
Abstract
Background:
Although classically the fibula has been reported to be in external rotation after supination-external rotation (SER) or pronation-external rotation (PER) ankle fractures, a previous CT study demonstrated that what had traditionally been interpreted as external rotation of the distal fibular fracture fragment is actually internal rotation of the proximal fibular fragment. The purpose of this study was to evaluate a series of CT scans in patients who have suffered type IV SER or PER ankle fractures to assess the rotational deformity of the fibular fragment.
Materials and Methods:
CT scans of the injured and uninjured extremities were performed on 30 extremities which had sustained either SER (21) or PER (9) injuries. The rotational relationship between the tibia and fibula was determined by a measured rotational ratio. A qualitative assessment of the rotational relationship between the tibia and fibula above, at, and below the fracture site at the level of the mortise was also performed. The difference in the ratio (calculated by subtracting the rotation ratio of the normal side from the fracture side) demonstrated whether the fractured fibula is externally or internally rotated compared to the uninjured side.
Results:
The average rotational ratio difference above the fracture compared to below the fracture for the SER group demonstrated significant external rotation (p < .001). The PER fracture also demonstrated external rotation of the distal fragment compared to the proximal fragment (p = .002). Additionally, qualitative assessment of the relationship demonstrated no obvious change in the rotational relationship in any patient above the fracture site except one where mild internal rotation of the proximal fragment was noted. However, at the level of the mortise, all had a normal talofibular rotational relationship while 24 of 30 had widening of the medial clear space with external rotation clearly evident on 15 of these 24 scans.
Conclusion:
Our study demonstrated that the distal fibular fragment in both SER and PER fractures is externally rotated relative to both the contralateral normal side and compared to the proximal fibular fragment.
Keywords
INTRODUCTION
Ankle fractures are among the most common injuries of the lower extremity. Biomechanical studies have demonstrated significant alterations in stability and joint reactive forces associated with talar shifts and fibular displacement. 6,9 –11 Consequently, persistent fibular displacement following an ankle fracture has been an indication for surgical intervention. 1,3,7,8 However, there is no consensus as to the amount of fibular displacement that is accepted for surgical indication based on plain radiographs. Recent work utilizing computer tomography (CT) showed plain radiographs overestimate fibular displacement. 2 These authors also concluded that what had traditionally been interpreted as external rotation of the distal fibular fracture fragment is actually internal rotation of the proximal fibular fragment. However, the study evaluated mainly supination-external rotation (SER) type injuries and half of their patients were treated nonoperatively. Another study evaluated patients with an SER II injury without any deltoid ligament injury, and found that at the level of the ankle joint, there was no change in the medial joint space and little or no change in the lateral fibular talar interval. At the level of the syndesmosis, they noted the proximal fibular fragment to have assumed a position of mild medial displacement with apparent slight internal rotation in most cases. They only evaluated patients with nonoperative SER II ankle fractures. 2 The purpose of our study was to examine the fracture rotational relationship in displaced SER and PER ankle fractures.
