
Abstract
For a 29-year-old man with a three-week-old Hawkins Type IV talar neck fracture, intra-operative reduction and fixation were not possible due to soft tissue contractures and severe comminution. A primary talonavicular and subtalar arthrodesis with the use of iliac crest bone graft was performed. Postoperative follow-up at 16 months demonstrated solid fusions, no avascular necrosis of the talus and a functional range of motion at the ankle. He was not capable of returning to his job of roof maintenance.
Keywords
INTRODUCTION
Talar neck fractures (TNF) make up 50% of all major injuries to the talus and are associated with significant morbidity. In 1970, Hawkins 3 published a TNF classification system which is widely used today - Type I: undisplaced, Type II: displaced with subluxation or dislocation of the subtalar joint with the talar body reduced within the ankle mortise, and Type III: displaced with dislocation of the talar body from the ankle mortise. In 1978 Canale 1 et al. recognized a fourth fracture pattern - a Type II or Type III associated with dislocation of the talonavicular joint: a rare injury with little information on clinical management and outcome to date. This often high-energy trauma with significant deformity is seldom subject to delayed diagnosis.
CASE REPORT
A 29-year-old man sustained a fracture of the talar neck from a fall of approximately 12-foot height. He was first assessed in an emergency room. Because he was able to weightbear (albeit with some difficulty), radiographs were not obtained and he was simply advised that he had an ankle sprain. His continued complaints of pain and stiffness prompted radiographic evaluation approximately 19 days following the injury - a three-week delay in diagnosis from the injury date to his presentation at our institution. His clinical examination revealed residual swelling of the foot and ankle with the skin intact and no open wounds. There was no neurovascular deficit. Radiographs revealed a Type IV talar neck fracture (Figs. 1a, 1b, 1c).

During the surgery, the fracture-dislocation was accessed through a combined dorsal-medial and dorsal-lateral approach. A large amount of fibrous tissue and comminuted bone fragments were removed. When the non-comminuted portion of the talar neck was identified, it consisted of the medial half of the talar neck and head, completely dislocated from the talonavicular joint and devoid of any soft tissue attachment. This fragment of the talar head and neck was removed. The talar body was extended at the neck and held in a neutral dorsiflexed position with smooth K-wires transversing the tibia and the talar body. The posterior facet of the subtalar joint was then reduced and held with smooth K-wires. A femoral external distraction device was applied to the tibia and midfoot on the medial side in an effort to bring the midfoot out to length and to aid in fracture reduction. Due to the severe soft tissue contractures and the gross comminution, reduction and fixation were not possible. It was, therefore, decided to proceed with a primary fusion of the subtalar and talonavicular joints. In the absence of the talar neck and head, it was possible to prepare the subtalar joint and articular surface of the navicular through the dorsal-medial incision. The intact portion of the talar neck and head was prepared and used as a strut graft between the talar body and the navicular. The remaining defect was packed with autologous iliac crest bone graft. The arthrodesis was stabilized using two 4.5 mm cannulated screws from the navicular into the talar body and one 7.0 mm cannulated screw from the calcaneus into the talus.
The patient was treated in a non-weightbearing cast for six weeks and in a weightbearing cast for six weeks. He underwent an uneventful postoperative recovery. A Hawkins sign 3 was observed at seven weeks. At the six-month review, fusion was complete with no evidence of avascular necrosis (Fig. 2).
