
Abstract
The complex valgus deformity of the right ankle of a 24-year-old Maffucci syndrome man was corrected by three-dimensional osteotomy followed by limb lengthening. Before surgical correction of the deformity, we used computed tomography data to make a life-size three-dimensional plastic model of the deformed ankle for an accurate understanding of the anatomical deformity. We then used this model to perform a simulated osteotomy. The real osteotomy was performed immediately afterwards and valgus and recurvatum deformities were corrected accurately. We recommend simulated surgery using a three-dimensional plastic model which will improve the pre-operative planning technique and the accuracy of the end results.
INTRODUCTION
Maffucci syndrome is a condition featuring multiple hemangiomas and enchondromas. Due to multiple enchondromas involving the growth plate of long bones in childhood, shortening or deformity of affected bone is often apparent. 3 These limb shortenings or angled deformities can be so complex that it is difficult to correct them. Before any surgical treatments for these conditions, an accurate understanding of the anatomical deformities is essential. Recent remarkable progress in imaging equipment makes it easy to obtain information about bone. We present a case of 24-year-old man suffering from Maffucci syndrome whose limb deformity was assessed by means of computer-assisted design (CAD), and was corrected successfully by osteotomy.
CASE REPORT
A 24-year-old man was admitted to our clinic for the treatment of his ankle deformity. The patient was first diagnosed as Maffucci syndrome at the age of four, and multiple hemangiomas had been removed many times. His chief complaint was valgus deformity of the right ankle and pain at the medial aspect of the ankle especially on weight bearing. Examinations showed him to have many subcutaneous hemangiomas in the right extremity and his ankle showed valgus deformity so that he was standing on the medial aspect of the foot (Fig. 1). The range of motion of the ankle was restricted compared to contralateral side (20° dorsi flexion and 40° planter flexion, 35°, 50° respectively in contralateral side). Tomography revealed 45° valgus (apex medial) deformity and 30° apex anterior deformity at the distal tibia (Fig. 2). Tracings were obtained from the frontal and lateral radiographs (Fig. 3). Three-dimensional (3-D) wedge osteotomy was then planned for correction of these deformities; proximal cut was made in the plane perpendicular to the tibial axis, and distal cut was performed in the plane made by two lines, a line 45° oblique in the frontal projection and a line 30° apex posterior in the lateral projection. We made a life-size 3-D plastic model of the deformed ankle in order to identify the actual bone shape (Fig. 4). The model was made by transmitting DICOM (Digital Imaging and Communications in Medicine) data of 1 mm slice computed axial tomography to the main computer via the local area network (LAN), and the data was converted to 3-D with a conversion software, Mimics (Materialise, Belgium). The model was then made with starch powder by a 3-D printer (Z-402, Z Cooperation, MA) that injects fine glue onto the layer of starch powder. We actually performed simulated osteotomy on this model, which was followed by accurate correction of the valgus and recurvatum deformities. The patient's osteotomy was performed following the model surgery. The separated bones were fixed with an Orthofix external fixator, and the operated tibia was 2.5 cm short. After a two-week rest, limb lengthening was started at the rate of 1 mm/day. Callotasis was successful and uneventful (healing index: 35 day/cm). After leg lengthening, the external fixator was removed and the patient could stand on the entire sole (Fig. 5). The ROM of the ankle joint had improved equally to the contralateral side.

Valgus deformity of the right ankle and many subcutaneous hemangiomas are apparent.

Tomography revealed 45° valgus (apex medial) deformity and 30° apex anterior deformity at the distal tibia.
