
Abstract
Background:
Medial opening wedge distal tibial osteotomy, a relatively new technique for treatment of intermediate ankle joint arthritis, is a technically demanding procedure that requires preoperative planning to determine the size of the wedge that will restore anatomic alignment of the joint surface. The purpose of this study was to facilitate the preoperative planning process for distal tibial osteotomy by determining angular correction obtained with various wedge heights.
Methods:
Measurements of the distal tibia were taken from cadaver specimens to develop a database of average distal tibial widths. A distal tibial osteotomy was then done on the cadaver specimens with the placement of wooden block wedges of various heights at the osteotomy site. Preoperative and postoperative radiographic measurements of the joint surface angle were obtained on all specimens. The measured amount of angular change was compared to the mathematically predicted angular change using the formula ta θ = H/W.
Results:
The mathematical model accurately predicted the amount of measured angular correction of the distal tibial articular surface. There was an approximate 2-degree angular change of the articular surface per millimeter of wedge height. As the tibial width increased, a smaller amount of angular correction per millimeter of wedge height was noted, and as wedge height increased with the same tibial width, less angular correction was obtained per millimeter of wedge height.
Conclusion:
With appropriate preoperative planning, an accurate prediction can be made as to the amount of ankle joint correction that should be obtained with surgery. The size of the wedge that will provide the desired amount of correction can be accurately determined preoperatively.
INTRODUCTION
Distal tibial osteotomy is a relatively new procedure that has been used in the treatment of a varus ankle deformity caused by intermediate ankle joint arthritis. Anthropometric measurements of the angle between the tibial shaft and the tibial joint surface seen on an anteroposterior radiograph (TAS angle) and lateral radiograph (TLS angle) have been published. 1,5,7,8,11,12 The TAS and TLS angles are two standard measurements used to determine the plane of the ankle joint (Figure 1). The TAS angle demonstrates the amount of varus or valgus angulation of the ankle joint, while the TLS angle demonstrates the amount of anterior ankle joint surface opening.
Normal measurements for the TAS angle range from 88 to 93 degrees. 1,5,7,8,11,12 Ethnic differences have been noted, with the Japanese tending to have more varus than Caucasians. 1,5,7,8,11,12 Measurements of the normal TLS have been published only for Japanese subjects with an approximate 81 degree anterior opening. 1,2,5 –12
The goal of surgery is to recreate the normal angle of the ankle joint surface (Figure 2). Takakura et al. first recommended using an opening wedge osteotomy with slight over-correction of the TAS and TLS angles, 10 but in a later study they recommended that correction not exceed the normal angle. 11 Cheng et al. sought to correct the TAS and TLS angles to their normal values, and all of their patients were brought to within the normal ranges with surgery. 2,3
During preoperative planning, it is necessary to know the width of the distal tibia in the coronal and sagittal planes. This information is then used to determine the height of the wedge that must be fashioned to obtain the appropriate amount of correction of the distal tibial articular surface. 4 The purpose of this study was to provide information that will make this determination easier. The study provides a database of average tibial widths at the osteotomy site, which makes it possible to determine an average amount of angular correction per millimeter of wedge height. An algorithm for preoperative planning of an opening wedge distal tibial osteotomy is proposed using a mathematical model to predict the amount of angular correction that is obtained with surgery.
