
Abstract
The purpose of this study was to investigate the effect on gait in patients who underwent reconstruction for stage II posterior tibial tendon (PTT) dysfunction. Twelve patients with stage II PTT dysfunction underwent surgical reconstruction consisting of debridement of the posterior tibial tendon, flexor digitorum longus tendon transfer to the navicular tuberosity, medial displacement calcaneal osteotomy, and spring ligament reconstruction. Midfoot arthrodesis was performed in six patients and gastrocnemius recession in three. Gait analysis was performed 2 weeks prior to surgery and 1 year postoperatively. Preoperative and postoperative data were compared to determine differences in temporal-spatial parameters, lower limb kinematics, and ankle push-off power. Step length for the operated side increased from 52.6 ± 9.6 cm before the surgery to 57.5 ± 7.1 cm after the surgery (p = .048). Cadence improved from 100.2 ± 10.7 steps/min to 109.1 ± 8.5 steps/min (p = .05), thus increasing velocity from 87.6 ± 22.6 cm/s to 103.4 ± 15.9 cm/s (p = .042). Single support percentage was unchanged. Maximum sagittal ankle joint power at push-off increased from 0.79 ± 0.35 W before surgery to 1.2 ± 0.5 W after surgery (p = .042). There were statistically significant improvements in all radiographic parameters studied. This is the first prospective study to evaluate the in vivo effects on gait in patients undergoing this common surgical procedure. Analysis demonstrated statistically significant improvement in kinetic and kinematic parameters of gait function.
Keywords
Introduction
Posterior tibial tendon (PTT) dysfunction is the major cause of acquired adult flatfoot deformity. 12,21 The pathophysiology has been described to evolve through a series of stages which are characterized by well recognized symptoms, clinical signs, and roentgenographic changes. 8 Because of the broad spectrum of disease, there are a variety of conservative and operative procedures that are based on the pathologic anatomy. 14 During the earlier phases of this degenerative process, the foot is flexible and passively correctable but lacks dynamic support. While recent studies of repair and reconstruction of the spring ligament have also been reported, 4,6 the most commonly performed surgical reconstruction at this time consists of flexor digitorum tendon transfer to provide motor substitution concomitant with medial displacement osteotomy to address the valgus hindfoot deformity. 19,20,22 While the surgical indications and techniques are well accepted for clinically demonstrable deformity, there are no prospective studies of the effect of these widely performed reconstructions on a patient's gait. The hypothesis of this study was that patients after reconstruction for posterior tibial tendon dysfunction will have significant improvements in gait parameters, specifically temporal-spatial parameters and ankle power.
Materials and Methods
Posterior tibial tendon reconstructions were performed on 12 consecutive patients (11 female and 1 male) with clinically demonstrable stage II PTT dysfunction. The patients all had severe weakness of posterior tibial strength on manual motor testing, demonstrating inability to invert the foot from an everted position or to resist eversion maneuvers in the inverted position. All patients had pain, tenderness, and swelling over the tendon, and inability to do single-limb toe raises. MRI documented enlargement and abnormal signal in the posterior tibial tendon consistent with chronic tear of the tendon. The subjects had an average age of 58.1 ± 6.5 years, an average height of 167.3 ± 7.8 cm, and an average weight of 80.3 ± 19.7 kg.
