
Abstract
Background: Simultaneous anterior and posterior ankle impingement has not been previously reported. We identified 62 patients with both anterior and posterior impingement and report the results of anterior arthroscopic and posterior open treatment. Methods: Between January, 1990, and December, 2003, 62 consecutive patients with symptoms and signs of both anterior and posterior impingement of the ankle were identified. Fifty-eight recorded a single injury or multiple ankle sprains. The most common mechanism of injury was inversion or plantarflexion. Initial conservative treatment failed in all patients and anterior arthroscopy and open posterior clearance were done. Followup averaged 11.4 months (up to 5 years). All patients showed posttraumatic synovitis at arthroscopy, and 48 had other arthroscopically-detected lesions, such as anterior tibial plafond lesions, ossicles, or soft-tissue impingement. The posterior arthrotomy revealed a bony cause for impingement in all but four patients, usually an os trigonum or a long posterior process of the talus. Results: Three patients had anterolateral tenderness after arthroscopy and three had tenderness of the posterior arthrotomy scar. There were no persistent neurologic complications. Fifty-eight patients were available for followup. Forty-seven (81%) had excellent or good outcomes, nine (15.5%) had fair outcomes, and two (3.5%) were graded as poor. Conclusion: Usually, anterior and posterior impingement occur separately; however, there are patients who have symptoms and signs of both anterior and posterior ankle impingement. A single inversion or plantarflexion mechanism of injury may be responsible for this syndrome, although it may also be caused by repetitive inversion injury. Combined anterior arthroscopic and posterior open treatment obtained good results with minimal complications and morbidity.
Introduction
Ankle injuries are common, occurring particularly during sporting activities. Various studies have shown rates of ankle injuries occurring during sports of up to 30%. 4 Residual symptoms occur in up to 50% of people, with 15% finding sporting activities compromised by these symptoms. 10 Ankle impingement is a major cause of chronic pain.
Anterior and posterior impingement are well documented in the literature, but are generally considered as separate entities with different causal injury patterns. 3,5,10,12 -15,17 -20,23,25,26,28 We identified a group of patients who developed symptoms and signs of both anterior and posterior impingement simultaneously, usually after a single injury. If the combination of symptoms is not found at the time of initial assessment, the patient will not be treated appropriately and may continue to have ankle pain.
Anterior and posterior impingement can be treated arthroscopically or by open debridement and clearance, with good results. 3,6,10,12,14 -17,19,20 -23,25,26,28 Although arthroscopy of both the anterior and posterior aspects of the ankle is well established, posterior portals are associated with a complication rate of up to 9%. 9,11 Our patients were treated with a combination of anterior arthroscopic debridement and mini-open posterior clearance. This paper describes the diagnosis, proposed mechanism of injury, and treatment.
Materials and Methods
Between January, 1990, and December, 2003, 714 consecutive ankle arthroscopies were done at this unit for a variety of conditions. The senior author evaluated all patients. Sixty-two consecutive patients had symptoms and signs of both anterior and posterior ankle impingement after injury. The patients were identified on the basis of clinical examination alone, supplemented in all cases by plain radiographs (Fig. 1), with further imaging in 38 patients (isotope bone scans in 21, computed tomography (CT) in 24, including three CT arthrograms, and magnetic resonance imaging (MRI) in 11). A diagnosis of combined anterior and posterior impingement was made if patients were found to have pain on forced dorsiflexion of the everted foot, with or without tenderness in the notch of Harty or syndesmosis, and posterior pain on forced ankle plantarflexion, with or without posteromedial or posterolateral tenderness. Preoperative symptoms included pain, stiffness, and reduced range of movement that compromised sports or work. All had a minimum of 2 months conservative treatment in the form of rest, ice, compression, anti-inflammatory medication, and physiotherapy. Five had prior corticosteroid injection. If conservative treatment failed, patients were offered surgery.
Patients were excluded from the study if they had a history of inflammatory arthropathy, bilateral symptoms without separate identified injuries, or an alternative diagnosed cause of anterior or posterior ankle pain, such as Achilles tendinitis, posterior tibial tendon dysfunction, established arthritis, isolated flexor hallucis longus tenosynovitis, or sinus tarsi syndrome.