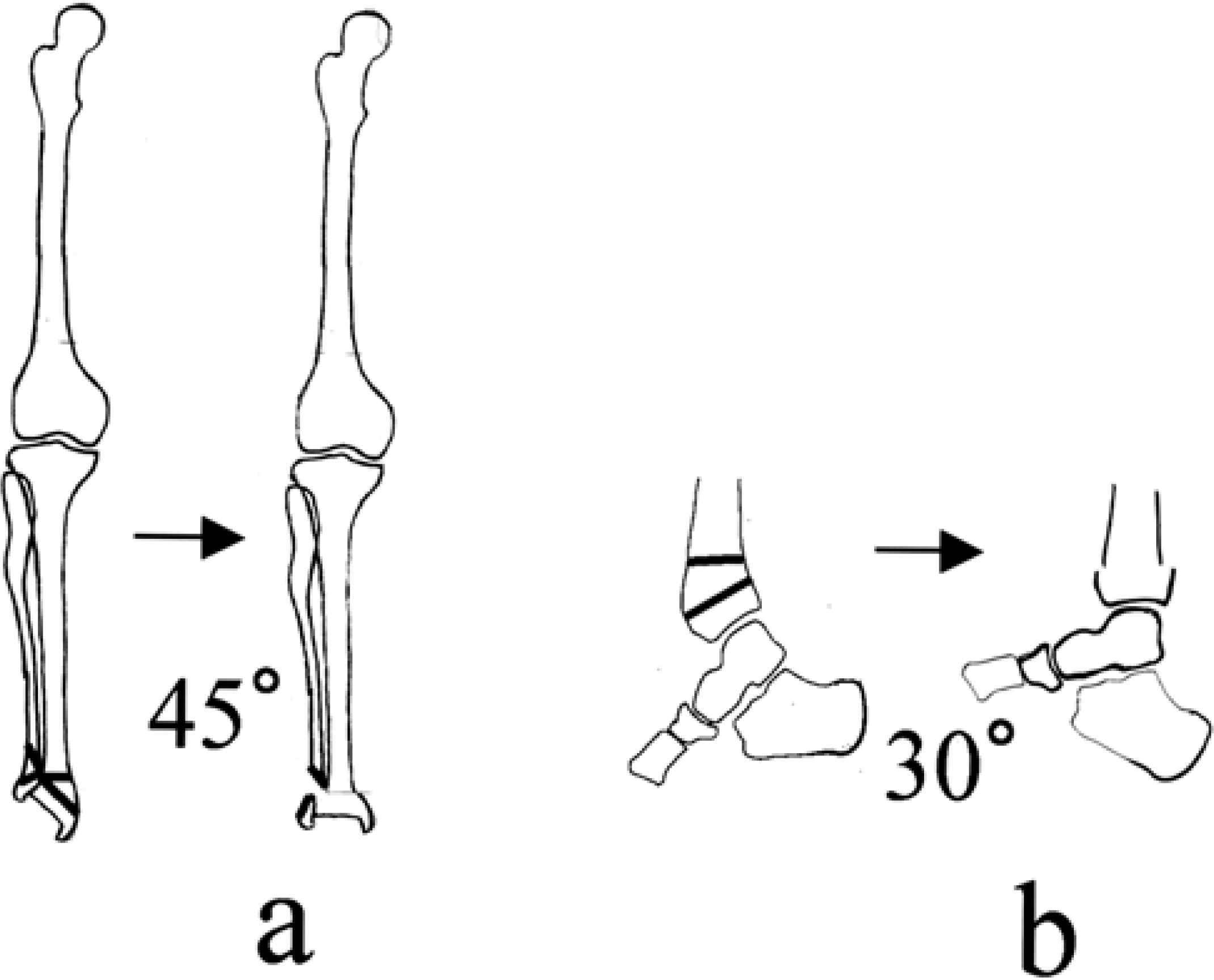
Tracings were obtained from the frontal and lateral radiographs. 45° valgus deformity and 30° apex anterior deformity were planned to correct by osteotomy.
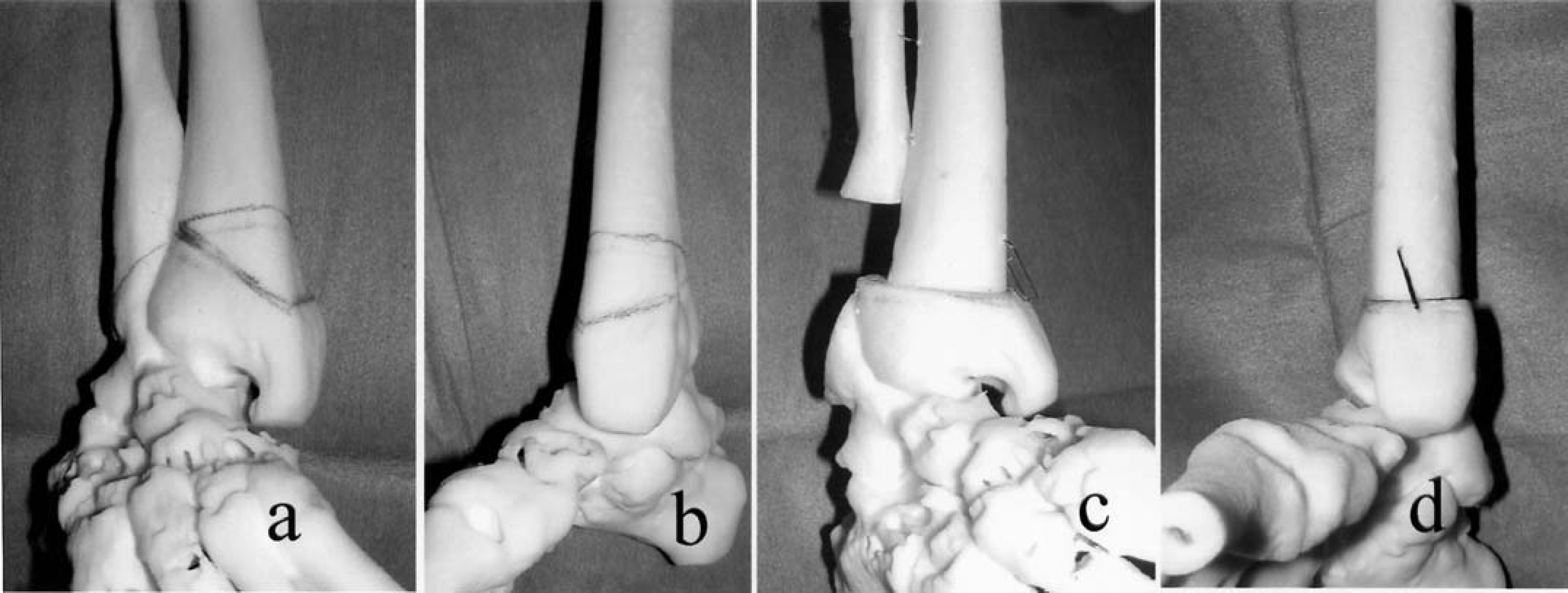
A life-size 3-D plastic model of the deformed ankle (a. frontal view, b. lateral view). The line is indicating the site for osteotomy. After simulated osteotomy with a 3-D plastic model, perfect correction of the valgus and recurvatum deformities were obtained (c, frontal view. d, lateral view)

After deformity correction and leg lengthening, bone formation at leg lengthening site was excellent
DISCUSSION
Ankle joint deformity causes many problems such as restricted range of motion, instability when standing on one foot and osteoarthritic changes. Our case also had difficulty standing on one foot as well as pain at the medial aspect of the ankle and foot. The pain was caused by high tension in the posterior tibial tendon and pressure on the many hemangiomas especially in the medial sole skin. Deformity correction of the ankle has brought many benefits to our patient, since he can now run quite fast without pain.
The Maffucci syndrome is accompanied by multiple enchondromas. This may seem to be a disadvantage for limb lengthening because of the presence of diseased bone, but a study of leg lengthening for Maffucci patients has reported no abnormalities even at the affected site. 7,11 For our patient, leg lengthening was performed through the actual osteotomy itself. This is contrary to the standard method of callotasis, where a corticotomy is first performed in a closed fashion to minimize disruption of the blood supply which is then followed by lengthening. Although our method may entail a high risk of nonunion due to periosteal stripping that would be necessary at the wedge resection site, a previous study which focused on immediate correction of limb deformity followed by limb lengthening with unilateral fixator reported success without any problem of nonunion. 5 It is important to preserve the periosteum to a maximal extent at osteotomy site. Furthermore, in order to avoid subsequent deformity caused by minor bending of the pin of the unilateral fixator inserted during limb lengthening, over-correction of the deformity by osteotomy must be included.
