
Abstract
This study tested the hypothesis that fixation of a fifth metatarsal tuberosity fracture with a lag screw that engages the intact medial cortex is biomechanically stronger than fixation with a long intramedullary screw (control). The right and left feet from 10 male cadavers were alternately assigned to the two fixation groups. After fracture reduction and fixation, each specimen was potted in acrylic cement and tested on a servohydraulic testing machine. The repairs were then distracted until failure by placing the peroneus brevis tendon under tension at a rate of 1 mm/s. The lag screw technique resulted in a significantly greater mean (± SD) load to failure (150 ± 90 N) than did intramedullary screw fixation (70 ± 60 N) (p < .05) and may offer a useful method of internal fixation of fifth metatarsal tuberosity fractures when surgical stabilization is indicated.
INTRODUCTION
Fractures of the fifth metatarsal are the most common of all metatarsal fractures, 3,6,9 and avulsion fractures of the proximal metaphyseal region or tuberosity are ubiquitous. Fifth metatarsal tuberosity fractures are thought to occur when a plantarflexion-inversion force causes the peroneus brevis tendon with or without the lateral band of the plantar fascia to avulse the tuberosity. 9,13,19 Unlike metaphyseal-diaphyseal (Jones) fractures, which have a high rate of delayed healing, tuberosity fractures typically heal in 4–8 weeks with no long-term functional deficits and a low rate of nonunion. 1,2,17,18,20 Nonoperative treatment modalities, such as taping, hard-soled surgical shoe, fracture boot brace, and below-the-knee casting, have been advocated for most tuberosity avulsion fractures. 1,3 –5,8,9,11,20,21 Although most tuberosity avulsion fractures heal successfully with nonsurgical treatment, acute tuberosity fractures in the athlete, fractures with displacement, intra-articular incongruity, or painful nonunion may benefit from open reduction and internal fixation. 2,3,8 –10,16 –18,21 Some investigators have recommended internal fixation for the presence of joint displacement of more than 3–5 mm, a lateral prominence, rotatory displacement, or delayed union. 3,5
There is no consensus as to the optimal method of fixation of fifth metatarsal tuberosity fractures. Recommendations include open reduction and internal fixation via Kirschner wires (K-wires), 3,8 tension band wiring, 12,16 cancellous screws, 18,21 and intramedullary screws. 7,8,17,18 Excision of the proximal fragment has also been discussed. 4,10,17,18
Contemporary orthopaedic literature offers few scientific studies of the effectiveness and clinical outcomes of the various treatment modalities for tuberosity fractures. The objective of the current cadaver study was to compare the strength provided by intramedullary screw fixation with that of lag screw fixation oriented perpendicular to the fracture (engaging the intact medial cortex of the fifth metatarsal). We hypothesized that biomechanical testing would show that lag screw fixation was stronger than intramedullary screw fixation for fifth metatarsal tuberosity fractures.
MATERIALS AND METHODS
Ten pairs of fresh cadaver feet were obtained from the Maryland State Anatomy Board. All specimens were from male cadavers [mean (± SD) age of the specimens, 78 ± 6 years]. None had evidence of fifth metatarsal pathology on physical or radiographic inspection. All specimens were stored in a freezer at–20°C and thawed to room temperature in a saline-soaked cloth. The insertion of the peroneus brevis and the distal 8–10 cm of the tendon were retained; all other soft tissues were dissected from the tendon. During the dissection of each foot, the angular orientation of the peroneus brevis insertion into the proximal fifth metatarsal in both the anteroposterior and lateral planes was recorded. After debridement, a simulated extraarticular fifth metatarsal tuberosity fracture was created with an oscillating microsagittal saw. The osteotomy was oriented perpendicular to the tendinous fibers of the peroneus brevis at the junction of the extra-articular portion of the fifth metatarsal and the articular fifth metatarsocuboid facet, a location chosen to allow the reproducible creation of a simulated fracture.
