
Abstract
Background:
The purpose of this study was to evaluate preliminary results with Kalix® subtalar arthroereisis in sinus tarsi for stage II posterior tibial tendon dysfunction.
Methods:
Twenty-one patients with stage II posterior tibial dysfunction, according to Johnson and Storm, underwent surgical treatment between July 1999 and December 2000. All patients were evaluated clinically using the America Orthopaedic Foot and Ankle Society (AOFAS) hindfoot-ankle score. We performed a tendon repair depending on the type and location of the injury and implanted a Kalix® endorthesis in the sinus tarsi.
Results:
Nineteen patients attended for clinical review with an average follow-up of 27.31 months (range, 19–36). AOFAS scale improved from a preoperative average of 47.2 to an average of 81.6 at revision. The most important improvement was observed in pain (16.3 preoperative to 31.6 postoperative). Two cases required removal of the endorthesis for pain, probably because the endorthesis was too big, without any loss of correction. Patient satisfaction was “satisfied” or “very satisfied” in 17/19. All except three patients would have elected to undergo the same procedure.
Conclusions:
Subtalar arthroereisis by means of implantation of a Kalix® endorthesis in the sinus tarsi, with prior correction of the deformity and tendon repair, offers an alternative to bone operations such as calcaneal osteotomies, lengthening the external column, or arthodesis in patients with stage II posterior tibial dysfunction.
INTRODUCTION
The objective of subtalar arthroereisis in the treatment of flatfoot is to avoid movement of the talus downwards, forwards, and inwards on the calcaneus, and to correct valgus deformity of the hindfoot. This technique originates from Grice's extra-articular arthrodesis, 9 used to correct the valgus deformity in flatfoot of paralytic origin. In the original technique, bone graft from the patient's own tibia was used. Later, several authors used other materials to perform the arthroereisis and to correct flatfoot in children. Enklaar designed a small ivory cone. Viladot 29 used an autologous fragment of fibula, which he replaced some years later for a piece of silastic with a “wine cup” shape. Valenti 26 used an acrylic prosthesis. In 1985, Giannini 8 published his first results with an expanding endorthesis made with polyethylene and a metal screw incorporated in order to effect the expansion.
Numerous publications support the use of endortheses in surgical treatment of flatfoot in children. 1,8,9,14,20,29,30 However, there are few references to their use in adults. 15
The purpose of this report is to present the first results of arthroereisis using the Kalix® endorthesis in the surgical treatment of flatfoot in adults caused by posterior tibial tendon dysfunction, stage II, in accordance with Johnson and Strom's classification. 12
MATERIALS AND METHODS
We included 21 patients with stage II posterior tibial tendon dysfunction, according to Johnson and Strom, 12 who underwent surgical treatment between July 1999 and December 2000. They were all operated on by the same surgeon. Exclusion criteria were overweight, prior surgical treatment of the hindfoot, neuropathic foot, and osteoarthritic foot.
The diagnosis was made by means of clinical examination. All patients complained of pain in the medial side of the ankle and hindfoot which had persisted for more than 6 months, asymmetrical flatfoot with abduction deformity of the forefoot and difficulty in standing on tiptoe on the affected limb (single heel rise test). Mobility of the subtalar joint was preserved or slightly reduced and foot deformity was correctible in all cases. X-rays of both feet were taken in standing position from dorsoplantar and lateral views. The Moreau-Costa-Bartani angle (120°–130°) and Kite's deviation angle (15°–25°) were measured on the x-rays. Clinical diagnosis was confirmed with magnetic resonance imaging, in accordance with Feighan's criteria. 5 All patients were evaluated preoperatively using the American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot and ankle score. 13
Surgical Technique
The patient is placed in supine position with a pillow under the homolateral gluteus in order to reduce external foot rotation and to facilitate approach to the sinus tarsi. Before repairing the posterior tibial tendon dysfunction, the state of the Achilles tendon should be evaluated in order to correct any possible contraction: the leg is held with the knee in complete extension and the hindfoot supinated; in this position, passive dorsal flexion of the ankle should be more than 90°; if it is less, the tendon should be lengthened by performing two percutaneous incisions on its lateral edge and one incision on the medial edge. This procedure will lengthen the tendon allowing correction of valgus deformity.
