
Abstract
A case is described of a 20-year-old college student in whom open reduction and internal fixation of a Weber B fibula fracture was complicated by arterial thrombosis and gangrene of the foot. The patient subsequently required a below-knee amputation. A hypercoagulability workup revealed the presence of an anticardiolipin antibody. Although this is an extremely unusual complication, young female patients with a positive personal or family history of early thrombotic events, such as DVT, multiple pregnancy loss, or early myocardial infarction, should be viewed as being at increased risk. Additional risk factors such as oral contraceptive use, should be sought during the initial history.
INTRODUCTION
Anticardiolipin antibodies belong to the phospholipid antibody (lupus anticoagulant) family of antibodies that prolong phospholipid-dependant coagulation reactions. The antiphospholipid antibody syndrome is the occurrence of anticardiolipin antibodies with arterial or venous thrombosis, fetal loss or thrombocytopenia. Estimates for the prevalence of this syndrome vary widely. In healthy volunteers the prevalence has been estimated between 5 and 9%, while among individuals with systemic lupus erythematosus (SLE), 25 to 45% may express these antibodies. 1 This case of arterial thrombosis following a simple fibula fracture is unique and suggests the need for additional investigation to determine the role hypercoagulability plays in contributing to thrombosis in patients who undergo orthopedic surgical procedures.
Case Report
The patient is a 20-year-old female college student who sustained a closed right fibula fracture as a result of a twisting injury that occurred while playing rugby. She had an unremarkable personal medical history, did not smoke cigarettes, and consumed alcohol only on occasion. She was taking oral contraceptives for approximately six months prior to the accident but discontinued them following her injury. Her only previous surgery was an uncomplicated wisdom teeth extraction. The patient had no history of vascular disease, coagulopathy or autoimmune disease. Her family history was significant for a myocardial infarction in her maternal grandfather at the age of 47.
The patient presented to her local hospital the afternoon of the injury. Radiographs demonstrated a Weber B fibula fracture. The following day she underwent open reduction and internal fixation through a single lateral incision (Figs. 1, 2). She was splinted in the operating room and sent home on the first postoperative day. Over the next several days, she experienced pain unresponsive to analgesics, and on the sixth postoperative day was evaluated for new, progressive discoloration of a toe. The splint was removed and was not noted to be too tight. Examination out of the splint revealed adequate capillary refill and soft compartments; however, pulses were not documented at that time. She was re-splinted and discharged, but returned the next day with increasing discoloration and pain in her toes. Angiography demonstrated complete arterial thrombosis of the anterior and posterior tibial arteries. She was then transferred to our facility.

Radiograph of affected extremity prior to surgical fixation

Radiograph of affected extremity following surgical fixation
Upon arrival, she was found to have a temperature of 38.9°C, pulse of 104/minute and blood pressure of 110/60 mm Hg. Her foot was edematous, mottled, and cool to the touch (Figs. 3, 4). Slight serous drainage was noted from the operative wound. The discoloration extended about 5 cm proximal to the malleoli with sparing of the heel. The patient was able to move her toes with difficulty and sensation to light touch was diminished in all nerve distributions distally. The popliteal pulse was palpable, however the posterior tibial pulse was monophasic on Doppler exam. A repeat angiogram demonstrated tapering occlusion of the anterior and posterior tibial arteries at the level of the ankle with no reconstitution distally. Radiographs showed that the ankle was reduced.

Gross appearance of affected extremity at presentation.