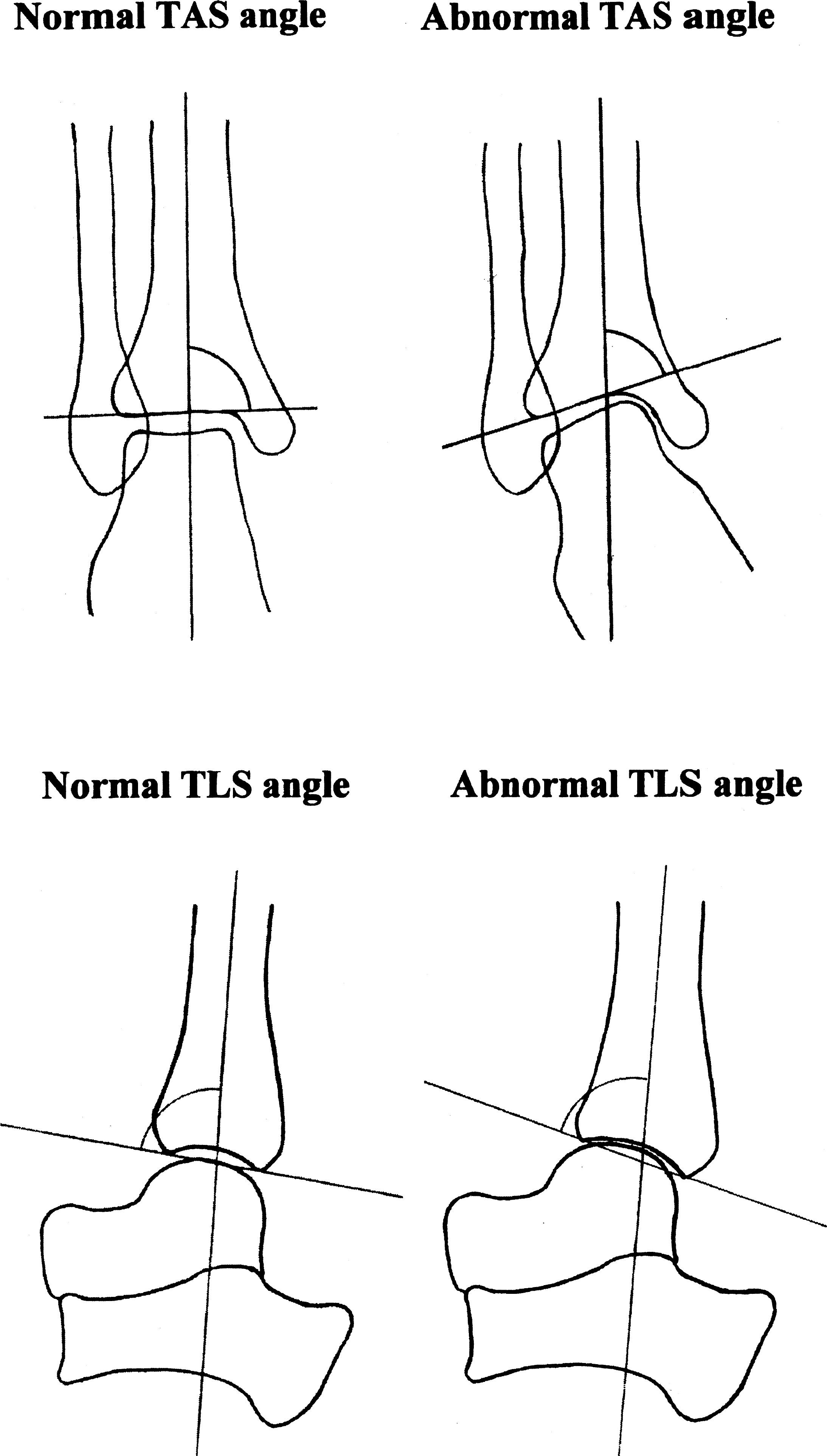
Abnormal TAS angle shows a varus ankle with medial joint space narrowing. Abnormal TLS angle shows anterior joint opening with anterior joint space narrowing.
MATERIALS AND METHODS
Part I
Measurements were taken bilaterally from the distal tibia in 39 Caucasian cadaver specimens. The widths of the distal tibias were measured in both the coronal and sagittal planes at a point 5 cm proximal to the tip of the medial malleolus (Table 1). A digital caliper accurate to +/-.01 mm was used to make the measurements. There were 21 male and 18 female cadaver specimens. A database of average tibial widths was formulated from this data. Pearson correlation coefficients were used to determine if the sagittal and coronal measurements had a linear correlation. A Student's t-test was used to determine if the measured widths (both sagittal and coronal) were different between males and females. A paired t-test was used to determine a statistically significant difference between the measurements of the right and left legs. A paired t-test also was used to determine a significant difference in ages between male and female cadaver specimens.