A skin incision is made over the posterior tibial tendon down to the navicular. Tendinous sheath is opened and the tendon is explored.
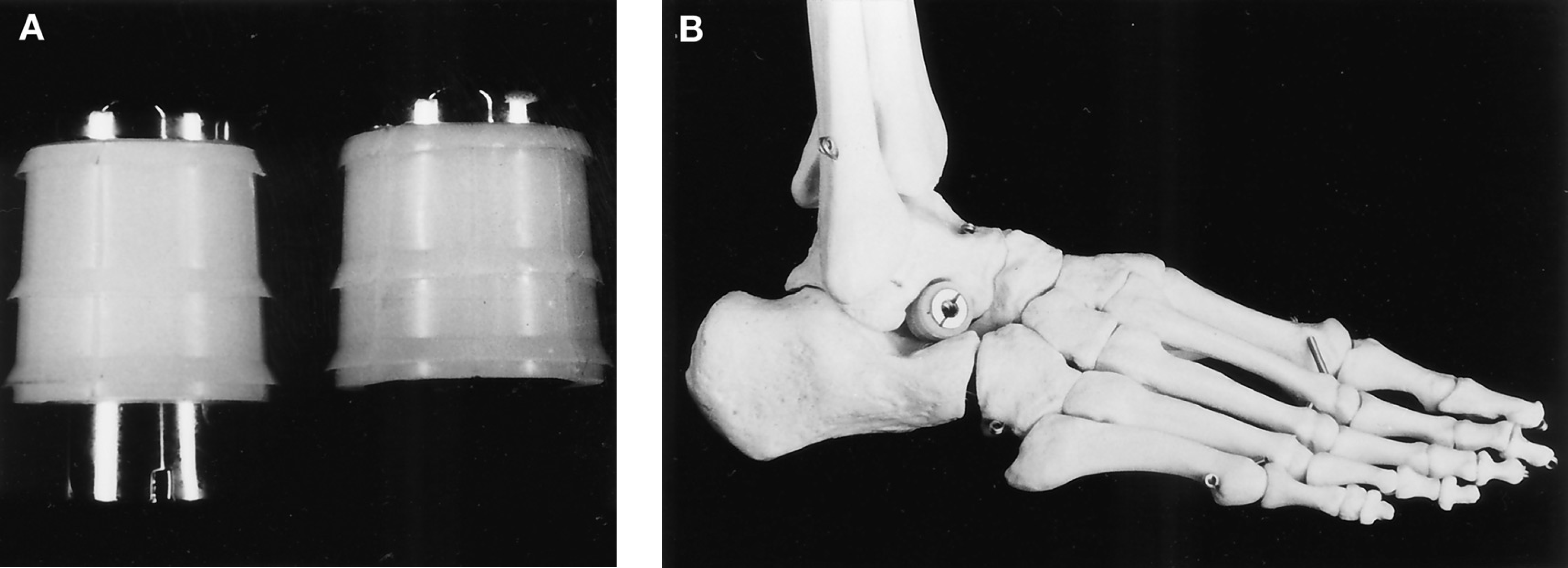
Another incision is made on the lateral side of the hindfoot over the sinus tarsi. The sinus tarsi is emptied (its content is fatty tissue with abundant nerve ends) in order to eliminate the irritative stimuli of the endorthesis in the sinus. Viladot's lever is introduced through the sinus tarsi and under the neck of the talus (Fig. 1A). Now it is time to perform the reduction procedure: supination of the hindfoot (using the lever) and pronation of the forefoot (Fig. 1B). The aim of this maneuver is to raise the head of the talus, close the talocalcaneal angle, and correct the hindfoot pronation. The required endorthesis size is determined using the trial component. The trial component is left in place maintaining the correction while the posterior tibial tendon is repaired.

The tendon repair is then performed. The repair technique used depends on the type and location of the injury. In cases where abundant inflammatory tissue is observed with peritendinous liquid, without tendon tearing, a tenosynovectomy is performed. If there is macroscopic lengthening without tearing, a tendinous plication is performed. If the tendon is torn, its ends are sutured side-to-side to the flexor digitorum longus tendon (FDL). Finally, if the tear is accompanied by marked retraction of the proximal end, the flexor hallucis longus tendon (FHL) is transferred to the navicular. When the tendon injury has been repaired, the definitive endorthesis is implanted and the wound sites are closed in layers. A below-knee compression cast is applied.