Surgical Procedures
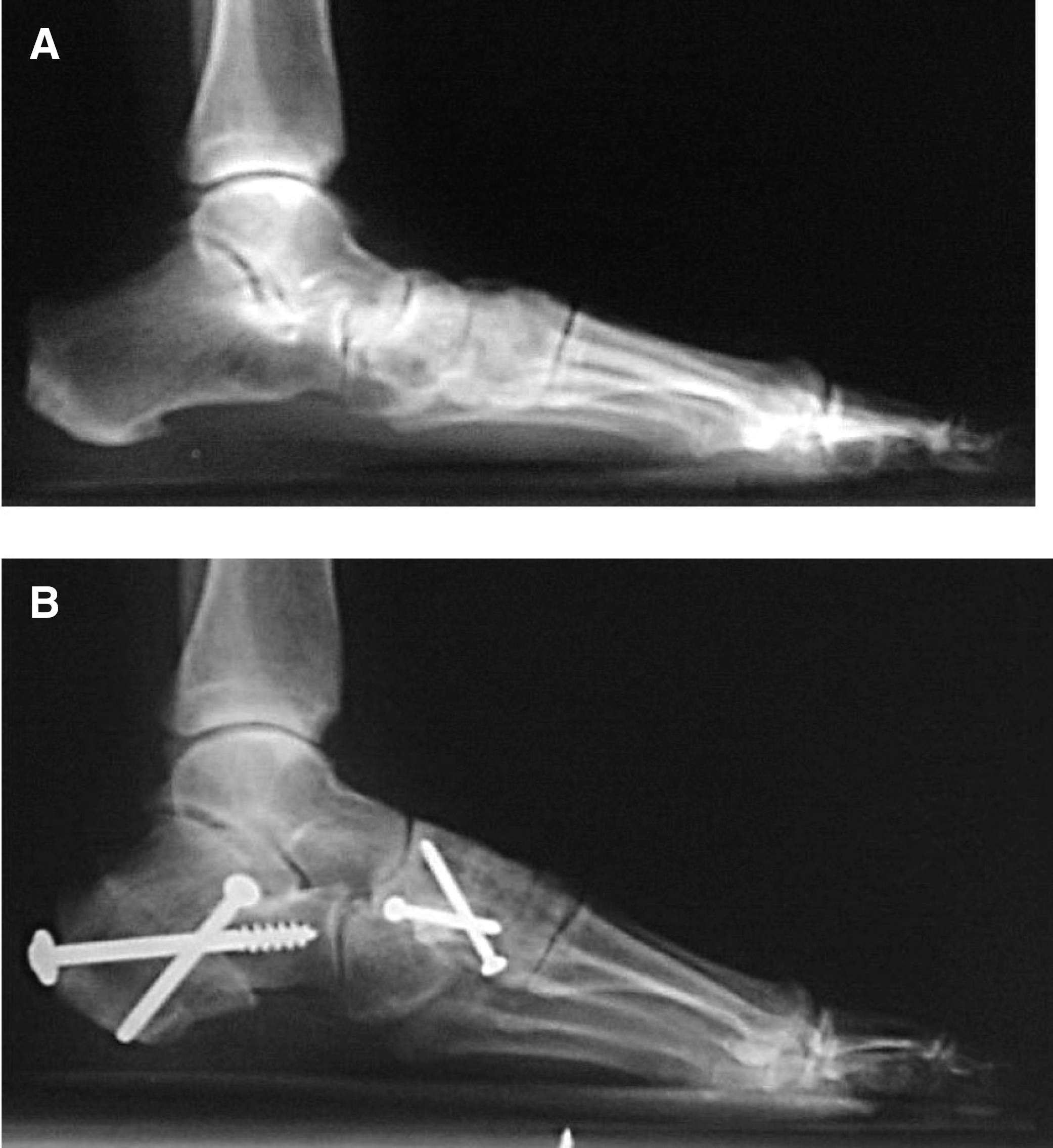
The reconstructive procedures were comprised of debridement of the degenerative posterior tibial tendon, flexor digitorum longus tendon transfer to the navicular tuberosity, medial displacement calcaneal osteotomy, and imbrication of the spring ligament. In addition, three naviculocuneiform and three first tarsometatarsal arthrodeses were performed in six patients for dorsal subluxation and arthrosis as demonstrated on standing lateral radiographs. Three patients required gastrocnemius recessions for contracture. Figure 1 depicts preoperative and postoperative lateral radiographs of a case after posterior tibial tendon reconstruction including midfoot arthrodesis. The nonparallel, dual-screw fixation technique of the calcaneal osteotomy is shown.