MATERIALS AND METHODS
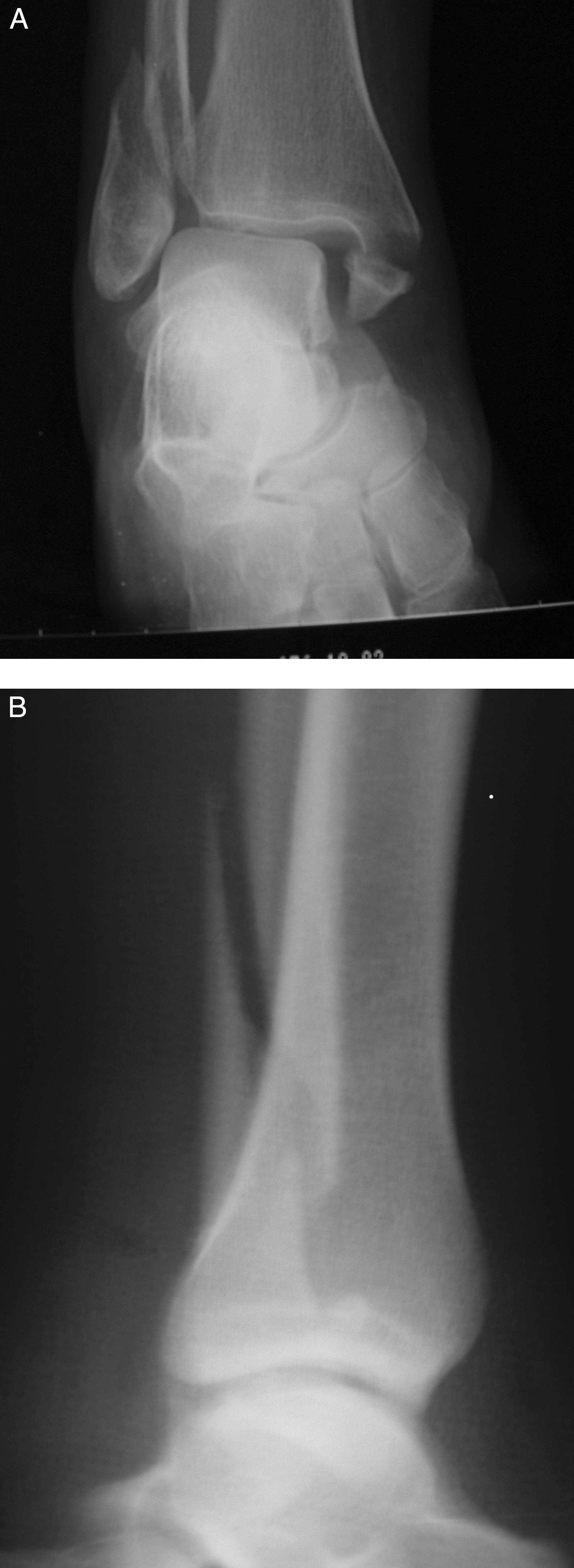
Patients with radiographic evidence of either displaced SER or pronation-external rotation (PER) type injuries in accordance to the Lauge-Hansen fracture classification were evaluated (Fig. 1). 3 All fractures underwent closed reduction with bier block anesthesia and were initially stabilized in a long leg cast or splint while awaiting surgery. Patients who had bilateral injuries or had prior injuries to the contralateral limb were excluded in order to allow for the contralateral limb to serve as a control.
A total of 30 patients were evaluated (13 female, 17 male). The average age was 39.3 years (range, 19–84). Thirteen of the ankles were fractured on the right side and 17 were on the left side. Nine patients had PER type injuries and 21 patients had SER injuries. A qualitative assessment of the rotational relationship of the tibia to the fibula was also made. At a site proximal to the fracture, visual evaluation of the tibia-fibular relationship was made and recorded as externally rotated, internally rotated, or no apparent rotation. At the joint level, the relationship between the talus, medial malleolus, and lateral malleolus was assessed. The evaluation included whether the medial or lateral clear space was widened and whether there was visible external or internal rotation of the malleolar fragment relative to the talus. Also, the preoperative mortise radiographs were assessed for medial clear space widening, lateral clear space widening, shortening of the fibula, and lateral talar shift relative to the tibia. Each of these measurements was made on a mortise radiograph with a ruler in 1-mm increments to the nearest millimeter. The measurements were repeated twice and were made by the senior author on both occasions. In no instance, measuring to the nearest millimeter, was there a difference in the measurement.
All patients had ankle CT scans performed in the same field of view on both the injured and the normal contralateral side as controls for comparison. Scans were performed with 3-mm cuts with a spiral CT scanner (Pickar PQ6000) starting proximal to the fracture site and extending to the subtalar joint. Scans 5 cm proximal to the fibular fracture, below the fibular fracture, at the level of the tibiotalar joint, and at the talofibular level were identified on the fractured side. The matching corresponding views on the normal, contralateral side were then identified starting at the tibiotalar joint, and then paired to the fractured side by the distance from the tibiotalar joint based on the CT slices. The matched CT cuts were then digitized using a digital camera (Kodak DC480, 3.3 megapixel) and downloaded into a JPEG file for measurement. Measurements of the CT scans were done using the Sigma Scan 4.0 software (Jandel Scientific, Chicago, IL).