Sutures are removed 10–12 days postoperatively and a below-knee walking cast is applied. This cast is removed after 6 weeks and the patient is advised to wear rigid orthopaedic insoles for approximately 6–12 months.
Kalix® Endorthesis
We have been using the Kalix® model (Newdeal SA, Vienne, France) since the end of 1998 for the surgical treatment of flatfoot in children and adults alike. This type of endorthesis basically consists of a metal cone trunk which is introduced into another polyethylene cone trunk which expands (Fig. 2). The polyethylene used is UHMW-PE, equivalent to the one used for total hip replacement. In our opinion, it offers several advantages over other endortheses:
It has been designed and studied at a biomechanical laboratory (C.R.I.T.T. Centre Regional d'Innovation et de Transfert de Technologie, Nogent, France), undergoing static compression tests and tests for fatigue on compression, with excellent results.
Prior studies were performed on cadavers [Departamento de Ciencias Morfológicas (Morphological Science Department), University of Barcelona, Spain].
It is manufactured with biocompatible materials: titanium and high-density polyethylene.
Its conical trunk shape adapts perfectly to the sinus tarsi.
Its expansion mechanism and lateral fins prevent it from being forced out.
Its position in the foot can be controlled on x-ray.
This endorthesis is available in Europe and also in the United States, since it was approved by the Food and Drug Administration in July 2000.
RESULTS
Of the 21 patients who underwent the operation, 15 were women and six were men. Average age was 55.8 years (range, 20–76). In 13 cases the right foot was operated on, and there were eight left foot cases.