Preoperative (
Radiographic Analysis
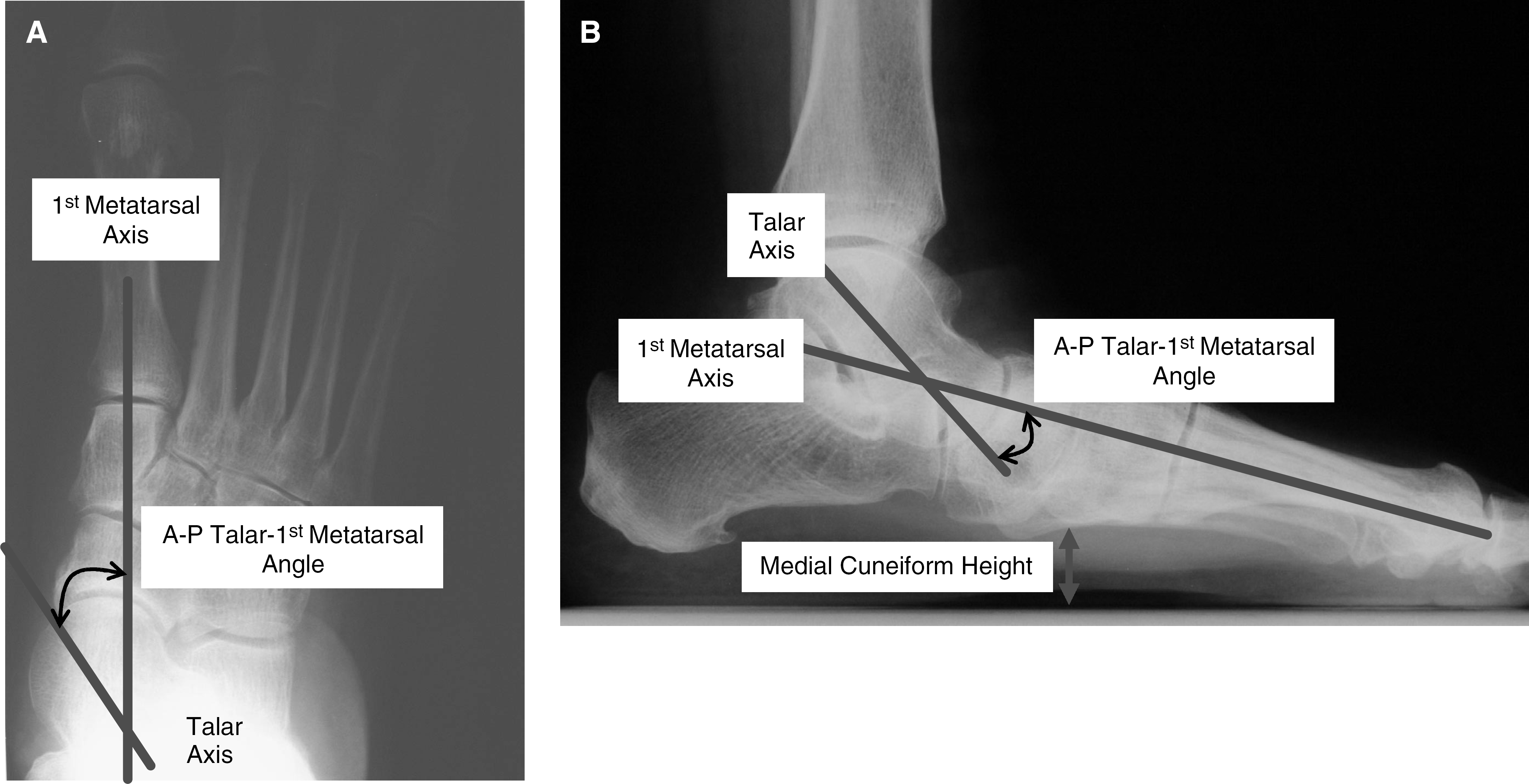
Talar–first metatarsal angles were determined in anteroposterior and lateral planes, and medial cuneiform height (mm) was measured in the lateral plane (Fig. 2, A and B). Statistical analysis was performed using paired t tests and significance was set at p < .05.