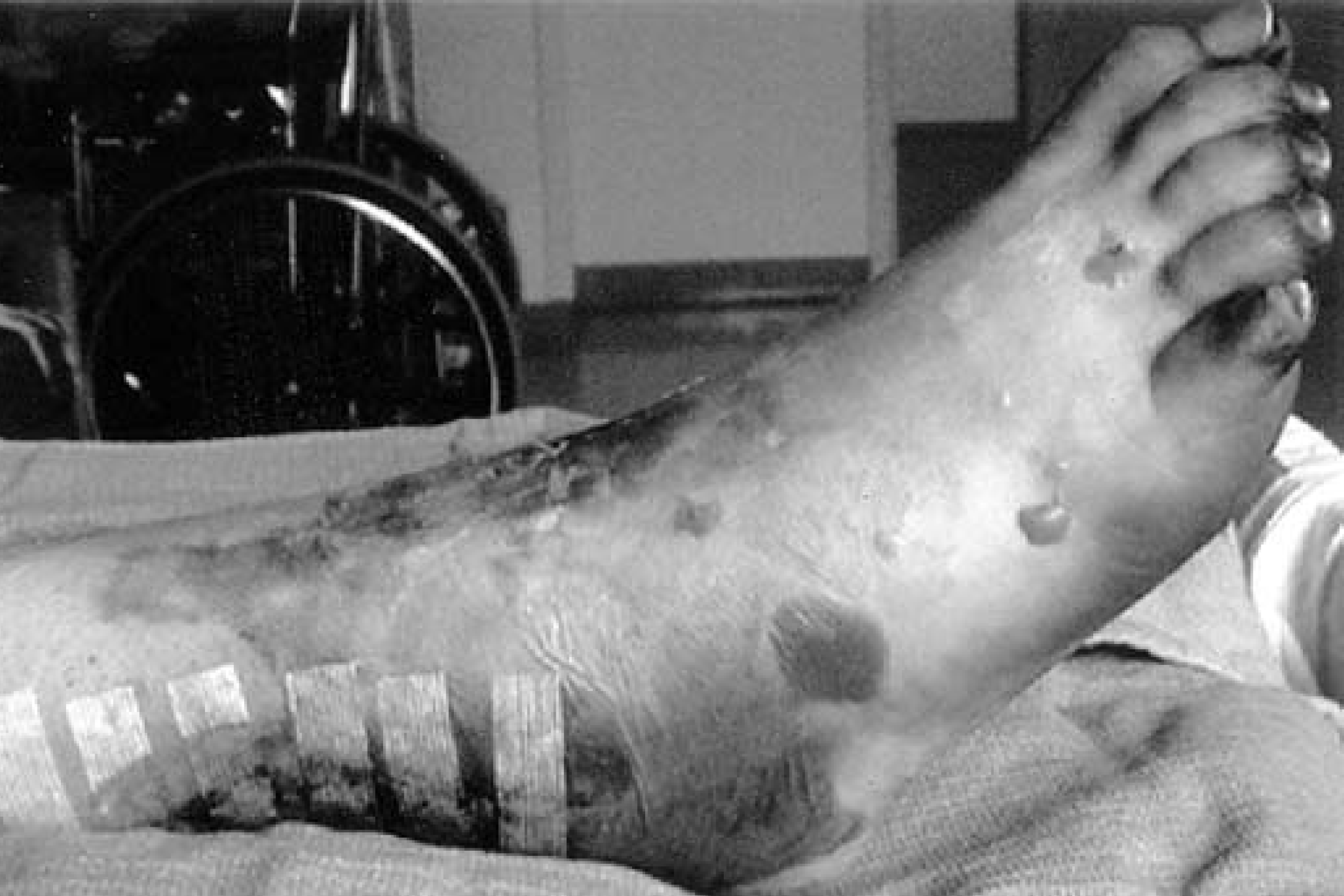
Gross appearance of affected extremity at presentation.
The patient's right foot and ankle were necrotic, gangrenous and judged to be nonviable. The presentation was not consistent with a missed foot compartment syndrome. In addition, there was no evidence of infection proximal to the surgical wound and there was no evidence of thromboses in her other extremities. She was started on heparin and a hypercoagulable workup was performed which revealed elevated levels of anticardiolipin IgG and IgM antibodies. Other indicators of hypercoaguability, including Protein S, Protein C, Factor V Leiden, Prothrombin 20210, and Homocysteine, as well as her peripheral blood count were within normal limits. A below-knee amputation was performed without complication. Pathologic examination of the specimen demonstrated organizing thrombus of unclear duration within the anterior and posterior tibial arteries. Despite postoperative neuropathic pain, she was ambulating successfully with a prosthesis five weeks later. The patient was anticoagulated with warfarin postoperatively for three months and has had no additional thromboembolic episodes in the 10 months since her injury.