With regard to the posterior tibial tendon injury, the procedure used was: tenosynovectomy in eight cases; tendinous plicature in one case; suturing of posterior tibial tendon to the FDL in four cases, and transfer of the FHL tendon to navicular in six cases. The endorthesis size implanted was: #11 in three cases, #12 in six cases, #13 in five cases, #14 in four cases, and #15 in one case. Percutaneous lengthening of Achilles tendon was performed in 11 patients.
Nineteen patients attended for clinical review (Table 1); the other two patients could not be located, and so they were not included in the study. Average follow-up of the 19 patients was 27.31 months (range, 19–36).
Data of the patients included in this study
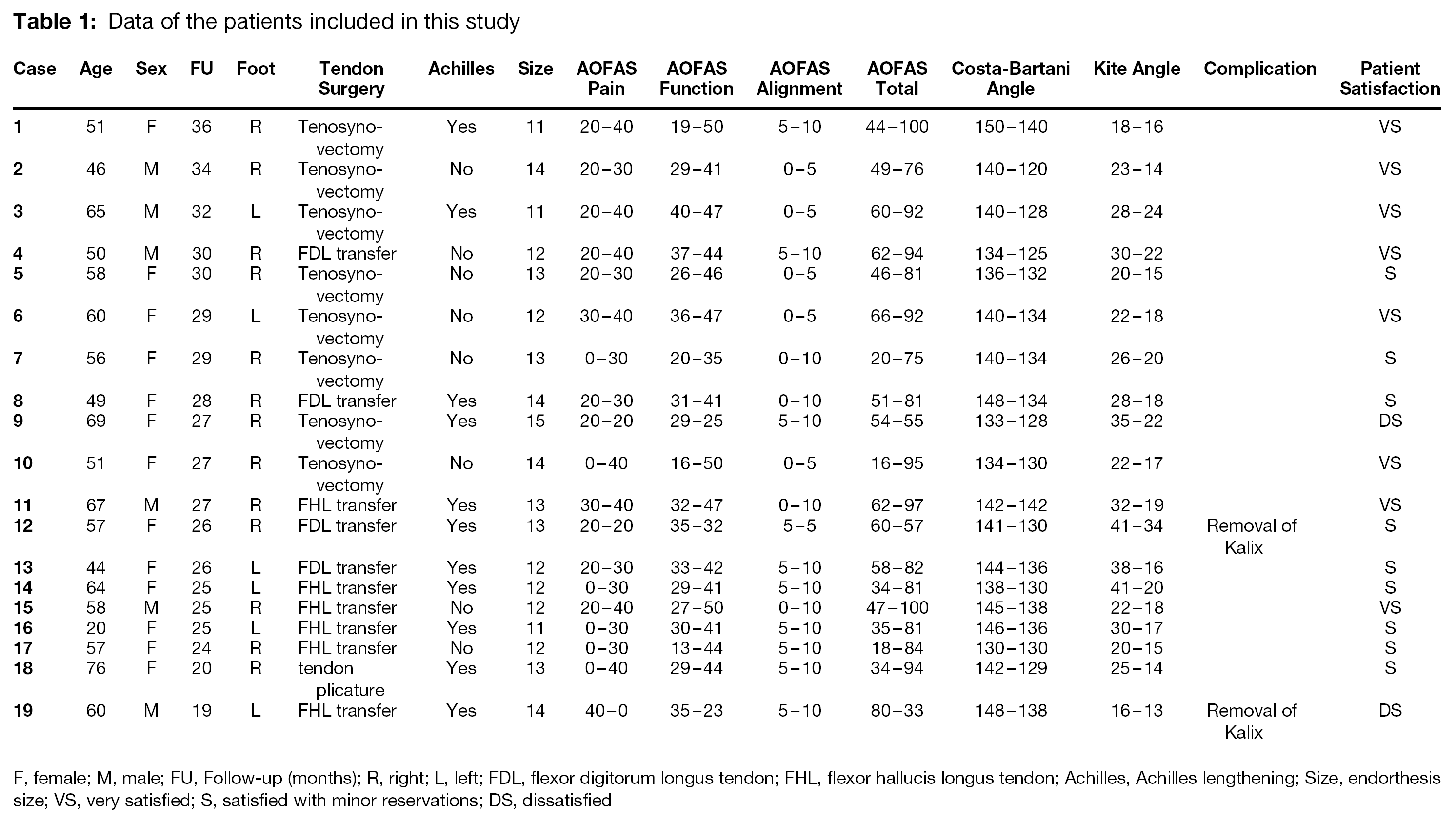
F, female; M, male; FU, Follow-up (months); R, right; L, left; FDL, flexor digitorum longus tendon; FHL, flexor hallucis longus tendon; Achilles, Achilles lengthening; Size, endorthesis size; VS, very satisfied; S, satisfied with minor reservations; DS, dissatisfied
The AOFAS evaluation scale improved notably, from a preoperative average of 47.2 to an average 81.6 at follow-up. If an analysis of the different parameters evaluated on this scale is made, it can be observed that there is an improvement in average pain from 16.3 to 31.6; improved foot and ankle function, with average preoperative value of 28.7 and postoperative value of 41.6; and a variation in alignment with an average value of 2.6 to a follow-up value of 8.4.
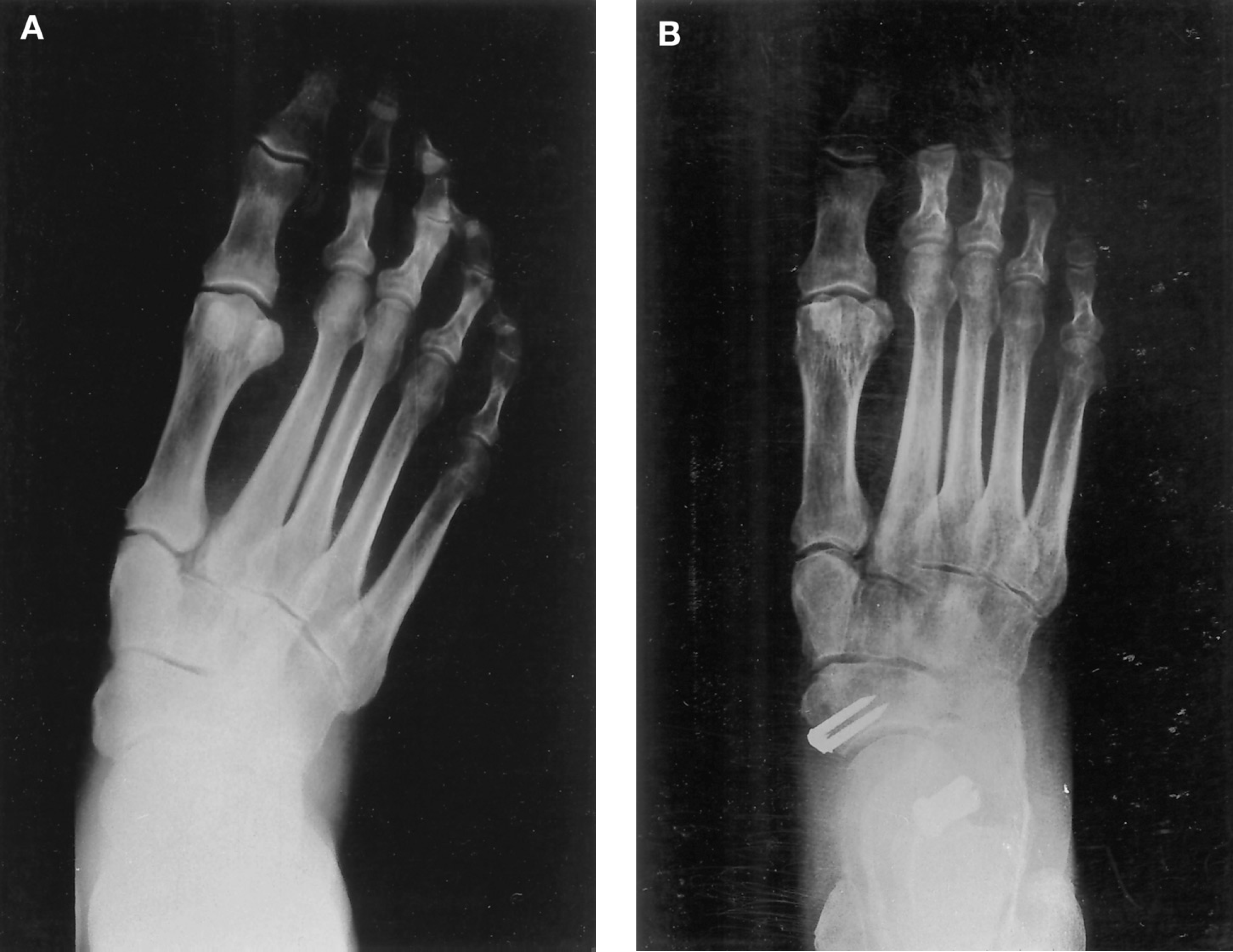
X-ray imaging showed an average reduction in the Moreau-Costa-Bartani angle of 14.3° and an average reduction in the talocalcaneal deviation, Kite's angle, of 8.7° (Figs. 3 and 4). Complications observed in the 19 patients reviewed were limited to some discomfort or pain in the sinus tarsi in