Gait Analysis
A gait analysis study was performed 2 weeks prior to surgery and repeated 1 year postoperatively. Preoperative and postoperative data were compared to determine differences in temporal-spatial parameters and push-off ankle power. Kinematic and kinetic parameters were collected using a five-camera Motion Analysis System (Motion Analysis Corporation Inc., Santa Rosa, CA) and AMTI OR6–5 force platform (Advanced Medical Technology, Inc., Newton, MA), recording at 1000 Hz, which is embedded in the center of an 8-m walkway. Inverse dynamics were used to derive kinetic information from the kinematic and ground reactive force data. Reflective markers were secured to anatomic locations with adhesive tape using the Helen Hayes Marker configuration. 9 Markers were placed bilaterally over the anterior superior iliac spine, over the lateral knee epicondyle, over the lateral malleoli, on the forefoot over the head of the third metatarsal, and on the posterior aspect of the heel at the same level as the marker over the third metatarsal head. Short 9-cm and 6-cm wands, with markers attached to the ends, were also secured laterally to the midthigh and midshank regions. These were in line with the greater trochanter and lateral knee epicondyle marker for the thigh wand and lateral knee epicondyle and lateral malleoli markers for the shank wand. Markers were also placed over the medial malleoli and knee medial epicondyle for collection of a static trial just before testing to identify the centers of the ankle and knee joints, respectively.
Subjects were then requested to walk barefoot at a self-selected pace on the level 8-m walkway. Data were collected until five “good” trials were recorded for each limb. A “good” trial was defined as the patient striking the force platform, with one foot completely encompassed by the force platform. Patients were allowed breaks whenever necessary. The collected data were normalized to the gait cycle for each trial, and the results were then averaged for statistical analysis.