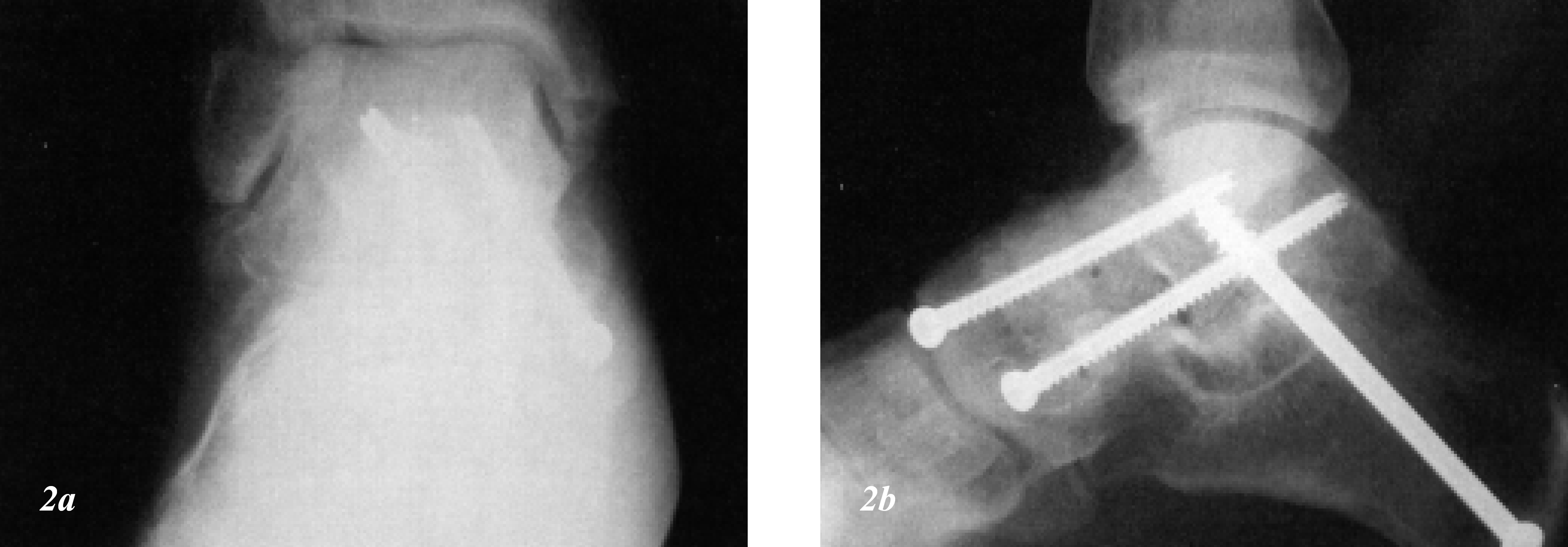
2a (AP view) and b (lateral view) of the hindfoot demonstrate a subtalar and talonavicular joint fusion with no evidence of avascular necrosis.
The patient was last assessed at 16 months postoperatively. Radiographs demonstrated consolidation at the subtalar and talonavicular joints with no signs of avascular necrosis of the talar body (Fig. 3a-b). He had no loss of sensation to the foot and no clawing of the toes that would suggest a previous compartment syndrome (Fig. 4). He had approximately 50° arc of motion at the ankle and no motion through the subtalar complex. Unable to return to work as a roofer, he was retraining for a sedentary occupation at the time.