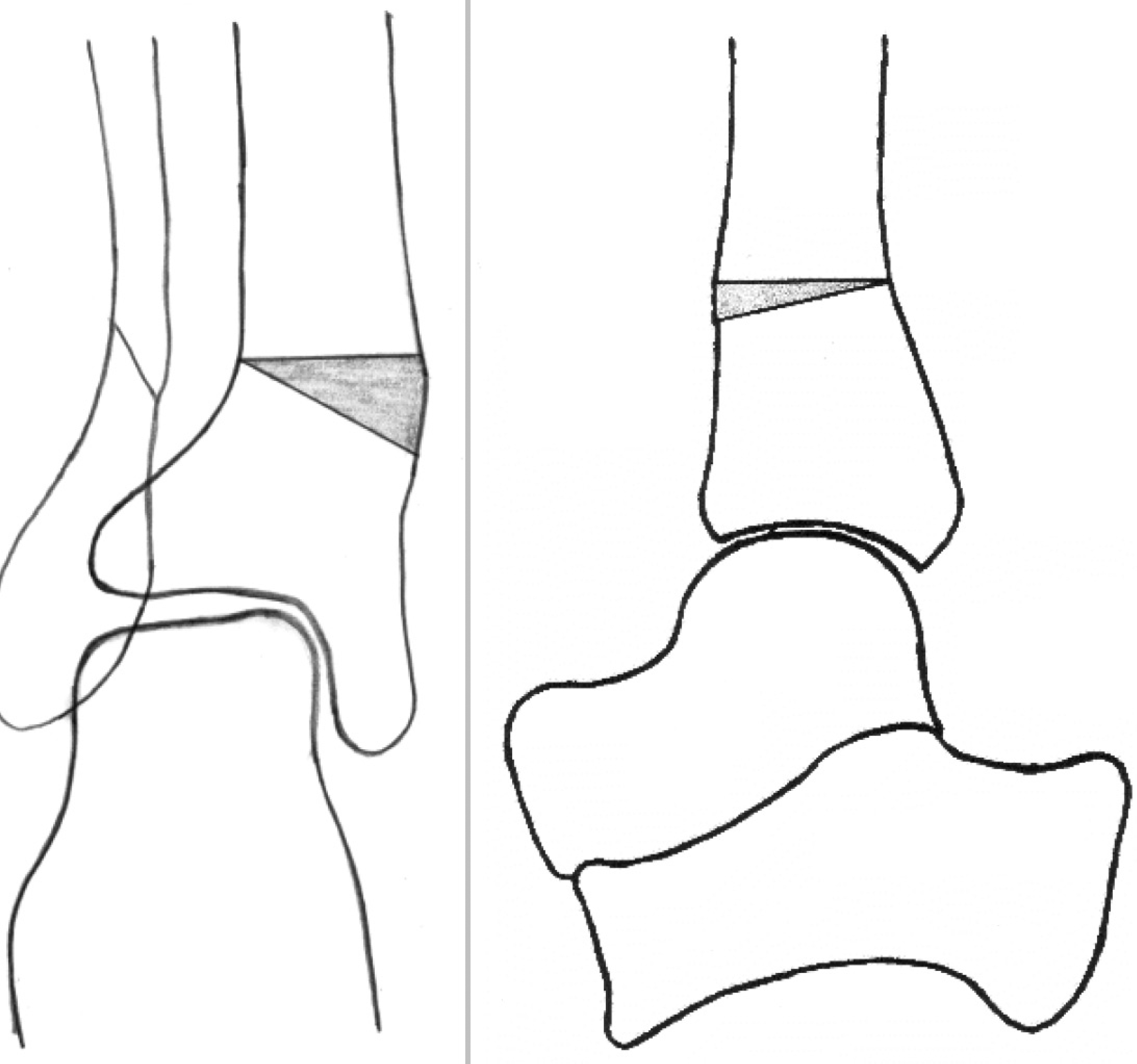
Distal tibial osteotomy.
Part II
Three separate ankles from cadaver specimens were measured to determine the width of the tibias in both the sagittal and coronal planes 5 cm proximal to the tip of the medial malleolus. Anteroposterior and lateral radiographs also were obtained of the ankle specimens. A horizontal tibial osteotomy was made 5 cm proximal to the tip of the medial malleolus. Wooden wedges were fashioned to match the width of the tibia at the osteotomy site. The width of each wedge coincided with the coronal and sagittal widths, respectively, at the osteotomy sites. The wedges were right triangles and were of various heights, ranging from 4 mm to 20 mm. The wedges were measured using a digital caliper. The amount of angular correction of the joint surface for each wooden wedge was predicted using the formula tan θ = H/W (θ: axial angle H: wedge height W: tibial width) (Figure 3). The wooden wedges were inserted into the osteotomy site, and anteroposterior and lateral radiographs were obtained of the ankle. Angular change in the joint surface was determined by measuring the angle between the tibial shaft and the tibial joint surface in the anteroposterior and lateral planes using a goniometer accurate to +/-1 degree. The calculated and predicted angular corrections were then compared to determine if the mathematical model accurately predicted the amount of angular correction obtained with the procedure. Pearson correlation coefficients were used to determine if the measured and calculated values had a statistically significant linear correlation.