Statistical comparisons were made of the patient's limb that underwent surgery both pre- and postoperatively. Temporal-spatial parameters including velocity, stride length, and step width were normalized for patient height and then analyzed. Ankle, knee, and hip kinematic patterns were analyzed at six distinct periods during the stance phase of the gait cycle. These periods were heel strike, first ankle rocker, second ankle rocker, heel rise, third ankle rocker, and toe-off. Maximum knee flexion during swing and maximum hip extension at terminal stance were also analyzed. Kinetically, peak ankle power in the sagittal plane, as well as knee varus and flexion moments, were extracted from the data. A paired t test was used to compare the differences in the temporal-spatial, kinematic, and kinetic parameters. In all cases, statistical significance was set at p < .05.
Results
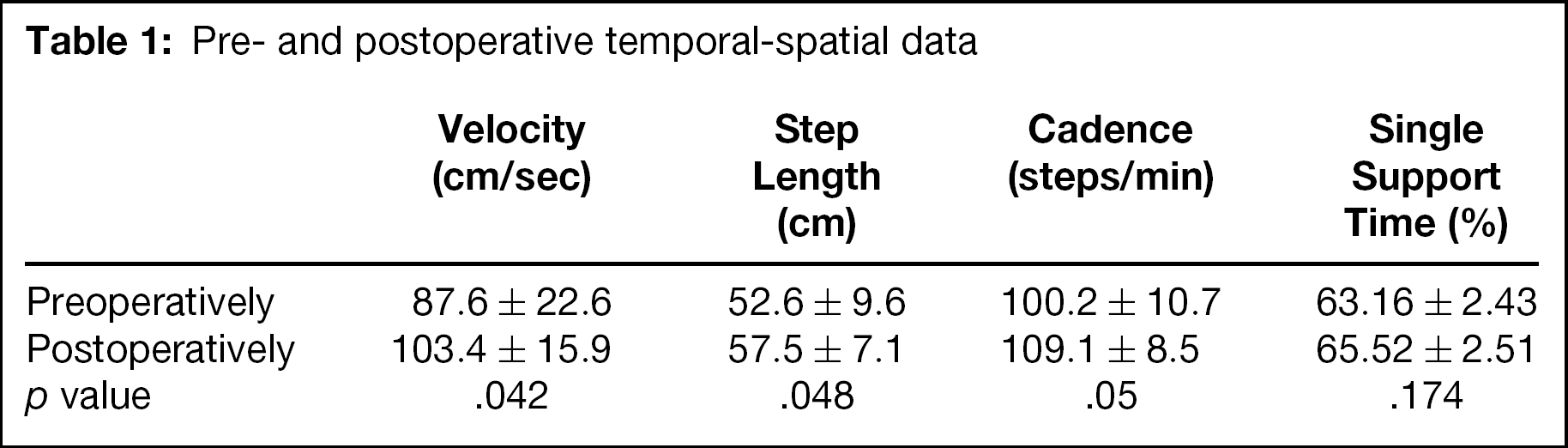
Of all tested parameters, step length, cadence, velocity, single support time, and maximum ankle power were most applicable to the reconstruction of the posterior tibial tendon (see Table 1 and Fig. 3). On the average, velocity increased from 87.6 ± 22.6 cm/s to 103.4 ± 15.9 cm/s (p = .042). This increase was due to independent significant increases both in step length and in cadence. Step length for the operated side increased from 52.5 ± 9.6 cm before the surgery to 57.5 ± 7.1 cm after the surgery (p = .048). Cadence improved from 100.2 ± 10.7 steps/min to 109.1 ± 8.5 steps/min (p = .05). Single support percentage was unchanged. Maximum sagittal ankle joint power at push-off increased from 0.79 ± 0.35 W before surgery to 1.2 ± 0.5 W after surgery (p = .042) (see Fig. 3). There were no significant changes in the lower limb kinematics of the hip or knee.
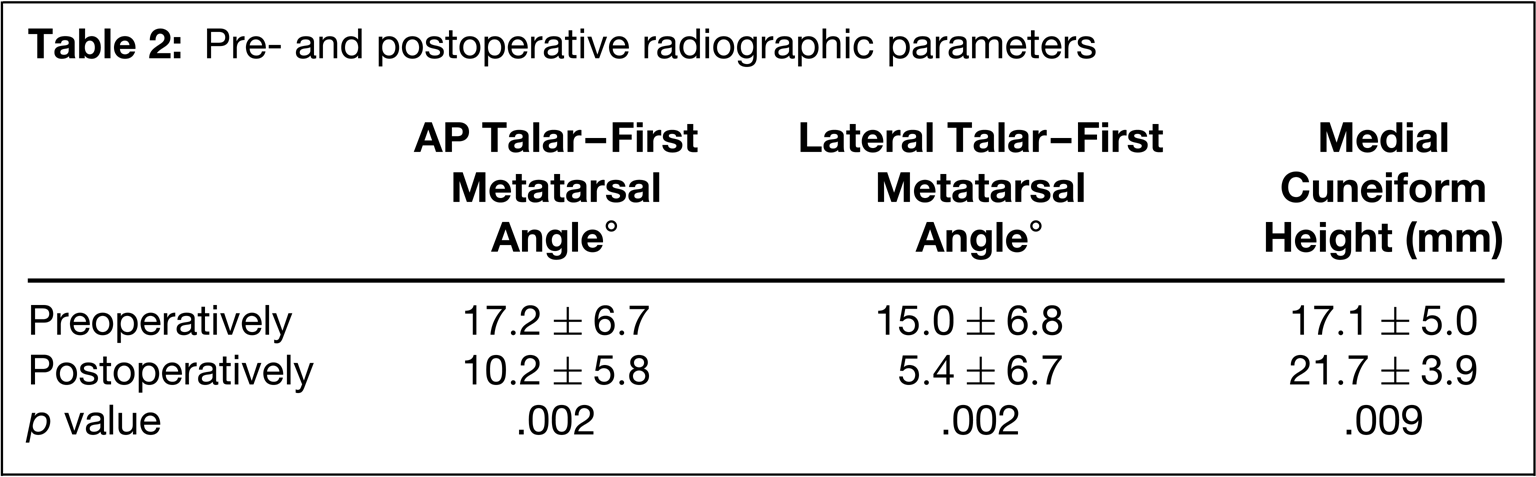
Radiographic analysis showed improvements in all parameters studied. The anteroposterior talar–first metatarsal angle decreased from a preoperative average of 17.2° ± 6.7° to 10.2° ± 5.8° postoperatively (p = .002). The lateral talar–first metatarsal angle decreased from a preoperative average of 15.0° ± 6.8° to 5.4° ± 6.7° postoperatively (p = .002). The medial cuneiform height increased from a preoperative average of 17.1 ± 5.0 mm to 21.7 ± 3.9 mm postoperatively (p = .009) (see Table 2).