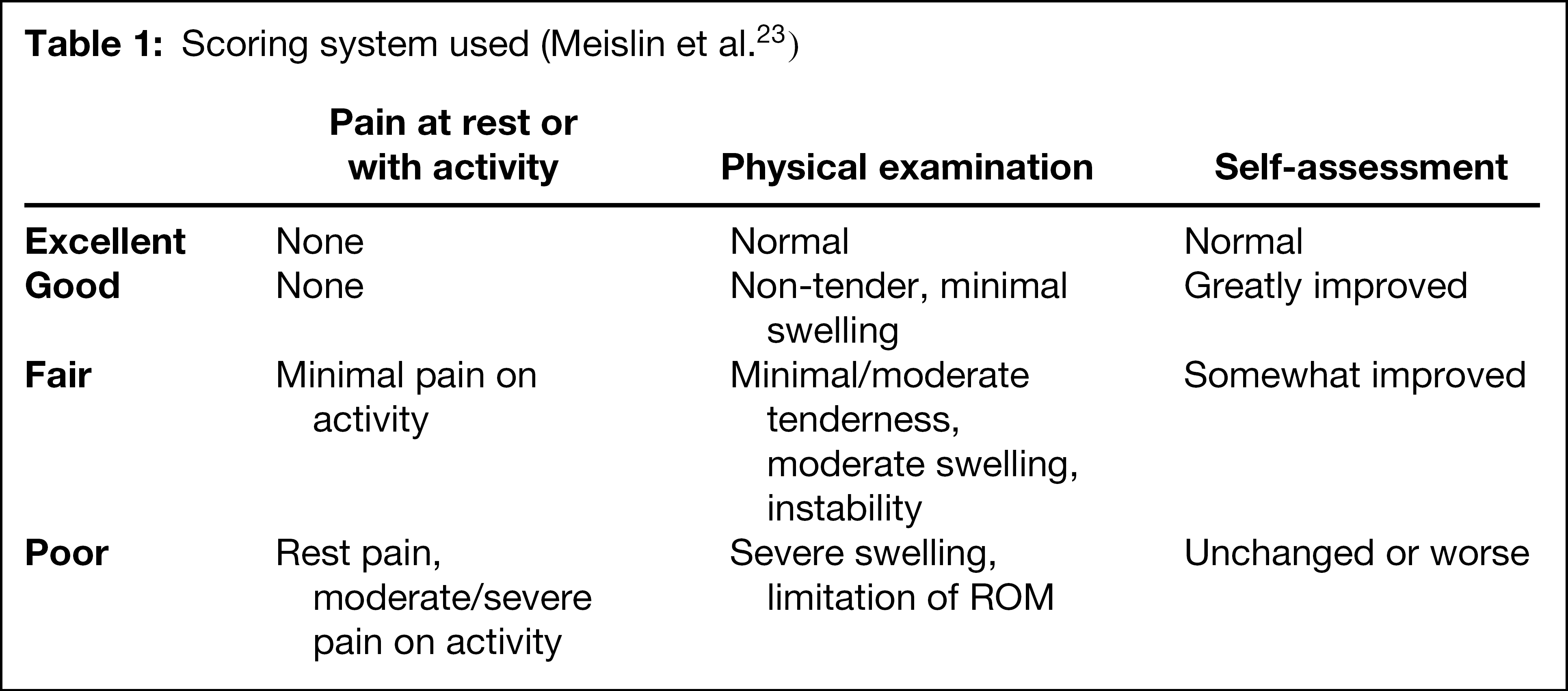
All patients were followed until discharge with resolution or plateauing of symptoms. They were graded according to the system described by Meislin et al., 23 which is broadly similar to other outcome systems (Table 1). 14,16,19,25 Any ongoing symptoms or complications arising out of the surgery were recorded.

Plain radiograph showing bony causes of both anterior and posterior impingement.
Surgical Technique
The patients were given general or regional anesthesia. A tourniquet was applied to the thigh and inflated after exsanguination of the limb unless peripheral circulation was considered potentially compromised. The calf was placed in a Lloyd-Davies leg support, positioned such that the dorsum of the foot was horizontal and abducted from the table to allow circumferential access to the foot and ankle. Two standard anterior portals were used. The ankle joint was pre-inflated with normal saline via the anteromedial portal site immediately medial to the anterior tibial tendon at the joint line. The anterolateral portal was made with the aid of transillumination to avoid damage to the superficial peroneal nerve. No traction or distraction of the joint was used. 19,23 After arthroscopy, the leg support was removed from beneath the drapes while keeping the surgical field sterile, and the leg was placed in the “figure-4” position. A small posteromedial approach was used through the bed of the flexor hallucis longus (FHL), as described by Bassett et al., 2,25 protecting the neurovascular bundle that was retracted posteriorly together with the FHL. The posterior compartment of the ankle was examined and cleared of bony and soft tissue impinging structures. The wound was closed in layers, and a plaster back-slab was applied and left in place for 12 days until the sutures were removed. Progressive weightbearing and active range-of-motion exercises were started at this point.