Mean Widths* of Distal Tibia in Cadaver Specimens
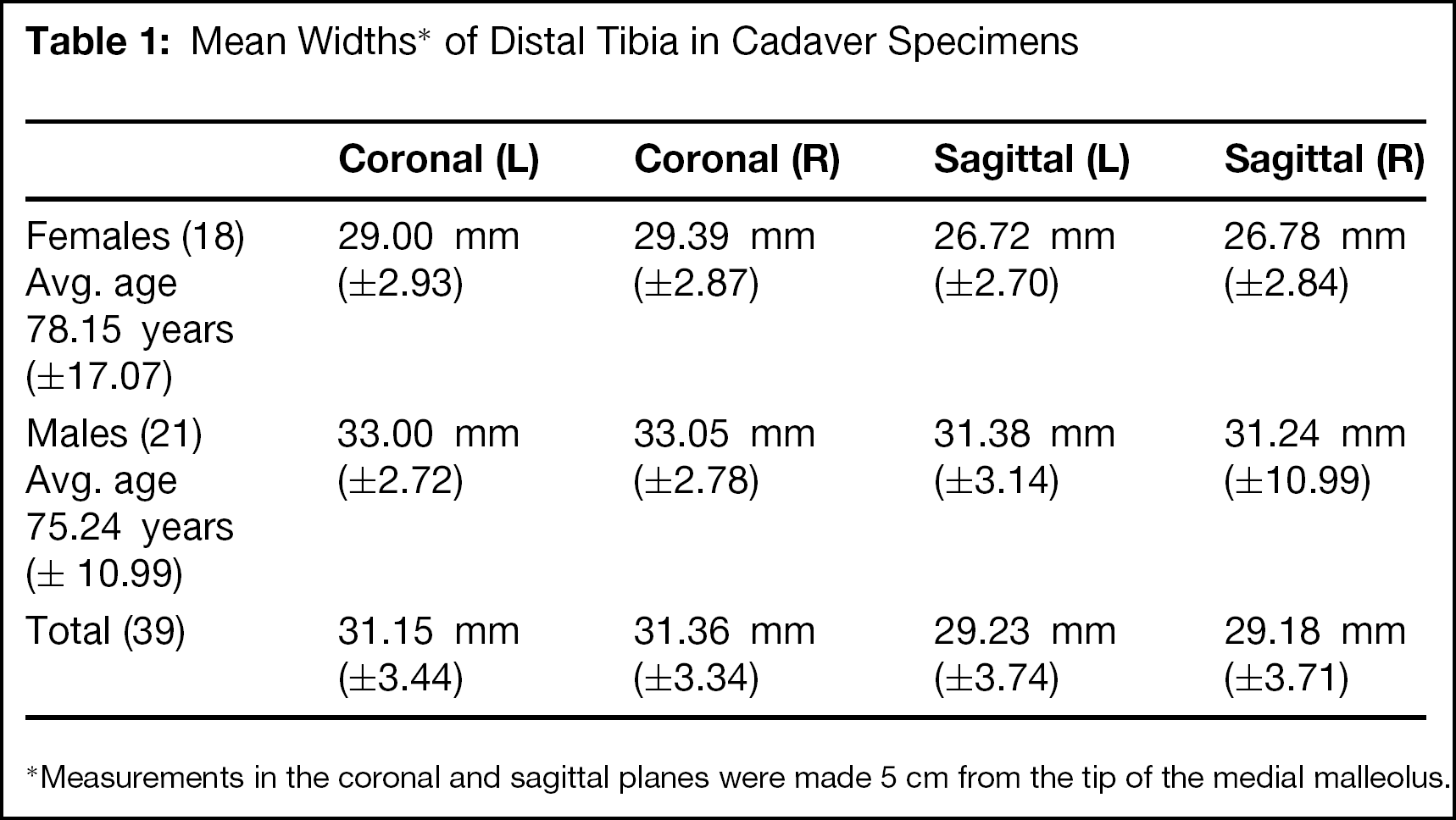
Measurements in the coronal and sagittal planes were made 5 cm from the tip of the medial malleolus.
RESULTS
The measurements of the distal tibial width in the sagittal and coronal planes provided a database of average tibial widths. The sagittal measurements had a linear correlation to the coronal measurements (R2 = .624, p = .001). A significant difference was found between the average female and male tibial widths of 4 mm (p = .001) Comparison of right and left legs in the coronal plane did not show a statistically significant difference (p < .073). There was no significant difference in ages between male and female specimens (p = .524).