Measurement of Tibia-Fibula Rotation
A tibia-fibula rotational ratio was used to assess the rotational relationship between the tibia and fibula. This ratio is calculated by dividing the distance (measured in pixels) between the center reference point of the tibia and the most anterior cortex of the fibula to the distance from the center reference point of tibia to the most posterior cortex of the fibula (Fig. 2). The center reference point on the tibia was determined by using multiple, bisecting lines and using the summation of the intersections as the center of the tibia (Fig. 3). The same measurements on the matched contralateral views were used for comparison. At the tibiotalar joint and talofibular level, similar methods of multiple, bisecting lines were used to identify the center reference point on the distal tibia and talus, respectively. Three separate measurements were made for each of the first five sets of CT scan pairs to ensure that the reference center and the rotational ratio calculated from the measurements were reproducible. The ratios from the same image were all within 0.005 on each measurement. The remainder of CT scan sets were only measured once.
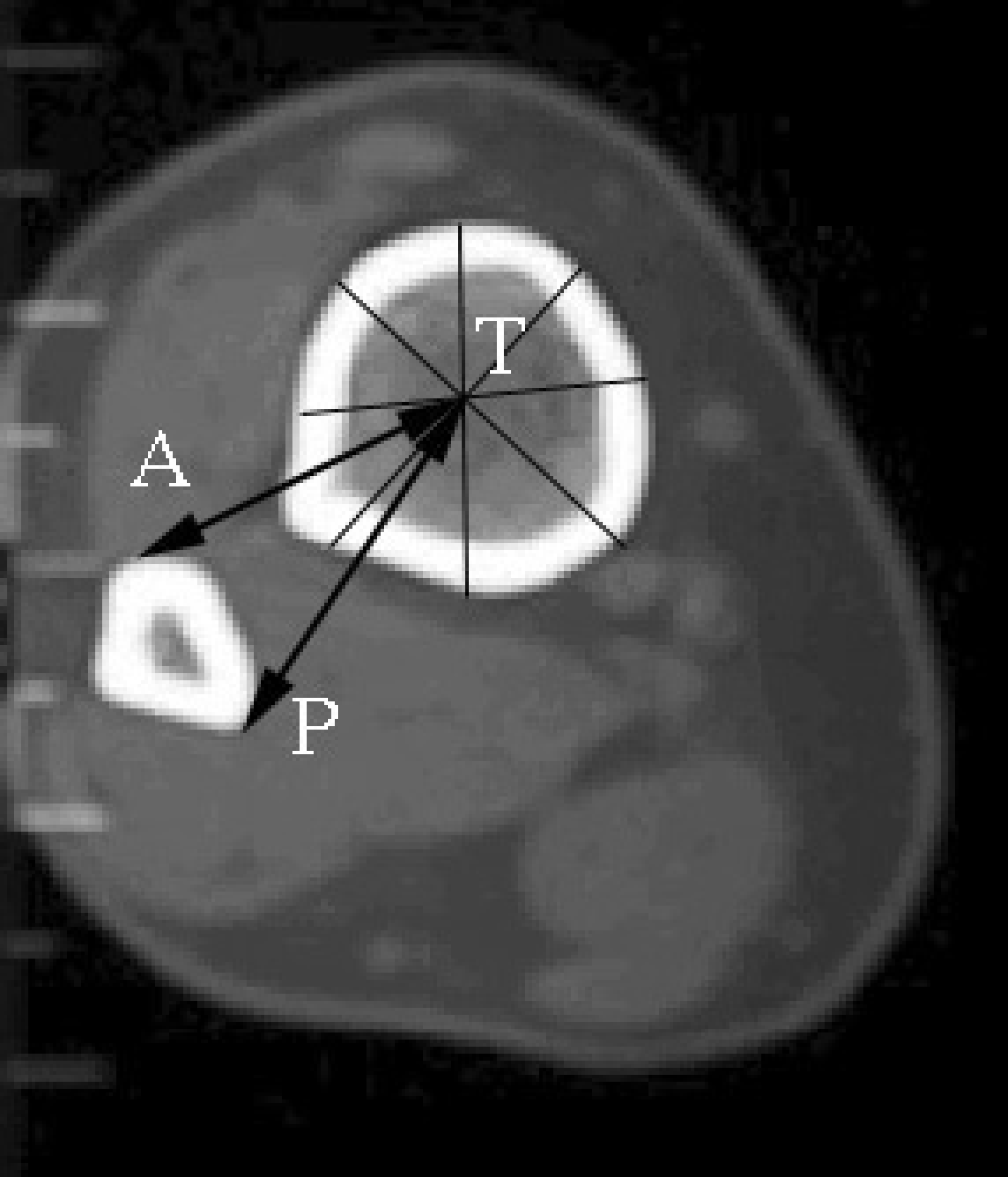
CT scan demonstrating the tibia/fibular rotational ratio of one cross-sectional CT scan.