DISCUSSION
The antiphospholipid syndrome is a hypercoagulable state characterized by the predisposition of affected individuals to test falsely positive in serologic assays to detect syphilis infection. 2 Immunoglobulin from these individuals, the cause of the cross-reactivity, nonspecifically inhibits phospholipid-dependant coagulation assays and is directed against a lipid-binding inhibitor of coagulation b2-glycoprotein I (apolipoprotein H). 3 Cardiolipin, a lipid present in mitochondrial membranes, is the antigen typically used in these tests; hence, anticardiolipin antibody syndrome is often used to describe this condition more specifically. The term lupus anticoagulant was used initially to denote antiphospholipid antibodies that prolong clotting time in patients previously diagnosed with systemic lupus erythematosus. 4 However, individuals with the lupus anticoagulant rarely have lupus, and the majority of those with SLE do not have the lupus anticoagulant. 5 Although considered as a unique entity, lupus anticoagulant is now known in some cases to act on cardiolipin. 6
Despite their effect on coagulation times in vitro, antiphospholipid antibodies may be paradoxically associated with arterial and venous thrombosis. Characteristic thrombotic manifestations include cerebrovascular accidents, myocardial infarction, deep vein thrombosis with pulmonary embolus, and recurrent spontaneous abortion. 7 Peripheral vascular disease, another described outcome of this syndrome, occurs less frequently and responds poorly to attempts at revascularization, 8 although this remains controversial. 9
In addition to anticardiolipin antibodies, other risk factors that may have contributed to thrombosis in this patient included oral contraceptive use, circulatory stasis secondary to immobilization of the extremity, the possibility of direct arterial injury, and heightened inflammation secondary to the surgery. Individually, these risk factors, which may be present in any orthopedic trauma patient, are not usually of a significant magnitude to result in perioperative thrombosis. However, together with a lupus anticoagulant or anti-cardiolipin antibody, the risk of thrombotic events may increase. 10
Traumatic or iatrogenic arterial injury, intimal disruption and embolic phenomena are unlikely in this case due to the tapering occlusion observed on angiogram of both the anterior and posterior tibial arteries. An inflammatory response to surgery or stasis secondary to postoperative immobilization are also unlikely to have been the primary cause of the thrombosis as, to our knowledge, complete arterial occlusion following surgery for isolated fibula fracture has not been documented despite the thousands of these procedures performed annually. Other risk factors associated with thrombosis occurring despite anticoagulation are not known, and require further study.
Although we hypothesize that the cause of the thromboses in this patient was multifactorial, the most likely underlying cause for the catastrophic vascular insufficiency and subsequent amputation was the patient's hypercoagulable state: anticardiolipin antibody syndrome. Notable is the total absence of prior thrombotic manifestations of the disease in this patient. The incidence of deep vein thrombosis (DVT) among patients with symptomatic antiphospholipid antibody syndrome, which may be as high as 50%, 11 typically precedes the first episode of arterial thrombosis. 8 Thus, the absence of prior thrombosis in this case suggests that oral contraceptive use 12,13 and/or trauma 14 may have precipitated anticardiolipin antibody formation and thrombosis. A hormonal etiology for anticardiolipin antibody syndrome is supported by studies in a murine model; however, it is not known whether antibodies detected in these circumstances are truly prothrombotic in vivo. 15,16 The apparent association with trauma may be due to immunogenicity of phospholipids on exposed endothelial cells. 17
There is no universally agreed upon treatment for anticardiolipin antibody syndrome. Anticoagulation is not currently recommended in asymptomatic patients with an incidental finding of antiphospholipid antibodies unless they are symptomatic or have multiple risk factors, per guidelines of the Haemostasis and Thrombosis Task Force of the British Society for Haematology. 18 Treatment recommendations for those with arterial or venous thromboembolus include heparin followed by warfarin to an international normalized ratio [INR] of 3. 19,20 Responsiveness to anticoagulation varies, however, and a single INR value may not be appropriate, or even accurate, in all patients. 21 The optimal duration of anticoagulation is also not known: some advocate six months 19 while others suggest lifelong anticoagulation, 22 depending on the presence or absence of modifiable risk factors. Our patient was anticoagulated with warfarin for three months and was no longer taking oral contraceptives. It is intuitive that early recognition of a thrombotic event may allow for more effective intervention, but, at this time, no study has investigated the efficacy of medical or surgical treatments for this situation.
In summary, an otherwise-healthy 20-year-old female taking oral contraceptives presented with arterial insufficiency of the lower leg and foot following surgical repair of a distal fibula fracture. A hypercoagulable workup revealed anticardiolipin antibody. As this case demonstrates, hypercoagulable states may be associated with significant morbidity in the patient with a common fracture. It would seem prudent to screen young individuals with threatened or actual thrombotic events in the perioperative period for hypercoagulable states. More studies are needed to better define the risk factors for acute, post-operative arterial thrombosis secondary to anti-cardiolipin antibody syndrome and to determine if such cases can be prevented or more effectively treated.
Footnotes
ACKNOWLEDGEMENT
The authors gratefully acknowledge the assistance of Dr. Arthur Manoli in the preparation and review of this manuscript.