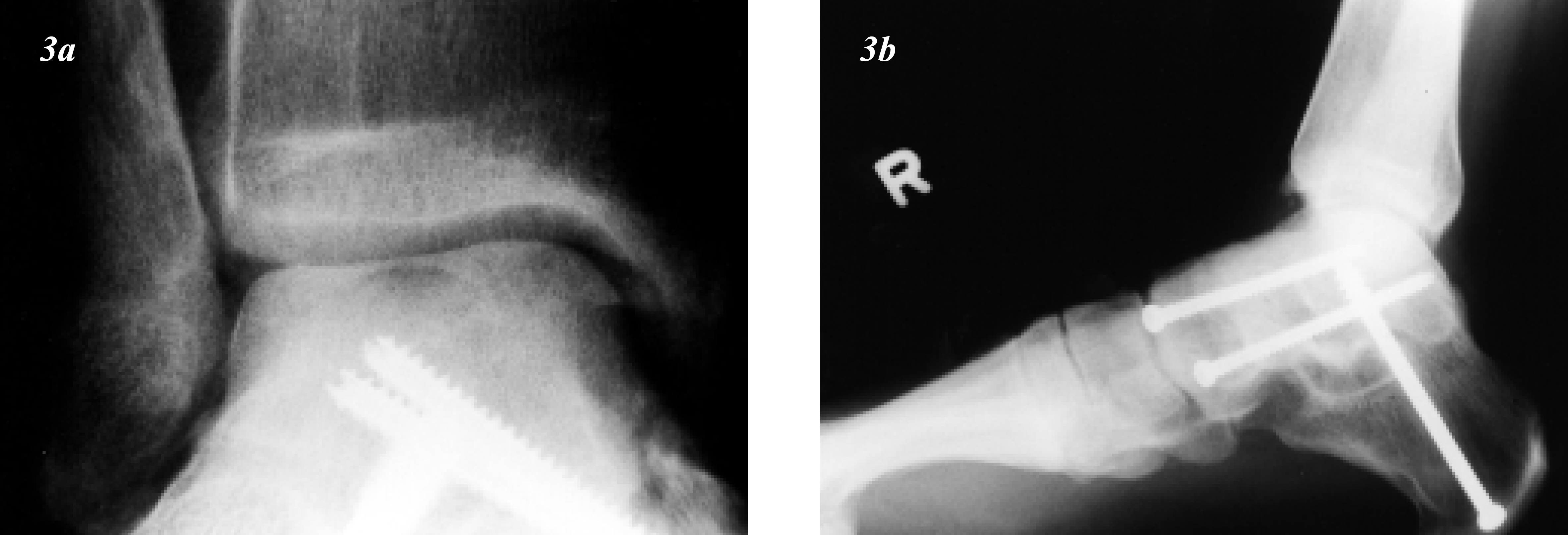
3a (AP view) and b (lateral view) of the ankle and hindfoot at 16 months following the arthrodesis. No radiographic evidence of avascular necrosis of the talar body. The patient had a functional and painless arc of motion at the ankle joint.

4a (medial view of foot) and b (AP view of both feet) at 16 months following the arthrodesis. Clinically, the patient had a plantigrade foot with normal sensation to the dorsal aspect of the foot. No deformity of the toes had occurred. There was a full range of motion at the metatarsophalangeal joints of the toes indicating no previous evidence of a compartment syndrome.
DISCUSSION
Type IV talar neck fractures are rare and there are very few reports in literature today. Optimal management centers around reduction and stabilization of the talonavicular joint combined with adequate management of the talar neck fracture. An immediate intervention is recommended with the use of a careful surgical dissection and rigid internal fixation. 2
In the case of our Type IV fracture, two specific problems influenced the ultimate surgical management. First, the delay in diagnosis had caused significant soft tissue contractures which made reduction difficult. Second, the severe comminution of the head and neck fragment precluded adequate restoration of the articular surface. As a result, a primary arthrodesis of the subtalar and talonavicular joints was performed - contrary to previous reports documenting salvage via a tibiocalcaneal fusion. 5 This procedure restored the length of the foot's medial column while preserving motion at the ankle.
The Type IV talar neck fractures tend to result in a less-than-favorable outcome. The severe nature of the injury would account for the morbidity. Canale and Kelly 1 reported on the outcome of three patients: two fair and, one poor. In a recent study, Pajenda et al. 4 reported a good outcome in only 10% of 11 patients. Following an injury of this severity, avascular necrosis can occur in both the talar head and body. 2
Fractures of the talar neck are often challenging to treat and can progress to secondary complications even with appropriate management. This case study illustrates that a salvage procedure may be required if problems are encountered intraoperatively and that a primary fusion is a viable alternative in the management of Type IV talar neck fractures.
Footnotes
ACKNOWLEDGMENT
The authors thank the British Orthopaedic Association/Wishbone Trust and The John Charnley Trust for their generous support of Dr. Rhys Thomas's fellowship.