To minimize potential left/right bias, one foot of each pair was assigned to lag (Lag) screw fixation (with a partially threaded bicortical 4.0-mm cannulated screw; mean length ± SD, 33 ± 2 mm) and the contralateral foot was assigned to intramedullary (IM) screw fixation consistent with common clinical practice (with a partially threaded 4.5-mm cannulated screw; mean length ± SD, 46 ± 1 mm). 17,18,21
Each fracture was reduced and held with a bone tenaculum clamp. In the Lag group, a 1.2-mm-diameter K-wire (guide wire) was driven from the proximal tip of the fifth metatarsal tuberosity, oriented perpendicular to and centered within the fracture site. The K-wire was advanced until it engaged the medial cortex of the metatarsal just distal to the fourth-fifth metatarsal articular facet, and a 2.7-mm cannulated drill was then used to drill over the wire. A second K-wire of identical length was placed alongside the first K-wire to determine the appropriate screw length, and then a 4.0-mm partially threaded cannulated screw was inserted over the guide wire. In the IM group, a 1.2-mm-diameter K-wire was driven from the proximal tuberosity fragment into the distal fragment oriented within the intramedullary canal of the metatarsal. A 2.7-mm cannulated drill was then used to drill over the K-wire. Then a 4.5-mm partially threaded cannulated screw was inserted over the guide wire. The intramedullary screw was long enough to engage the shaft distal to the fracture site by at least 2.5–3 times the diaphyseal diameter. All specimens in both groups achieved acceptable screw purchase, with no cases of stripping of the screw or cortical failure.