The cadaver study was used to confirm the accuracy of a mathematical model in predicting the angular correction obtained with various wedge heights. Radiographic measurements were taken of the ankle after the distal tibial osteotomy in the cadaver specimens. A database was compiled of the measured and calculated angular change for various wedge heights. A comparison was made between the measured change in the TAS and TLS and the mathematically predicted change using the formula tan θ = H/W (Table 2). The measured and predicted values were plotted on a graph with a statistically significant linear correlation thus showing that the mathematical model accurately predicted the amount of measured correction of the distal tibial articular surface (R2 = .976, p = .001) (Figure 4).
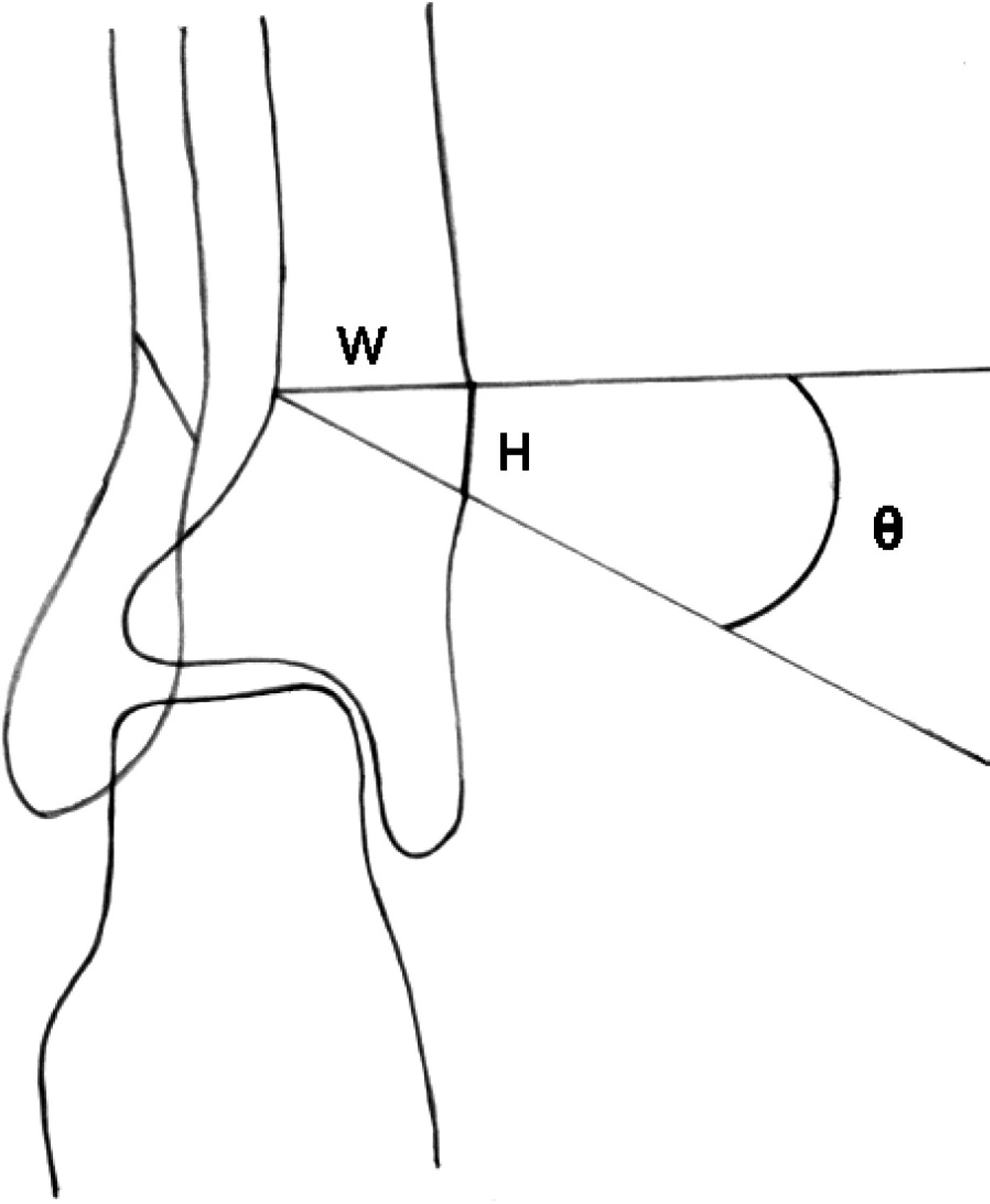
Tan θ = H/W (0: axial angle; H: wedge height; W: tibial width).