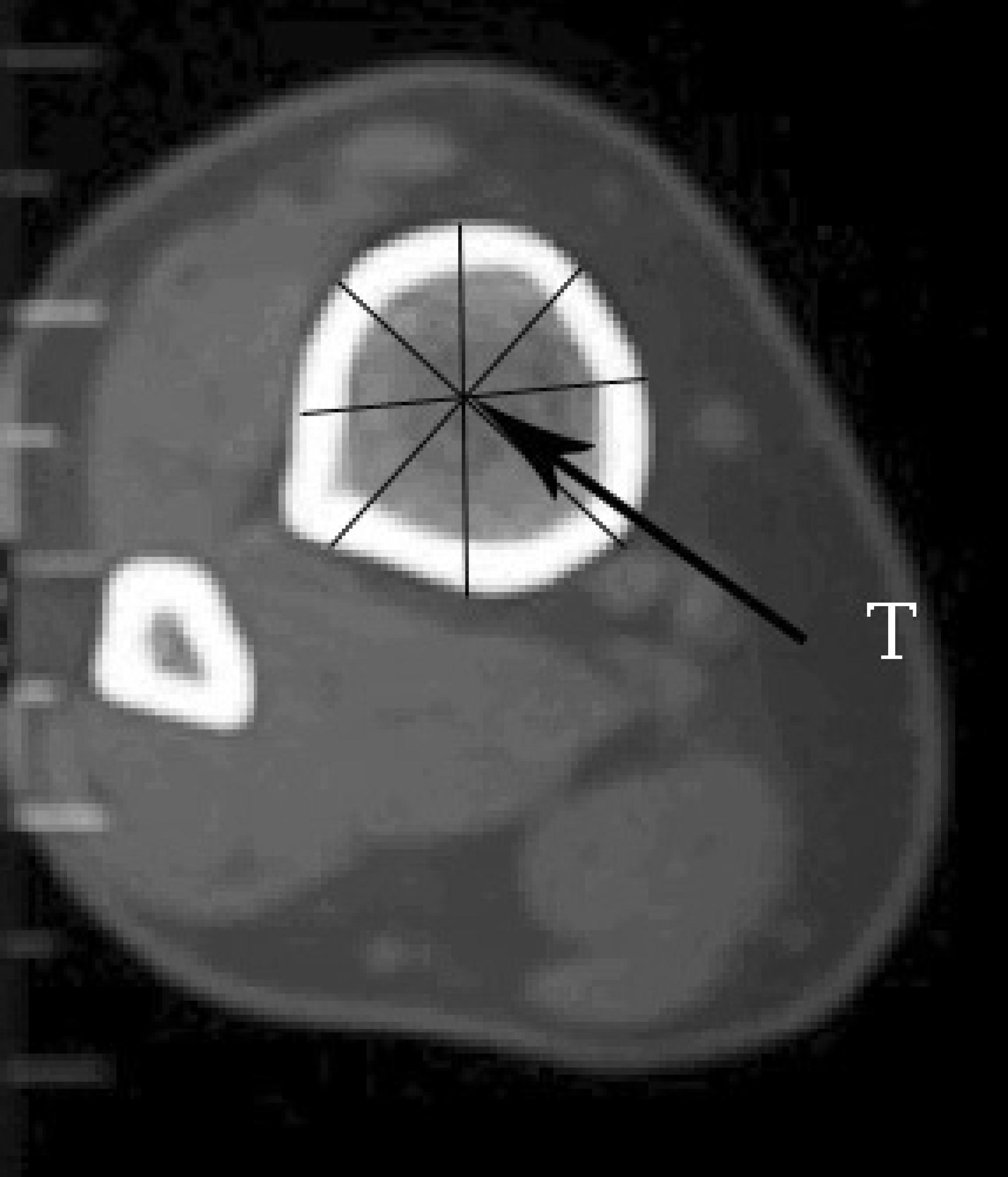
Center reference point calculation demonstrated on one CT scan.