The distal aspect of the fifth metatarsal was then prepared for potting by driving two 1.2-mm K-wires perpendicular to each other and the longitudinal axis of the diaphysis, leaving 1 cm of wire exposed in each direction to increase purchase in the potting material. The distal diaphysis was then potted in 2-inch-diameter polyvinyl chloride tubing with a polymethylmethacrylate cement (Fastray, Bosworth, Skokie, IL) (Fig. 1). The proximal aspect of the peroneus brevis was then attached to a custom-machined tendon clamp and the polyvinyl chloride pipe was secured to the table of a servohydraulic testing machine (8531, Instron, Canton, MA). The tendon was placed in the same angular orientation in the anteroposterior and lateral planes as was measured in the original specimen (Fig. 2). Tension was then applied in a longitudinal direction along the direction of the fibers of the tendon at a rate of 1 mm/s until the tendon ruptured or the fixation construct failed. The pattern of failure for each specimen was recorded. The load-to-failure value, defined as the maximum load sustained before a precipitous drop in the load-versus-deformation curve, was recorded for each specimen. The difference in load to failure between the two methods of fixation was analyzed for significance (p < .05) with a paired t test.
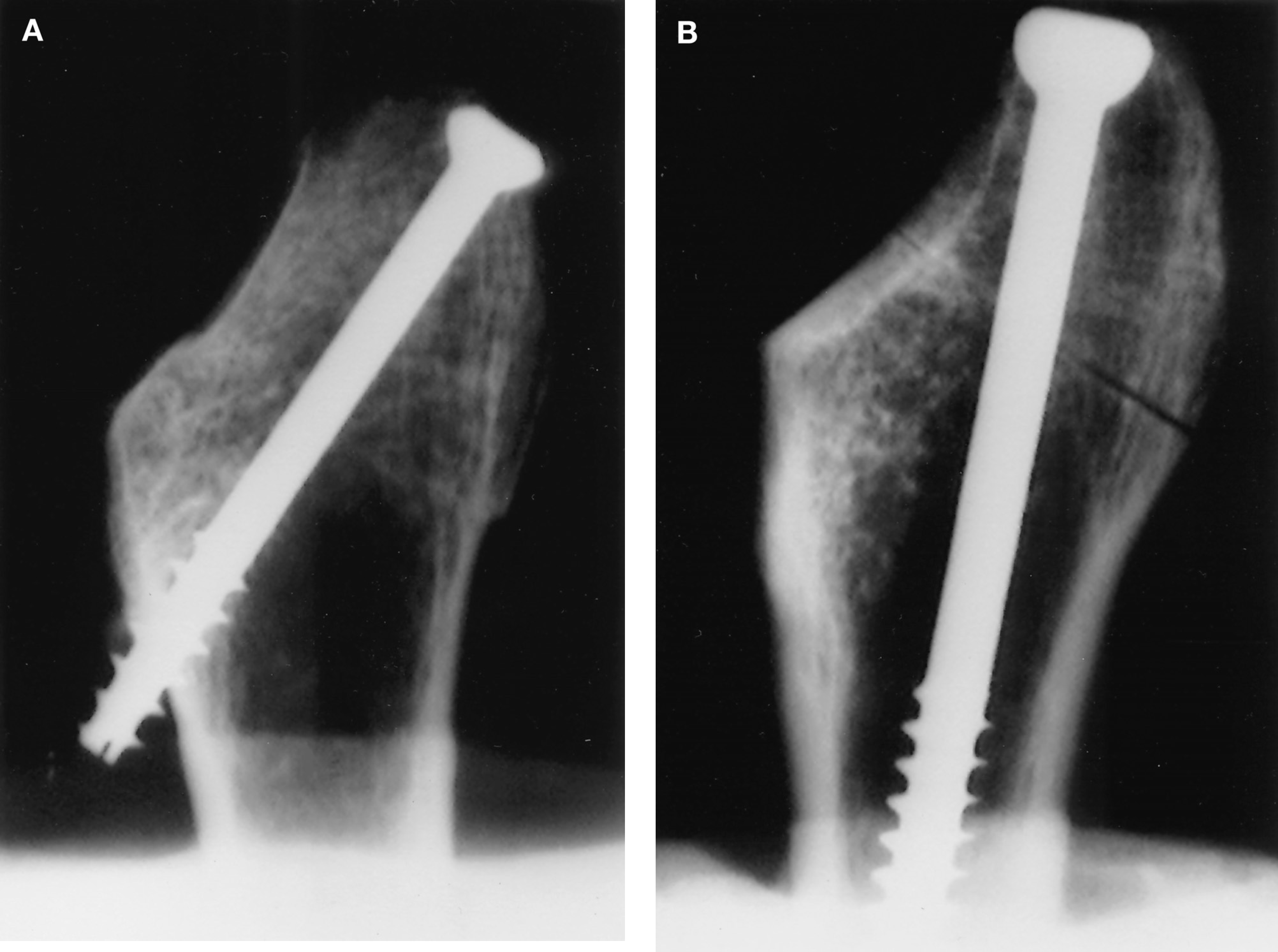
Radiograph of lag screw (
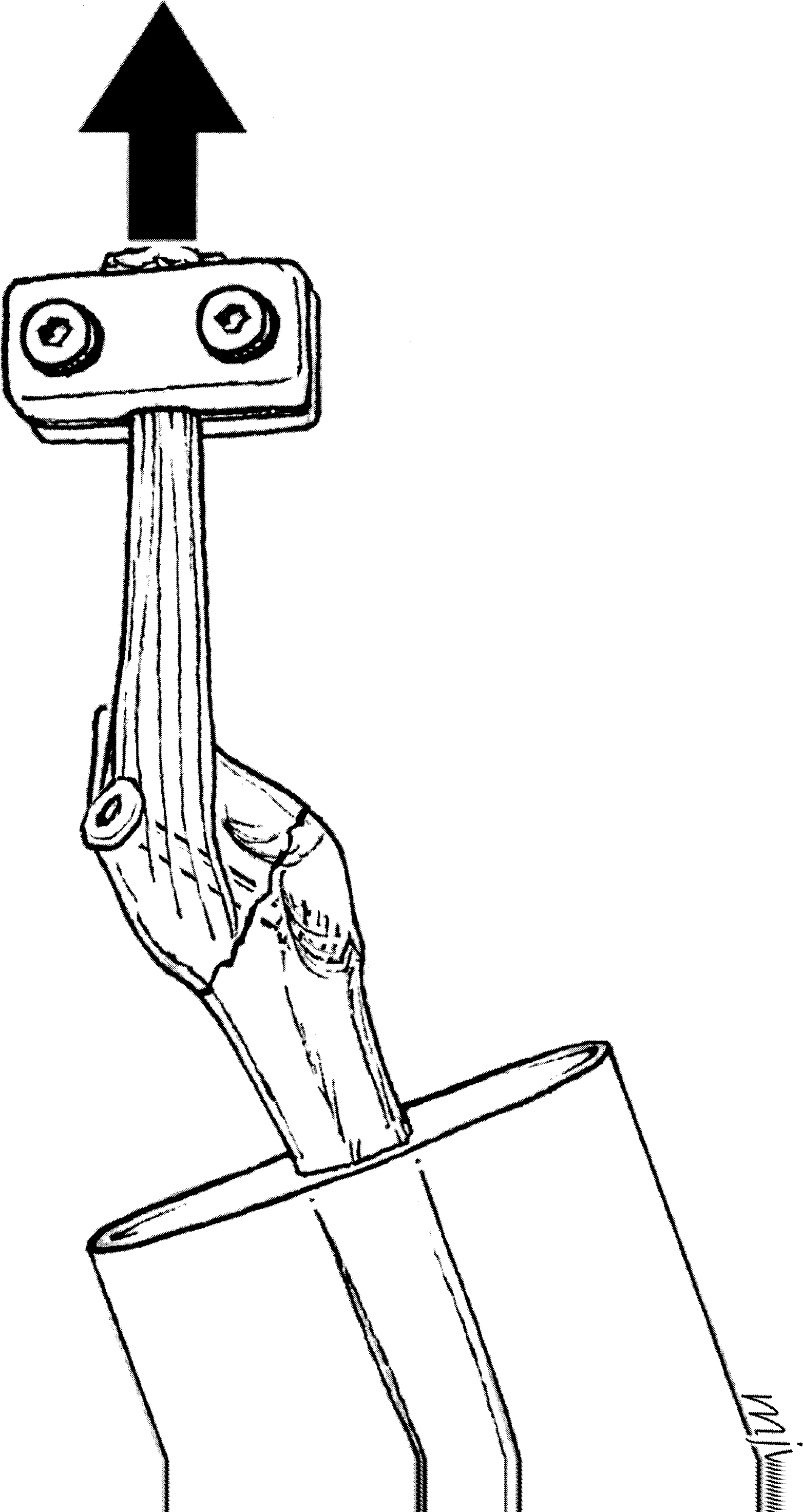
Schematic of specimen in testing apparatus.