Scoring system used (Meislin et al. 23 )
Results
Sixty-two patients (51 men and 11 women), with an average age of 30.5 years (range 15 to 65; median 40 years) were identified for the study. Thirty-seven right ankles and 25 left ankles were affected. None of our patients had bilateral combined impingement. Fifty-eight patients recalled a prior ankle injury: 26 inversion, five hyperplantarflexion, 10 combined inversion and plantarflexion, two deceleration, and 10 repetitive or multiple injuries. One patient was involved in a motor vehicle accident and four were not certain of the mechanism of injury. Of those who recalled an injury, 39 stated that their injury had occurred during sports or recreational activities. These included Australian rules football (13), soccer (4), tennis (4), basketball (3), athletics (3), and cricket (2). Others included acrobatics, bush-walking, and rock climbing.
Twenty-one patients had isotope bone scans before surgery. In four patients the scan was normal or non-contributory. In the remaining 17 patients there was abnormal increased uptake posteromedially at the site of the posterior impingement pathology, and in seven there was increased uptake anterolaterally in the ankle (Fig. 2). Twenty-four patients had CT scans. Ossicles or bony fragments were seen in eight patients and an os trigonum or long posterior process of the talus was seen in 11 (Fig. 3). CT scans showed transchondral fracture or cyst of the talar dome in six patients. However, only one of these corresponded with visible chondral pathology at arthroscopy. Three scans were normal. Eleven patients had MRI (Fig. 4) that showed injury or disruption to the anterior talofibular ligament (ATFL) in six, with two of these also having a calcaneofibular ligament (CFL) abnormality. The MRI picked up one deltoid ligament disruption, one posterior tibial tendon signal change, one FHL tendinitis, and one altered signal in peroneus longus. In four patients the scan was non-contributory.
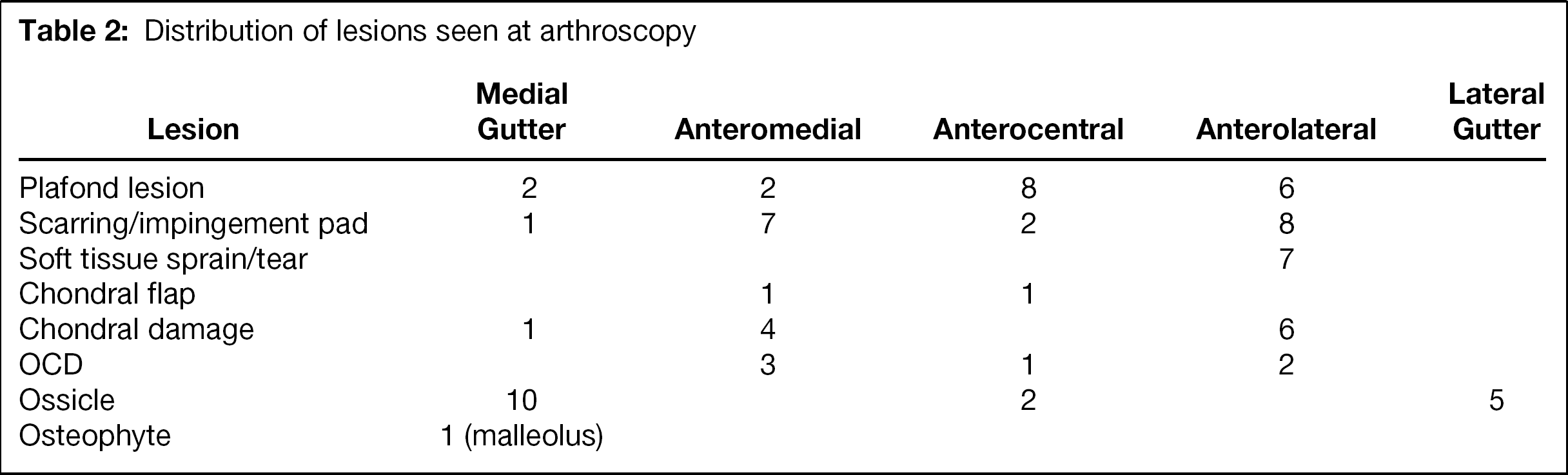
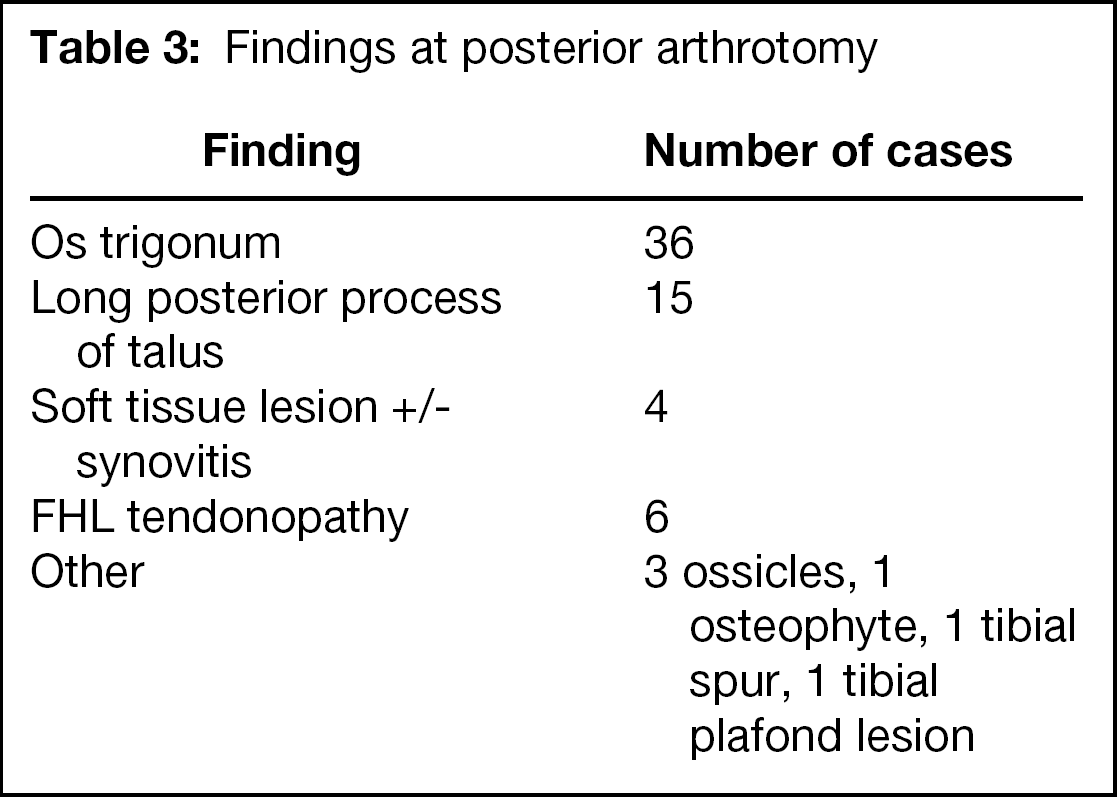
All patients had anterior synovitis seen at arthroscopy, which usually was generalized, except in three patients in whom it was localized to the anterolateral or anteromedial region of the joint. In 14 patients synovitis was the only finding at arthroscopy. In the remaining 48 patients arthroscopy revealed a range of lesions, both soft tissue and bony (Table 2). The findings at posterior arthrotomy showed predominantly bony causes of impingement except in four patients who had soft-tissue impingement or synovitis. Six patients had concomitant FHL tenosynovitis discovered at surgery (Table 3).