A rotational change of the fibula in relationship to the tibia would be detected by a change in the ratio comparing the fractured side to the contralateral side. External rotation of the fibula brings the anterior cortex away from the tibia reference point and the posterior cortex relatively closer to the tibia reference point. Internal rotation of the fibula would result in the converse. The difference in the tibia-fibular rotation was assessed by subtracting the rotational ratio on the fracture to the normal side. A positive difference in rotational ratio (dRR) indicates that the fractured side is in relative external rotation compared to the normal side, and conversely a negative dRR indicates a relative internal rotation on the fractured side.
Statistical Analysis
The rotational differences were calculated and analyzed using the Student t test. A Mann-Whitney U-test was done to determine if a statistical difference existed between the rotational ratio between the normal side and fractured side. A p value of less than .05 was considered statistically significant.
RESULTS
Qualitative assessment of the CT scans revealed that 26 of 30 scans had a comparable scan above the fracture site which allowed for assessment of the rotational relationship. Four of the 30 scans did not have a CT cut at a level 5 cm proximal to the zone of injury, and thus these were excluded from the analysis. One of these 26 scans revealed visible internal rotation of the proximal fibular fragment compared to the tibia. Twenty-five of 26 scans with a comparable level above the fracture site revealed no change in the rotational relationship and no visible difference between the fibula and tibia. All 30 CT scans had comparable cuts through the level of the midportion of the talus which allowed for visualization of both the medial and lateral malleoli. The talofibular interval was noted to be normal in 20 of 30 scans. Ten of 30 scans had mild widening but no rotational change. The medial malleolar interval was found to be widened in 24 of 30 scans. Of these scans with widening of the medial interval, 15 demonstrated external rotation relationship of the talus versus the medial malleolus.
Plain radiographic evaluation of the patients after reduction and placement in a cast revealed the average lateral talar shift was 1.4 mm (0–5 mm) and the average medial widening was 0.5 mm (0–4 mm). The average lateral widening was 0.3 mm (0–2 mm). The average shortening of the fibula was 1.3 mm (0–5 mm).
The rotational ratio (RR) between the normal side to the fracture side was compared for both SER and PER injuries above and below the fracture site (Table 1). Statistical analysis showed no difference between the ratio for the fractured and normal side above the fracture in both the SER (p = .882) and PER (p = .636) groups. In contrast, significant external rotation of the distal fibular fragment was noted in both the SER (p = .028) and PER (p = .023) injuries.