Pre- and postoperative temporal-spatial data
Pre- and postoperative radiographic parameters
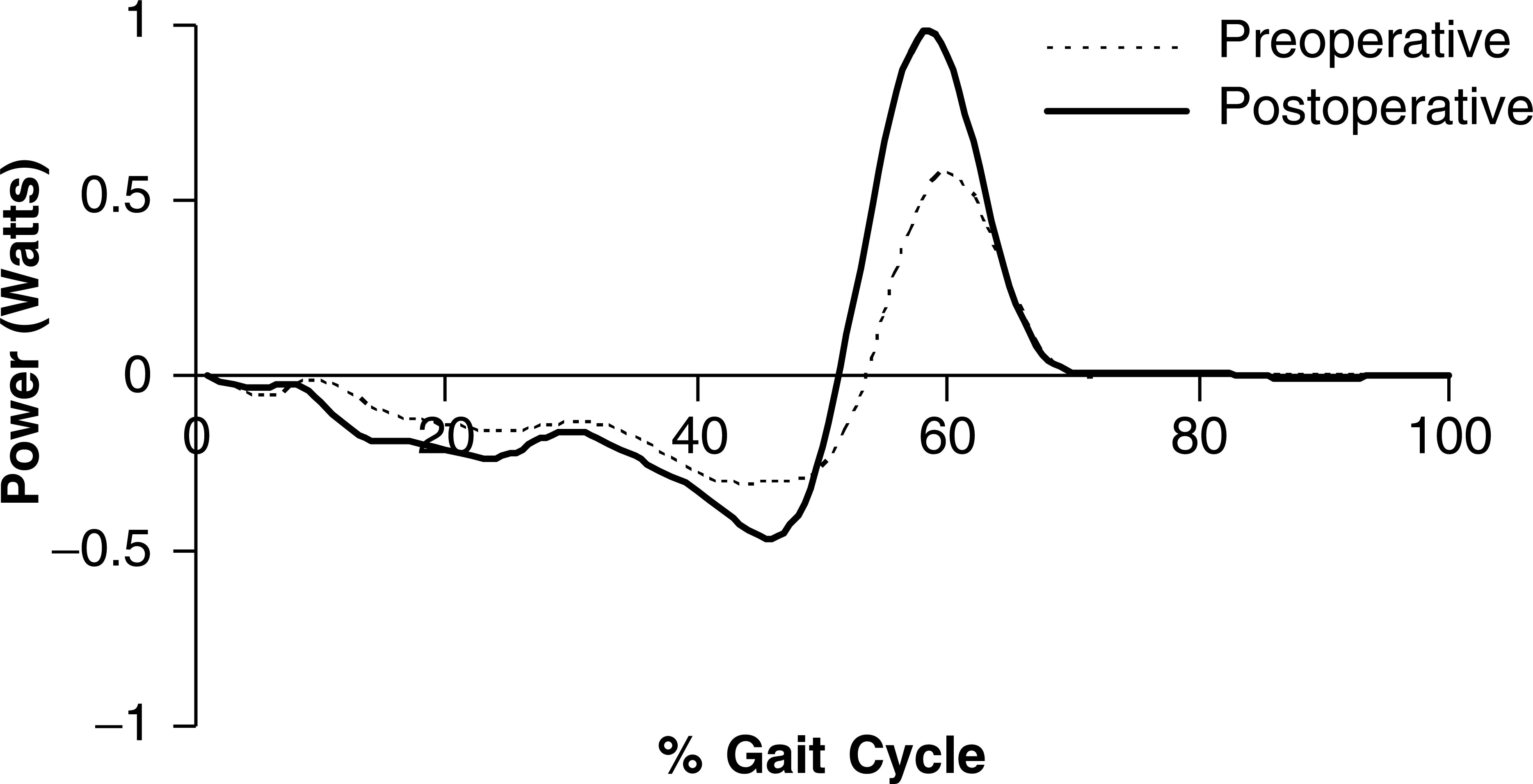
Graph of maximum sagittal ankle power showing significant improvement after reconstruction procedures.