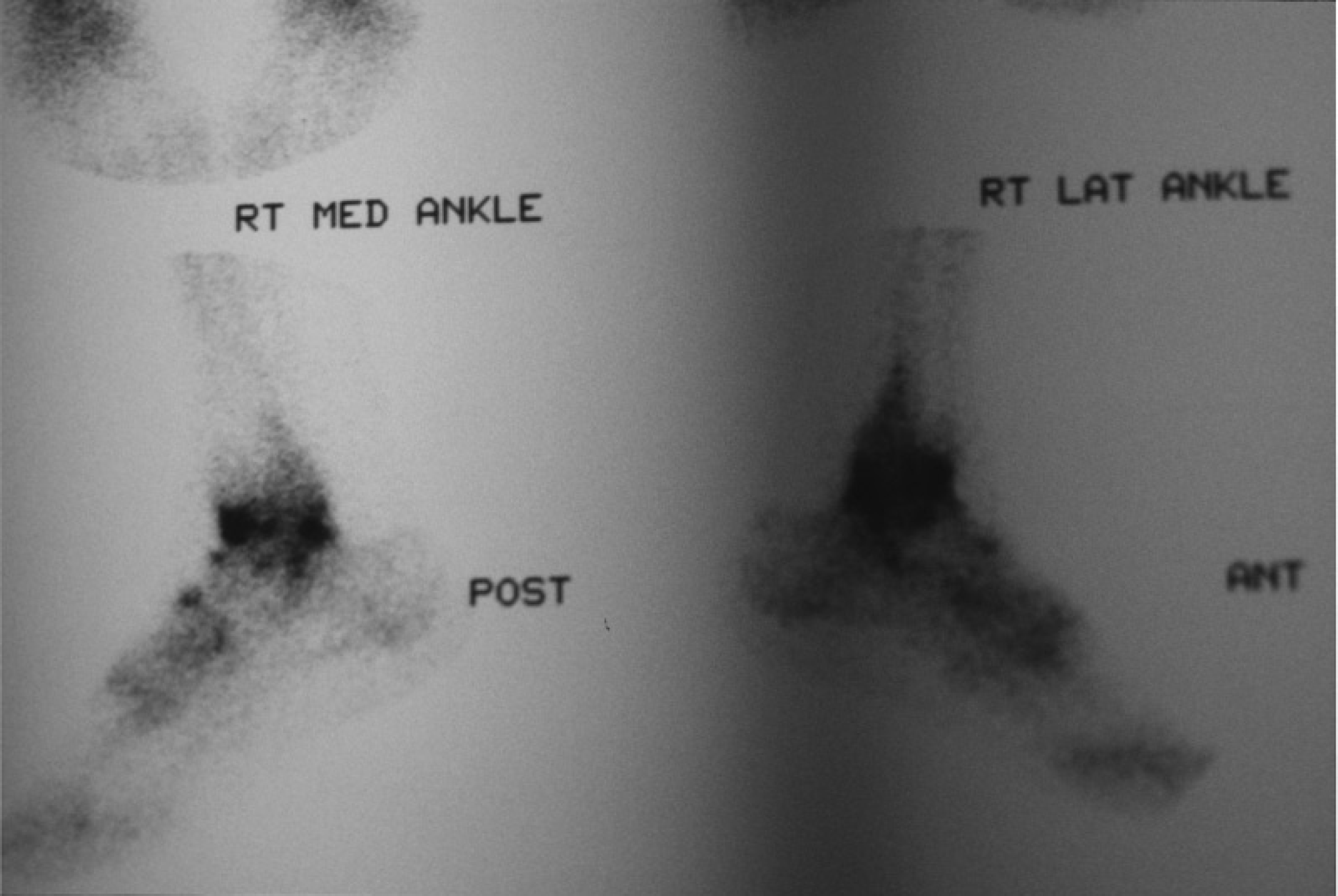
Isotope bone scan showing increased uptake anteriorly and posteriorly.