Comparison of rotational ratio between normal and fracture sides above and below the fracture site
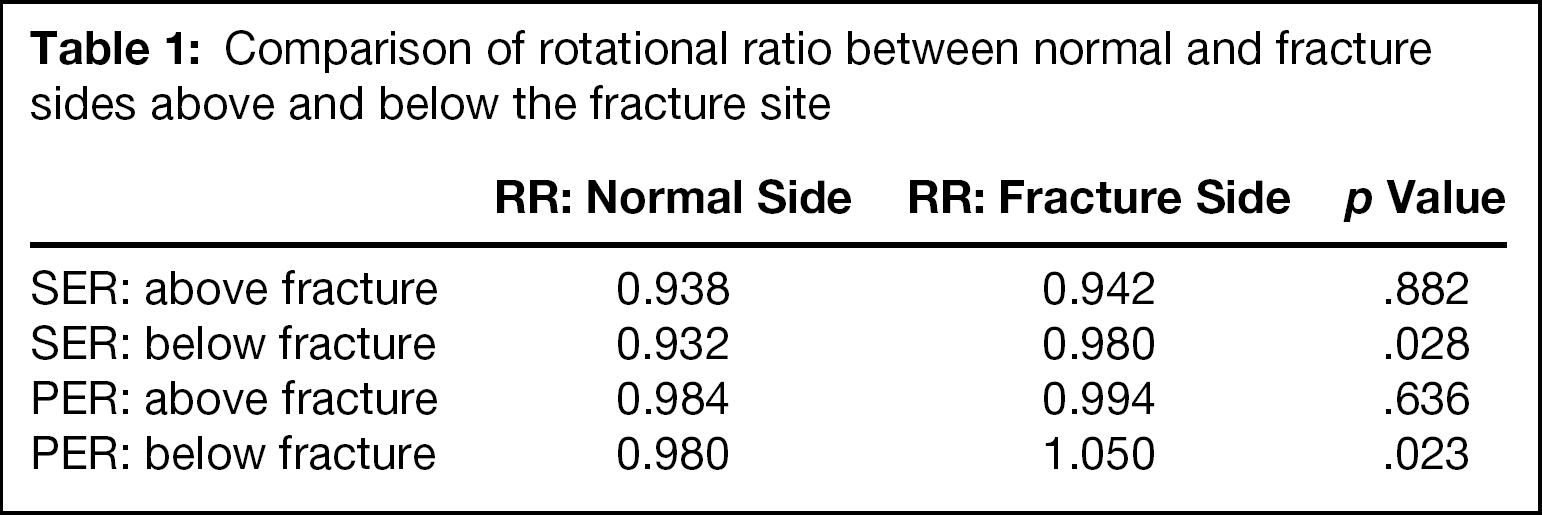
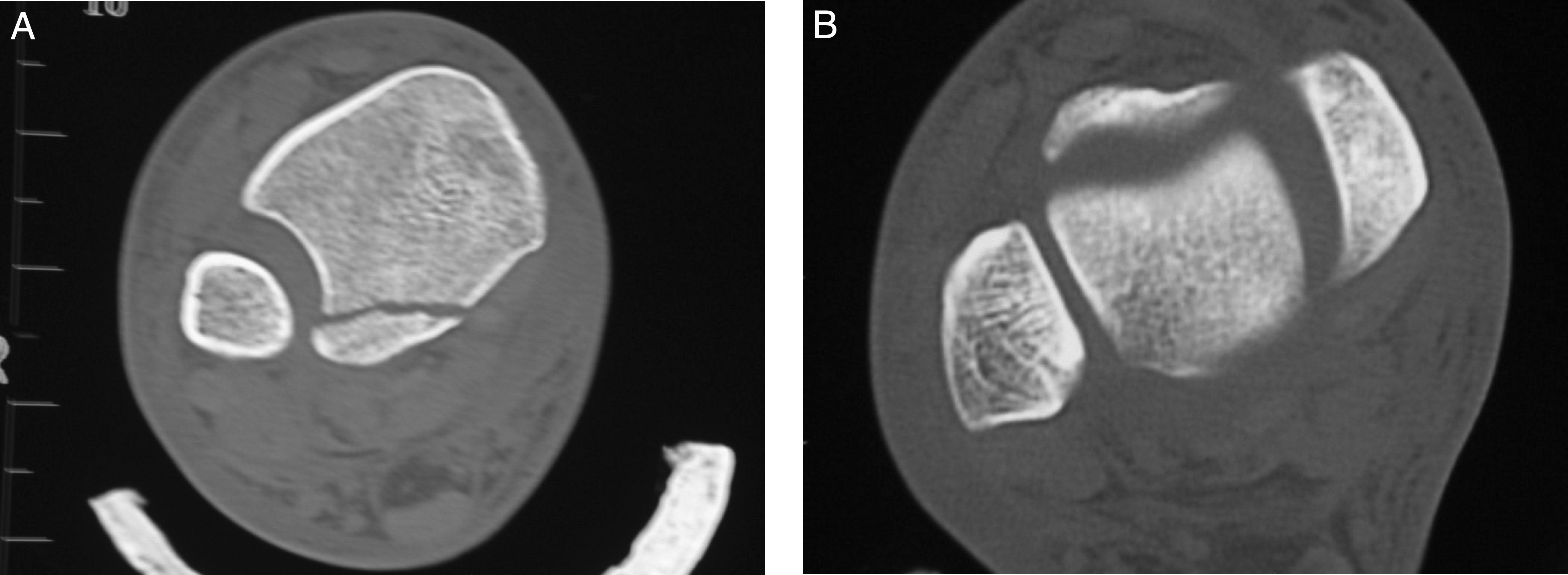
Table 2 shows the average dRR for each of the levels measured. Significant external rotation of the distal fibular fragments relative to the proximal fibula was noted in both the PER group (p < .001) and the SER group (p = .002).
