, at statistically significant levels. These reductions were greatest in the forefoot area. The results of this study demonstrate that in healthy individuals without clinical foot deformity, the Bledsoe Diabetic Conformer Boot performs as well as, and in some parameters even better, than a total contact cast to reduce the force, pressure, and pressure-time integral under the plantar surface of the foot. This was most strongly demonstrated under the forefoot, which is the area most often affected by neuropathic ulceration in the diabetic. The Bledsoe Diabetic Conformer boot had two main features which may explain why they function better than a TCC with respect to pressure reduction. First of all we believe that the auto-mold inner sole conforms better to the subject's foot which helps distribute the force over a greater area of the plantar surface and up the sides of the foot. Secondly, the walking boots have a three rocker sole which makes walking easier with less energy.
The Bledsoe Diabetic Conformer Walking Boot™ may be clinically applicable to the treatment of neuropathic ulceration as a substitute for the total contact cast. Potential advantages may include ease of application, and costs-savings effected as a result of a less labor-intensive method of off-loading the neuropathic foot. Additional studies are currently underway to investigate this technique in patients with diabetes and clinical foot deformity, while also examining clinical data and the effect of this technique on ulcer healing.