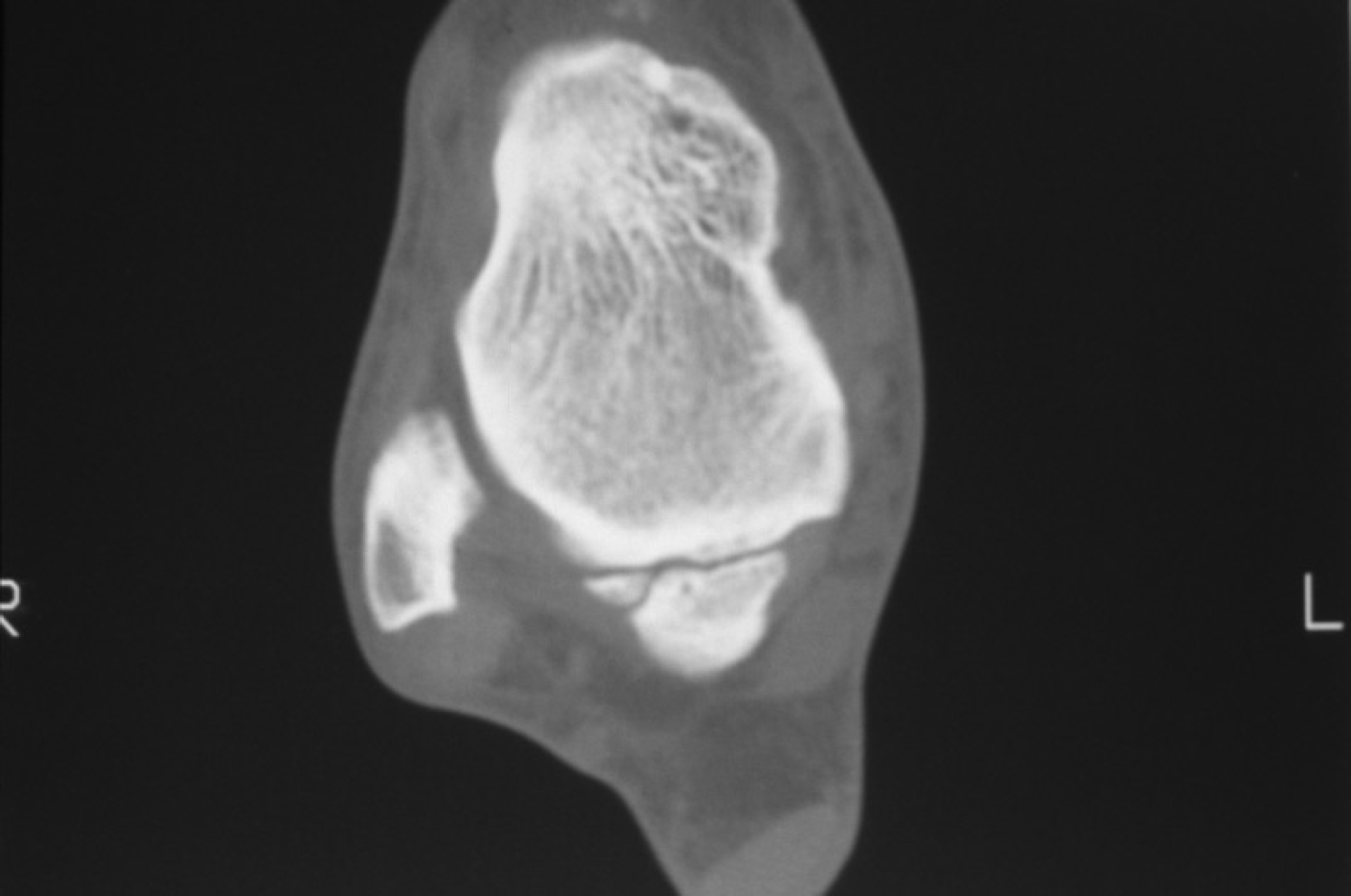
CT scan showing an os trigonum.

MRI showing posterior impingement from an os trigonum.
Distribution of lesions seen at arthroscopy
The followup was 11.4 months on average (range 2 to 69 months). One patient lived in another state and was followed by his family doctor and three patients declined review. In the remaining 58 available for review, the outcomes were excellent or good in 47 (81%), fair in nine (15.5%) and poor in two (3.5%). Patients with excellent and good outcomes were able to return to previous levels of sporting activity and work.