Average rotational ratio difference between the fractured and normal side
DISCUSSION
Pathologic anatomy of the ankle fracture has been studied extensively in the past. To our knowledge, only one previous study utilized CT scanning to quantify the rotational relationship between the fibula and tibia in ankle fractures. Michelson et al. concluded that a relative internal rotation of the fibula proximal to the fracture site existed in external rotation mechanism ankle fractures, while the distal fracture fragment maintained its normal relationship to the talus. 5 In that study, rotation of the fibular fragment was assessed relative to the tibia by examination of the contour of the tibia-fibular space distally. In that study, they evaluated 26 ankle fractures, of which half were treated nonoperatively. In contrast, the present study only evaluated SER and PER fractures which underwent surgical treatment. The CT technique used in that study was previously reported by them in the radiologic literature. 4 Their technique does not use premeasured distances from the ankle joint or the fracture site as was used in this study. The distal fibula and tibia-fibular space were assessed for width, contour, and deviation from the contralateral side on the first image above the tibial plafond. No quantitative assessment of the rotational relationship was performed in their study. A figure in that study at the level of the talocrural joint noted that a patient had subtle talofibular widening but did not comment on significant widening and external rotation between the medial malleolus and talus. 4 Harper noted in his study 2 that there was no evident widening between the medial malleolus and talus in any of the patients. It should be noted that none of the patients had a deltoid ligament injury, and that this was a group of patients with SER II ankle fractures treated nonoperatively. He noted mild widening of the talofibular interval through the joint. Otherwise, the CT scans were only performed at the level of the syndesmosis in that group, and not at a more proximal level as was performed in this study. However, our two groups of patients are not comparable as all of the patients in Harper's study had stable fractures treated nonoperatively due to the lack of deltoid ligament injury. All of the patients in the present study had medial ligamentous or bone injuries with instability which underwent surgical reduction and fixation.
The current study produced a different result, showing relative external rotational deformity distal to the fracture when compared to the normal contralateral side in both SER (Fig. 4) and PER (Fig. 5) ankle injuries. The current study utilized a quantitative rotational ratio to assess the relative rotation of the fibula to the tibia. A high degree of reproducibility was noted in the five sets of scans where measurements were repeated three times, and in the measurements of displacement on the mortise radiographs. Our data showed that the rotational ratio above the fracture site for both SER and PER injuries both quantitatively and qualitatively were not significantly different between the fractured side and the contralateral side. However, the ratio below the fracture for both the SER and PER groups were significantly different between the fractured side and the contralateral side (p = .028 and p = .023, respectively). Thus, the difference was due to external rotation of the distal fragments rather than the proximal fragments. Additionally, a normal talofibular relationship at the level of the ankle was noted in most of these patients. This finding, however, does not indicate that the distal fibular fragment was not rotated, but that it followed the talus as has been described by Yablon and others. 11
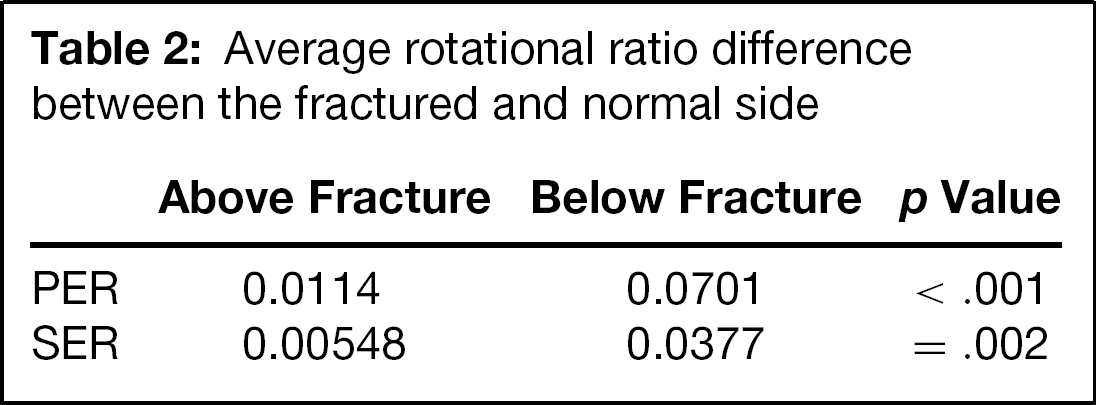
Computer tomography (CT) showing the rotational relationship between the tibia and fibula in a supination external rotation (SER) type IV injury.
