
Abstract

INTRODUCTION
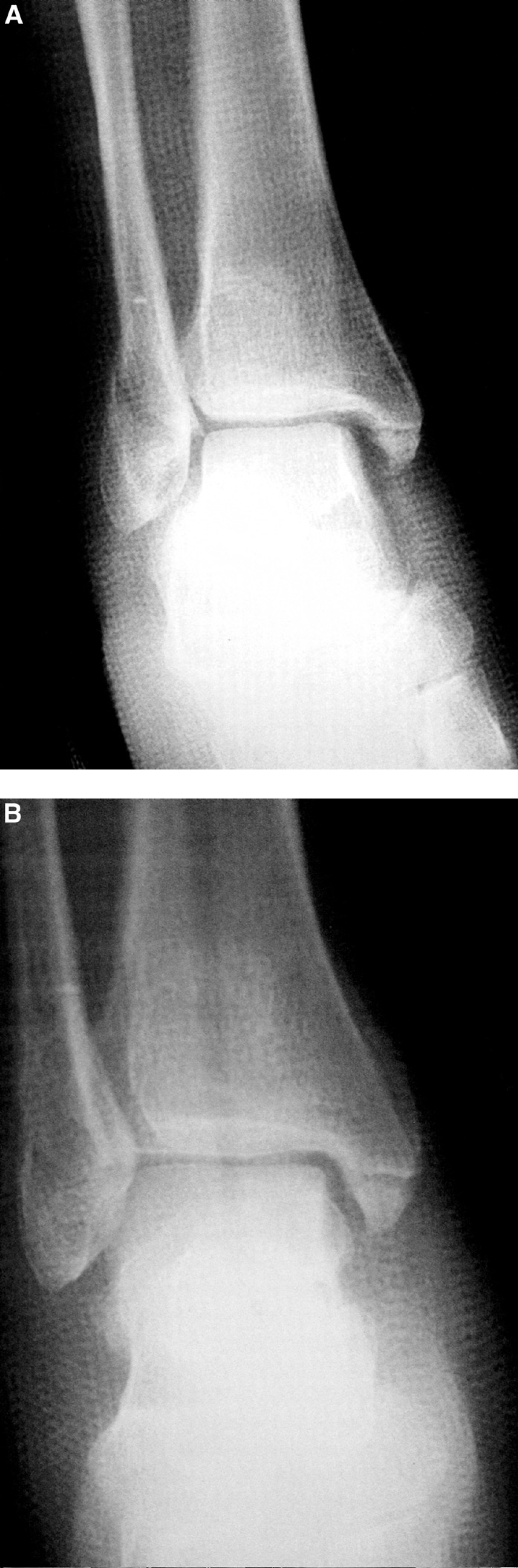
The treatment of trimalleolar fractures and the fixation of the posterior malleolar fragment have been discussed and recommended under certain circumstances 1,2 (Fig. 1). This is sometimes necessary when reduction of the lateral malleolar fracture does not lead to adequate reduction of the posterior malleolar fragment. 2 There are, however, few surgical techniques 3,4 described to facilitate this fixation. The authors present a surgical approach to the posterior and medial malleoli previously described by Edgar L. Ralston 1 in 1951. This description was published when open reduction and internal fixation of displaced medial and posterior malleolar fractures was relatively uncommon. This approach allows fixation of these two fractures under direct vision, through the same incision, while at the same time allowing direct examination of the distal articular surface. It then involves posterior dissection, mobilization, and anterior retraction of the tendons of the posterior tibialis and flexor digitorum longus. The posterior fracture fragment is then visible and can be treated under direct vision.
TECHNIQUE
A longitudinal incision is made over the medial malleolus extending from approximately 5 cm proximal to the tip past the malleolus, and then taking a gentle curve anteriorly at the tip of the medial malleolus (Fig. 2). This incision is optimally placed midway between the anterior and posterior edges of the medial malleolus; however, if a previous incision exists that is more anterior or posterior than midline, this can often be incorporated. The incision is extended to the bone, and dissection is performed posteriorly to the tarsal retinaculum. The posterior tibial tendon (PTT) sheath along with the flexor digitorum longus (FDL) tendon sheath are then opened longitudinally. The tendons are encircled with an umbilical tape or penrose drain and retracted anteriorly (Fig. 3). As the tendons are retracted anteriorly, the posterior medial aspect of the distal tibia is visualized. Periosteal dissection can be carried out posteriorly and laterally until the posterior malleolar fracture is visualized. Care should be taken to avoid injury to the neurovascular structures which are directly posterior to the dissecting instruments.