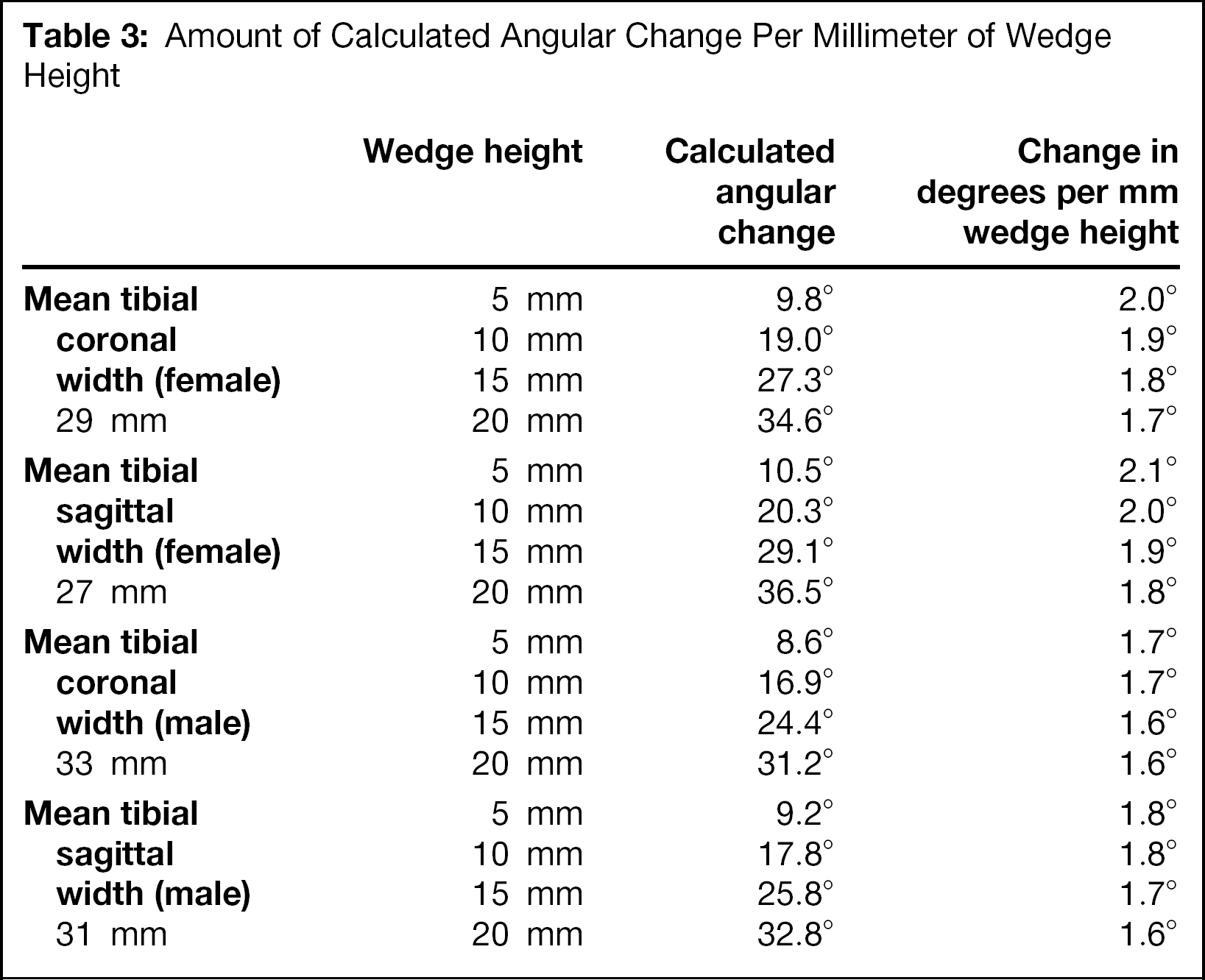
The mean coronal and sagittal widths of the tibias were used to make a database that predicts the amount of angular correction obtained per millimeter of wedge height. The angular change was calculated at each mean tibial width for the various standard wedge heights. The amount of angular correction for each wedge height was dependent on the width of the tibia. It was noted that, as the tibial width increased, there was a smaller amount of angular correction per millimeter of wedge height. Thus, wider tibias had a smaller amount of angular change per millimeter of wedge height and required higher wedges to obtain the same amount of correction. A second finding was that as the wedge height increased with the same tibial width, less angular correction was obtained per millimeter of wedge height. Therefore, as the wedge height increased the amount of angular correction per millimeter of wedge height decreased (Table 3).