Discussion
Cadaver studies have verified the effect of the tibialis posterior muscle on the arch of the foot in simulated weightbearing models. 10 When all tendons except the tibialis posterior were loaded, arch flattening or a mild pes planus deformity resulted. Loading the tibialis posterior produced normal arch alignment.
In normal gait, the tibialis posterior muscle produces inversion of the hindfoot. 6 It is also an adductor of the forefoot at the midtarsal joint opposing the action of the peroneus brevis. The posterior tibial muscle functions during the stance phase of gait. 17 After heel contact, the muscle acts as a shock absorber for the subtalar joint limiting hindfoot eversion by eccentric contraction. During midstance, its contraction causes subtalar inversion locking the transverse tarsal joints. This results in a rigid lever for forward propulsion of the foot by allowing the powerful gastrocnemius-soleus complex to act through the foot at the metatarsal heads. During the propulsive phase, the tibialis posterior functions to accelerate subtalar joint supination and assists in heel lift. The shift of the body weight center from lateral to medial through the longitudinal axis of the foot during the propulsive phase of gait is achieved by the balanced activity of the tibialis posterior and peroneal muscles. The posterior tibialis muscle then becomes inactive shortly after heel lift, with the residual effect of acceleration during swing phase. 7,17
With dysfunction the balance is weighted toward the peroneals with greater hindfoot eversion and ligamentous tension and stretching during the contact phase. In midstance there is decreased inversion of the subtalar complex, such that the hindfoot cannot function as a rigid lever. The gastrocnemius-soleus then acts at the talonavicular joint creating excessive midfoot stress, allowing increased midfoot abduction, as well as producing a levering action at the tarsometatarsal joints. In the propulsive phase, there is less lateral column loading and a delayed heel lift that reduces the magnitude of propulsive activity. The repetitive biomechanical alteration of gait results in progressive midfoot collapse, forefoot abduction, and excessive hindfoot valgus. 7,8,15
It is important for the surgeon to understand these normal biomechanical functions of the foot in order to comprehend the evolution of the complex and progressive deformity caused by dysfunction of the posterior tibial tendon. In theory, the surgical reconstruction of posterior tibial tendon should address as many of these biomechanical functions (or the lack thereof) as possible, in order to reverse or compensate for the lost function. Previous studies have demonstrated the shift of the weightbearing line medially as a result of calcaneal osteotomy. 3,22,23 In addition to this direct mechanical effect of the surgical procedure, the medialization of the Achilles tendon insertion most likely augments the inversion power of the gastroc-soleus.
Surgical indications and techniques for established stage II posterior tibial tendon dysfunction have been well described in the literature. 1,2,5,11,13,14,16,18 -20,22 It is well recognized clinically that while the surgical reconstruction cannot restore normal function of the hindfoot, nor full function or power of the posterior tibial muscle, the procedures have proven merit in reducing pain and improving patient outcome. 1,2,5,11,13,14,16,18 -20,22 The relation of these clinical observations and studies to the quantifiable biomechanical changes in vivo has not been previously studied, to the best knowledge of the authors.
This preliminary study has a small sample size but shows significant improvement in kinetic and kinematic parameters of gait function in patients who have undergone this form of reconstruction of the posterior tibial tendon. It shows significant improvements in parameters affected directly by posterior tibial muscle action during gait, including velocity, step length, cadence, and sagittal ankle power.
We are undertaking further studies to expand our ability to distinguish the effects of variations in the surgical technique for reconstruction of the posterior tibial tendon, such as midfoot arthrodesis and gastrocnemius recession. This study documents the objective changes in function of the ankle and lower extremity as a result of this surgery. It is the authors' hope that these data provide objective quantification of the functional changes effected by this surgery, and that they will contribute to the establishment of measurements by which future advances may be quantified.
Footnotes
Acknowledgement
The authors wish to acknowledge the generous endowment of the Motion & Performance Laboratory at Baylor University Medical Center by the Robert and Ruby Priddy Foundation.