The incision to be utilized is marked out over the medial malleolus.

The posterior tibial tendon and the flexor digitorum longus tendons are retracted anteriorly after the sheaths are opened. The fracture can be visualized posteriorly to the tendons.
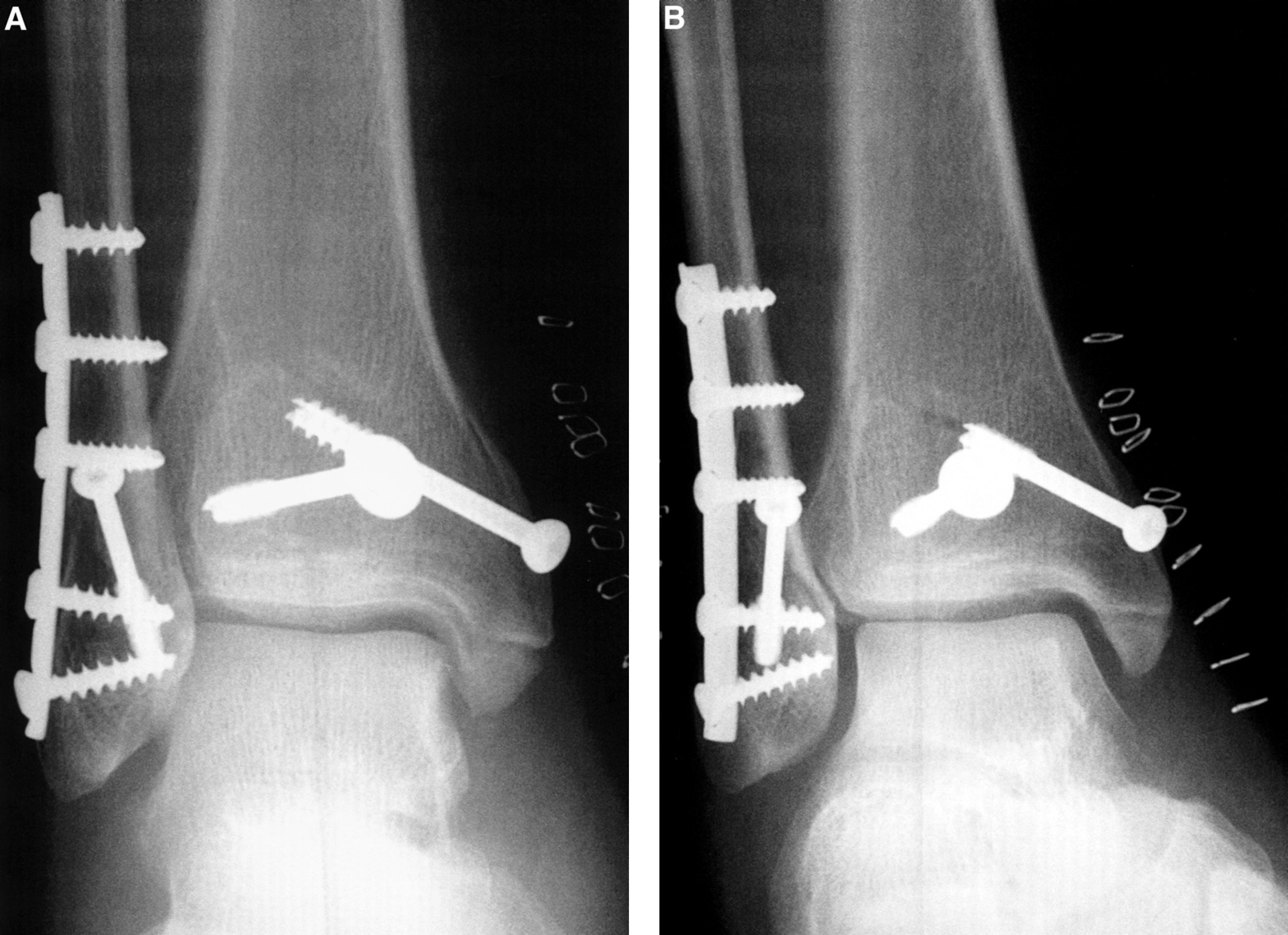
The posterior malleolar fragment can then be reduced and internally fixed under direct vision. A cannulated screw and a washer can provide adequate and proper fixation (Fig. 4).
The medial malleolar fragment can then be retracted distally and inferiorly with the assistance of a small bone hook, and the distal tibial articular surface can be examined for both congruity of the posterior malleolar fragment, and possible chondral injury. The medial malleolar fracture can then also be internally fixed through the same incision.