RESULTS
The lag screw technique resulted in significantly stronger fixation than the IM technique: mean loads to failure (± SD) were 150 ± 90 N and 70 ± 60 N (p < .05), respectively. In the lag group, the specimens failed by proximal fragment pull-off from the screw head (seven specimens), proximal fragment fracture (two specimens), and peroneus brevis tendon pull-off from the actuator clamp (one specimen). In all 10 specimens, the lag screw remained engaged to the distal fragment. In the IM group, specimens failed by screw pull-out from the intramedullary canal (seven specimens) and proximal fragment pull-off from the screw with the shank still engaged in the canal (three specimens).
DISCUSSION
We found that the bicortical interfragmentary lag screw fixation provided significantly stronger fixation than the intramedullary screw technique. Our results support the findings 6 that bicortical screw fixation perpendicular to the fracture line is stronger than other methods of fixation and may facilitate healing in patients for whom surgical treatment is recommended. That study, which was conducted on foam models and a small number of unpaired cadaver specimens, showed that bicortical screw fixation was mechanically stronger than tension band wiring. 6 To the best of our knowledge, the current ex vivo study is the first paired cadaver study to address the biomechanical efficacy of the bicortical lag screw fixation for these fractures.
Some investigators have recommended internal fixation for joint displacement of more than 3–5 mm, the presence of a lateral prominence, rotatory displacement, or delayed union. 3,5 The senior author (JTC) has also successfully used internal fixation for acute fractures in athletes. The long intramedullary screw has for many years served as a common method of fixation for all proximal fifth metatarsal fractures, including Jones fractures, proximal diaphyseal stress fractures, and, to a lesser extent, metaphyseal avulsion fractures. 4,7,17 The most commonly used screw has been a 4.0- or 4.5-mm-diameter partially threaded screw to allow for fracture site compression. 8,10,11,15,18,21 In a series of eight symptomatic tuberosity nonunions, three patients were treated by intramedullary 4.0-mm screws and had excellent results. 18 However, such fixation is oriented obliquely to the longitudinal axis of the metatarsal and does not provide compression perpendicular to the plane of the typical tuberosity avulsion fracture. 14 Furthermore, placement of such a screw can be technically more challenging, risks fracture of a fifth metatarsal with a very narrow isthmus, and may create a stress riser at the distal tip of the screw, possibly increasing the risk of a more distal shaft fracture.
A possible limitation of our study was the use of cadaver specimens to simulate the in vivo state. Although we used male specimens to minimize the effect of osteoporosis, the cadaver specimens were from geriatric individuals and may have had diminished bone mechanical properties compared with patients typically treated for tuberosity avulsion fractures. Nevertheless, because the study was conducted using paired specimens, we would expect the relative differences in fixation strength to remain, even if overall bone strength is greater in younger patients. A larger diameter screw to engage the intramedullary bone might improve the strength of that technique; however, most authors have recommended 4.0- or 4.5-mm-diameter intramedullary screws to allow passage within a narrow diaphyseal isthmus and minimize the risk of intraoperative fracture. 17,18,21 Finally, our biomechanical testing protocol may not have fully recreated the three-dimensional in vivo stresses applied to the proximal fifth metatarsal, but it nevertheless showed that bicortical lag screw fixation for fifth metatarsal tuberosity avulsion fractures was stronger than intramedullary screw fixation in a cadaver model.
Footnotes
ACKNOWLEDGMENTS
The authors wish to acknowledge Synthes, U.S.A. (Paoli, PA) for donating the screw implants.