Measurements of the Predicted and Angular Changes With Various Wedge Heights
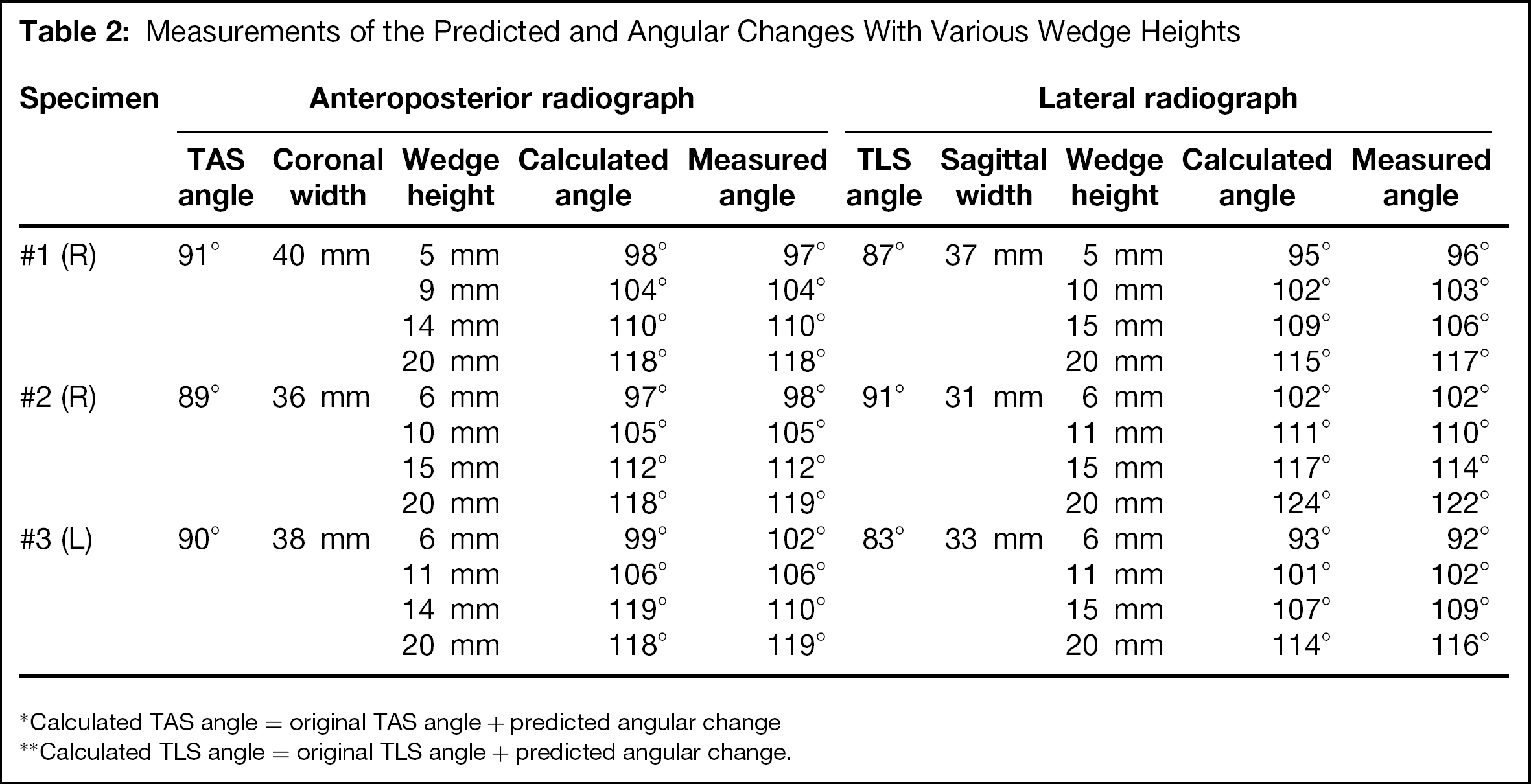
Calculated TAS angle = original TAS angle + predicted angular change
Calculated TLS angle = original TLS angle + predicted angular change.