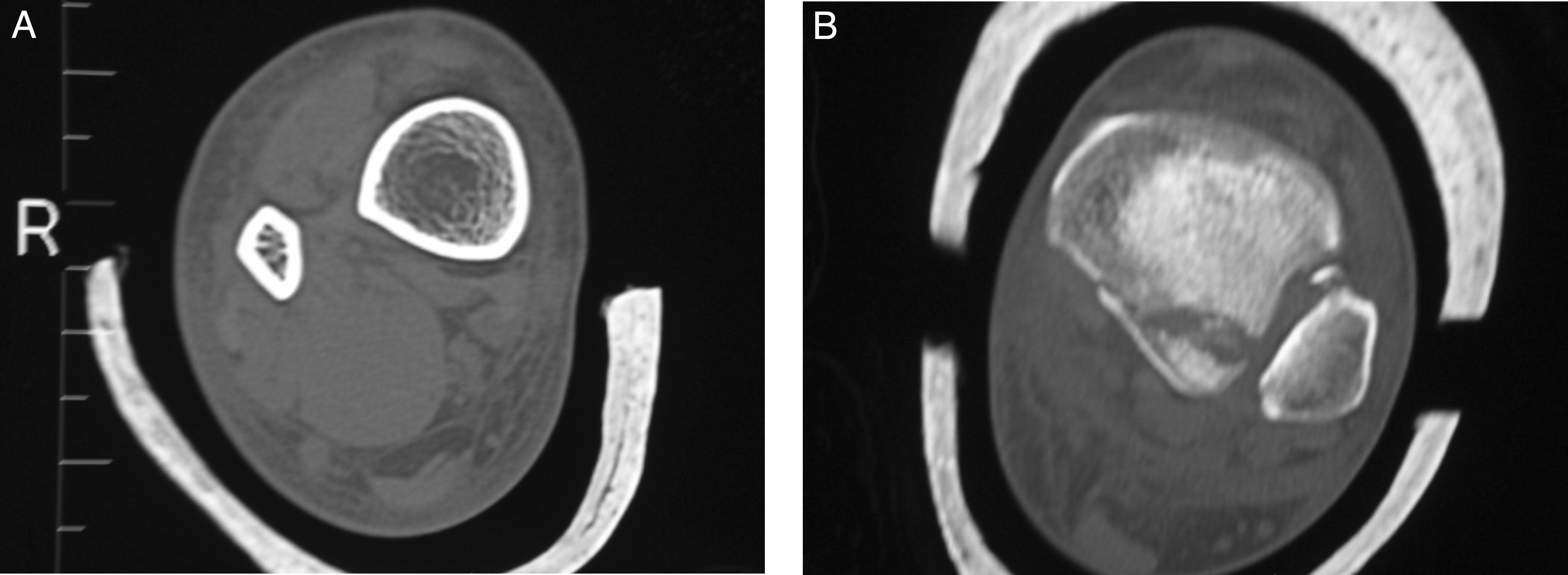
Computer tomography (CT) showing the rotational relationship between the tibia and the fibula in a pronation-external rotation (PER) type IV injury.
In conclusion, our study demonstrated a relative external rotation of the distal fibula fragment in the external rotation mechanism (PER and SER) ankle fracture patterns. These findings were confirmed both quantitatively and qualitatively and are consistent with the rotational deformity classically described for the distal fibular fragment.