One patient required a repeat arthroscopy at 3 years and one patient at 2 years after initial surgery. The first patient had sustained another ankle injury, and repeat arthroscopy showed an anterolateral tibial spur and recurrent soft-tissue impingement posteriorly. The second patient had no further injury and did not have recurrent posterior impingement but had anterior symptoms. Arthroscopy showed lateral malleolar ossicles. Both patients were graded as “excellent” after the second procedure. One patient had previously had a posterior clearance alone then after a new injury developed both anterior and posterior impingement symptoms. After combined clearance, this patient had a good result. Two patients had only mild symptoms of posterior impingement on initial assessment and did not have posterior clearance, as it was thought that their arthroscopic lesions were the cause of the symptoms (one osteochondral defect (OCD) of the medial talar dome, one articular disruption of the medial malleolus). However, both subsequently went on to have persistent posterior symptoms that slowly resolved over 12 months. One patient developed subtalar arthritis 4 years after a combined procedure at the age of 58 and required a subtalar arthrodesis. This was not related to the pathology seen at the original combined procedure, posterior synovitis and a bony ossicle. The final result after arthroscopy and open clearance was graded as “good,” with mild discomfort on walking not limiting work. One patient had previously had arthrotomy to remove a traumatic OCD and had persistent posterior pain. He returned with clinical features of both anterior and posterior impingement. At arthroscopy he was found to have generalized synovitis, and the OCD had filled in with fibrocartilage and did not receive treatment at arthroscopy. An os trigonum was excised through a posterior arthrotomy. After arthroscopy and posterior clearance, he improved and was graded as “good” on final followup.
Findings at posterior arthrotomy
Postoperatively, three patients had anterolateral tenderness associated with the arthroscopy portal, but there were no neurologic injuries in this series. Three patients had posteromedial tenderness over the arthrotomy scar. One patient had slight wound dehiscence and one had mild overgranulation of the arthrotomy scar, both of which settled in time. There were no wound infections in this study.
Discussion
There have been many reports of anterior impingement and posterior impingement in the literature, but generally these are described as occurring separately. 3,5,10,12 -15,17 -20,23,25,26,28 Hamilton 13 described anterior impingement occurring after posterior impingement in dancers with concomitant rotatory instability, but to our knowledge there are no other reports describing both occurring at the same time.
Arthroscopic treatment of anterior impingement is well established, 1,6,7,9,11,16,19,21 -23,26 with published good and excellent results reported in over 80% of patients. 7,19,22,23 Treatment of posterior impingement by arthroscopic and open techniques also has been described. 12,14,15,18,25 However, posterior arthroscopy, although well established, 1,6,7,9,11,21 has a relatively high complication rate (up to 9% in recently published literature 11 ) that is thought to be associated with the placement of the posterior and anterocentral portals. 9,11 The posterolateral portal is associated with damage to the sural nerve and short saphenous vein, and the posterocentral portal has potential morbidity from disruption of the Achilles tendon. The posteromedial portal poses the highest risk of damage to local structures, with the posterior tibial vessels and nerve, branches of the calcaneal nerve and the tendons of FHL and flexor digitorum longus (FDL) all potentially at risk. Arthroscopic removal of the os trigonum, which is a relatively large fragment with strong soft-tissue attachments, is demanding and often requires enlargement of the portal, further risking the neurovascular structures. We, therefore, favor a mini-open approach. In our series no significant neurovascular complications occurred. Using an open technique offered the advantage of direct exposure of the FHL tendon, which can be released if it is inflamed, as we found in six (almost 10%) of our patients. In addition, posteromedial impingement lesions 25 can be treated through the posterior arthrotomy. The scar left after this procedure is small (4 cm to 6 cm), and in this series none of the patients had scar hypersensitivity. We believe that this is a safe approach that gives an acceptable cosmetic result with minimal complications.
Both anterior and posterior ankle pain can have several differential diagnoses other than impingement that should be excluded. Anteriorly, there may be fractures of the talus, os calcis, or base of the fifth metatarsal; peroneal tendon dysfunction or subluxation; ankle ligament instability; 27 sinus tarsi syndrome; degenerative changes; loose bodies; or reflex sympathetic dystrophy. Posteriorly, there can be fractures of the talus and os calcis, posterior tibial tendon dysfunction, Achilles tendonopathy, a posteromedial impingement (PoMI) lesion, 25 and FHL tendinitis. Flexor hallucis longus tendinitis was found in six (9.7%) patients; however, there was an intraarticular cause for impingement in each. This can be a cause of posterior ankle pain in isolation and is one of the differential diagnoses, although clinical examination can usually distinguish it from impingement. Hamilton 12,13 stated that FHL tendinitis may occur with or without posterior impingement after an ankle sprain in dancers and may be possible with other sports as well. The FHL tendon is not seen during posterior arthroscopy so this pathology may be missed, which is a further indication for a mini-open posterior approach to the ankle.