Amount of Calculated Angular Change Per Millimeter of Wedge Height
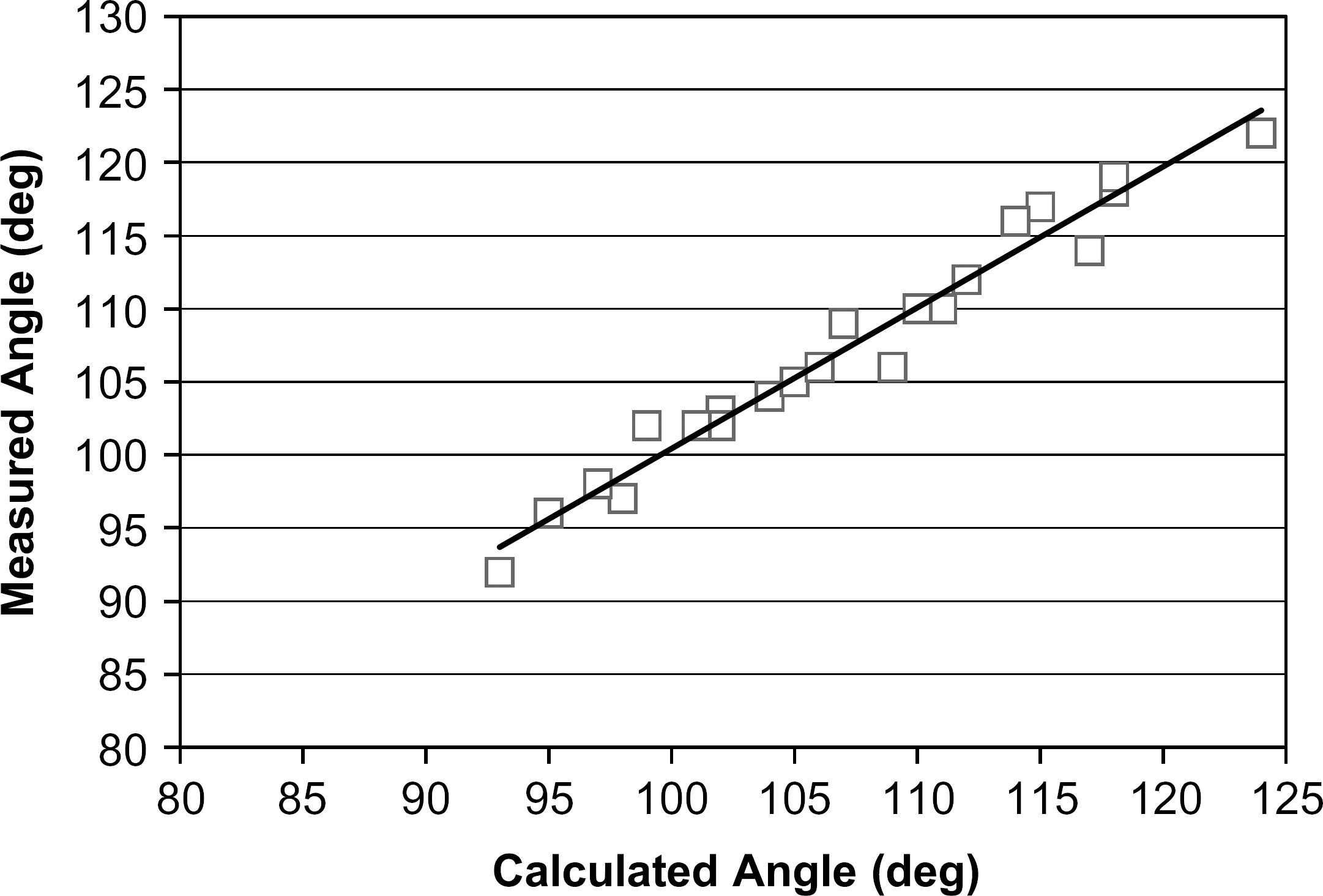
Correlation between the measured and calculated angular change.
DISCUSSION
Distal tibial osteotomy is a promising yet technically demanding treatment for moderate ankle joint arthritis. It is particularly difficult to fashion a wedge that corrects the tibia in both the sagittal and coronal planes simultaneously. The goal of treatment is to correct the varus tilt as well as the anterior opening of the distal tibial articular surface. Preoperative planning is an important part of this surgery. When done appropriately, an accurate prediction can be made as to the amount of ankle joint correction that should be obtained with surgery and the size of the wedge that will provide the desired amount of correction.