The limb deformities presented here are often seen and comprise fracture malunion, osteomyelitis sequelae and congenital anomaly. Surgical treatment is the treatment of choice for correction of these deformities. 2,6 Wedge or dome osteotomy is performed for correction of simple axial deformity. 9,10 For a complex deformity that is often accompanied by limb shortening, oblique or 3-D corrective osteotomy is performed for immediate correction with a unilateral fixator for limb lengthening, 5 or an osteotomy with a Ilizarov fixator attachment followed by both limb lengthening and gradual correction of the deformity with a fixator. 2 In the latter case, a complex deformity is difficult to visualize solely with the aid of two-dimensional films. For an accurate understanding of the deformed bone, the 3-D plastic model introduced here is very helpful. The model is life-size, so the distance from landmarks to osteotomy line can be determined to make it easy to cut the bone at surgery; furthermore, accurate placing for pinning or plating is possible resulting in a successful operation.
Other applications of 3-D models for orthopedic field have been introduced. 1,4,8 There are two types of 3-D plastic models made of different material, starch and resin. The model made of starch is cheaper and faster to make. For example, it takes only about seven hours for an ankle model, and can easily be cut with a knife, making it preferable for simulated surgery. In fact, we have used this model for severe deformity of the knee joint after osteomyelitis, for ankle osteoarthrosis following severe deformity leading to total ankle joint replacement as well as other deformities, and have obtained good results in all cases. We therefore conclude that simulated surgery using a 3-D plastic model improves the pre-operative planning technique and will improve the accuracy of the end result.