In this series two patients were thought to have predominantly anterior impingement and did not have posterior exploration and clearance. Both continued to have posterior symptoms after arthroscopy, which took several months to resolve. When clinical evidence of posterior impingement is present, the posterior ankle joint should be explored and cleared if necessary. The diagnosis is made on clinical examination with simple tests for both posterior and anterior impingement. Many patients localize their pain to the anterior or posterior aspect of the ankle, because one element of the syndrome predominates. In our practice both anterior and posterior impingement are tested for routinely, as they can be missed and potentially lead to chronic ankle pain. If posterior pain is elicited on passive forced plantarflexion, the posterior aspect of the ankle is then palpated to confirm impingement. However, there may not be tenderness to palpation. An impinging os trigonum usually is felt on the posteromedial aspect of the ankle and a PoMI lesion 25 is located just posterior to the medial malleolus. Diagnostic injection was used in four patients and can be useful if the signs are poorly localized.
Seventeen patients had isotope bone scans showing localized increased activity in the posterior or posteromedial aspect of the ankle joint. This test has previously been described as useful 25 and was found valuable in this series when the clinical findings were equivocal. Posterior clearance is done if the bone scan shows posterior impingement when the clinical signs are mild. Twenty-four patients had CT scans. Most confirmed the pathology seen on plain radiographs of os trigonum or bony ossicles. In six patients CT scan showed talar dome lesions, such as a transchondral fracture or cystic degeneration, which correlated with chondral pathology in only one patient at arthroscopy. Computed tomography added little to the management of our patients and did not identify any additional patients that clinical examination with or without bone scan may have missed. In four of our patients there was no abnormality on the CT scan, but one patient had a symptomatic posterior impingement that resolved with posterior clearance. Eleven patients had MRI. These patients were late in the series and reflect the increased use of this investigation over recent years. The most frequent finding on MRI was disruption or tearing of the ATFL in six patients. It is likely that MRI will be used more often, because it is particularly useful for defining the soft-tissue components of impingement and has been shown to be more sensitive than clinical examination for soft tissue injury. 8
The scoring system used is based predominantly on subjective criteria, with a return to previous sports or work as the main objective outcome. The grading system is that described by Meislin et al. 23 and is broadly similar to other grading systems. 12,14,15,19 We chose not to include a more detailed objective score, because several authors have shown that there is poor correlation between objective outcomes and return to work or sports, subjective patient satisfaction and pain levels. 24 -26 We accept this as a limitation in this study.
There was a range of findings on arthroscopy, and both soft-tissue and bony lesions were found across from the lateral gutter to the medial side. The only consistent finding was posttraumatic synovitis. Meislin et al. 23 showed that anterior impingement can be caused by soft-tissue impingement alone, and Martin et al. 22 described a series of 16 patients with clinically proven anterior impingement and synovitis identified only with arthroscopy that improved with arthroscopic synovectomy. Although this series describes several different findings at arthroscopy, we think that they can all be explained on the basis of an inversion or plantarflexion mechanism of injury. Based on the arthroscopic findings and previously published work, 5,8,13,25 we suggest a single mechanism of injury responsible for this condition. Plantarflexion of the talus occurs during an inversion injury of the ankle. As the talus inverts and plantarflexes in the ankle mortise it rotates medially with respect to the tibia, thus the anterior tibiofibular syndesmosis is put under strain and the ATFL is sprained. If the force is sufficiently high, the ATFL and occasionally the CFL also may be torn. As the talus rotates under the tibia, the ankle joint becomes incongruous and damage occurs to the anterior tibial plafond or the talar dome. The talus plantarflexes in the ankle mortise and the posterior elements of the talus are brought up to the posterior tibial plafond, leading to an injury of the os trigonum, if it is present, or to the posterior or medial talar processes. This mechanism helps to explain the finding of anterior soft-tissue and bony injury, with a posterior bony injury, as well as injuries to the talar dome or tibial plafond that were seen in several of our patients.
Postoperative stiffness was present for between 2 and 3 months after the combined procedure even in the group that had good or excellent results. This was probably from the anterior synovectomy and the time it took to reform a synovial lining. Final assessment of outcome should not be made before this time, although most patients will have good or excellent results.
Clinicians should be aware of the possibility of simultaneous anterior and posterior impingement of the ankle and actively examine for both in patients with anterior and posterior symptoms. This combination can be treated by anterior arthroscopy and a limited posterior arthrotomy, with satisfactory outcomes and minimal morbidity.