six patients, which gradually improved over the first 6 months postoperatively, except for two cases which required removal of the endorthesis after 18 months. A more detailed study of these two cases suggests the failures were due to overcorrection of the talocalcaneal deviation, due to the use of an endorthesis which was too big. We define overcorrection as a clinical varus deformity of hindfoot after surgery.

Patient satisfaction at the time of follow-up was eight very satisfied, nine satisfied with minor reservations, none satisfied with reservations, and two dissatisfied. The two dissatisfied patients were patient 9, because pain did not improve and final result did not reach her expectations, and patient 19, because of unexplained increase of pain after surgery.
All except three patients would have elected to undergo the same procedure again: Two of them were the dissatisfied patients, and the third one was patient 12, who required a second operation (removal of endorthesis) to achieve pain release.
DISCUSSION
If adult flatfoot is the consequence of an uncorrected flatfoot in childhood, there have been anatomical alterations since childhood and adaptation to the same. In these cases, we believe that it is a serious mistake to try to normalize the talus position in the tibia-fibula mortise, as this will lead to ankle arthrosis.
If flatfoot is caused by posterior tibial tendon dysfunction, 17,21 the approach changes; in these patients bone positions are normal until the tendon injury begins to cause the onset of flatfoot. In these cases an attempt should indeed be made to correct the bone positions and to put the talus back into position, providing that the deformity is reducible and that degenerative disorders are not observed in the tarsal joints.
In 1989, Johnson and Strom 12 classified three stages of posterior tibial tendon dysfunction, related to its evolution. For stages I and III there is minimal controversy regarding treatment, but for stage II more treatment options are recommended by different authors. Stage I is characterized by tendinitis, tenosynovitis, and tendinosis, but with absence of hindfoot deformity. Conservative treatment should be followed, 28 and if this fails, tenolysis with or without tenosynovectomy should be performed. 4 Stage III is characterized by severe and irreducible deformity of the hindfoot and treatment requires talonavicular arthrodesis, 10 subtalar arthrodesis, 23 or triple arthrodesis, 6 with or without lengthening of the Achilles tendon.
At stage II, the tendon is more severely affected than at stage I, and there is a reducible deformity of the hindfoot. Many techniques have been described to treat this disorder. The most commonly employed techniques to treat this type of tendon injury are tenolysis with or without tenosynovectomy, 4 end-to-end suture, tendinous plication, dynamic transfer of the FDL or FHL tendons 3,7 or transfer of the FDL or FHL tendons to the navicular, 16 or other type of plasty. 24 Frequently, the use of these techniques alone provides pain relief, but is insufficient to correct the deformity or to prevent recurrences. For this reason, these techniques are often associated with bone operations: calcaneus osteotomies, 11,18,19,22,25 lengthening of the external column, 2 subtalar arthrodesis, 23 or talonavicular arthrodesis. 10 On some occasions it is also necessary to lengthen the Achilles tendon. Positive results have been published on the short-term results of all these techniques, but long-term follow-up reviews are scarce. 27
Subtalar arthroereisis by means of the implantation of an endorthesis in the sinus tarsi, with prior correction of the deformity, offers an alternative to the bone operations mentioned above. It is always associated with a procedure to repair the tendon injury. Endorthesis prevents talus displacement onto the calcaneus, thus eliminating tension on the tendon repair performed. It works as a guide or mechanical support during the repair period, and can then be removed when the dysfunction has been corrected. In our study, in the two cases in which it was necessary to remove the endorthesis, it was not observed that there was any loss of correction or recurrence with regard to discomfort in the internal foot arch. The two removed implants showed no signs of mechanical wear of the polyethylene envelope. We think that the design of the endorthesis is the reason why debris formation is scarce and the implant is well tolerated.
We did not observe loss of strength in big toe flexion in cases in which the FHL was transplanted. This is because of the existence of fibers which join the FHL and FDL tendons. We did, however, observe moderate loss of mobility in the subtalar joint, but we do not believe that this affects resulting foot function. Three patients complained of some awkwardness when walking on uneven ground.
Despite the small sample size and short follow-up period, a more in-depth study of data obtained at patient review permits us to make certain reflections. There is no relation between the cases with the largest increases in AOFAS score and the cases with the largest correction in x-ray imaging measurements. This clinical-radiological discrepancy suggests that it is not essential to normalize x-ray angles to ensure the best outcome for the patient. It would probably be sufficient to block talocalcaneal displacement.
With regard to the different techniques used in tendon repair, in the eight tenosynovectomy cases, the average improvement in the overall AOFAS score was 38.9; in the four suture cases of the posterior tibial to the FDL tendon, the average improvement was 20.7; and in the six cases of FHL transfer to navicular, the average improvement was 33.3. The average improvement overall for the whole group was 34.4. These figures suggest that tenosynovectomy gives better results than other techniques and, probably, this is largely due to the fact that the cases in which tenosynovectomy was performed presented less tendon degeneration. In short, best results are obtained during the initial stages of the disease. This fact supports the need for early intervention in posterior tibial dysfunction, even at stage I with few symptoms, since tendon injuries always tend to get worse.
It is the authors' opinion that, in cases of flatfoot caused by posterior tibial dysfunction, it is better, at a “physiological” or “anatomical” level, to try to correct the valgus deviation of the heel through the subtalar joint than through a calcaneal osteotomy. Also, the implantation of an endorthesis does not rule out the possibility of calcaneal osteotomy or lengthening of the external column if the former fails. Implantation of a Kalix® type endorthesis is easy to perform and requires very simple instruments. Its advantages have already been mentioned.