
Abstract
Background:
While use of a thigh tourniquet with general anesthesia is widely accepted, use of an ankle tourniquet in the awake patient is more controversial. In particular, it is not clear how long patients tolerate this device or what the consequences are of intraoperative tourniquet pain.
Method:
A prospective audit was done of 1000 patients undergoing midfoot and forefoot surgery using an ankle block. We examined the intraoperative problems associated with the use of an ankle tourniquet, particularly the role and consequences of intraoperative tourniquet pain. Risk factors for tourniquet pain were statistically examined, and patient acceptance was gauged through followup questions.
Results:
With correct application and the option of sedation, 3.1% of patients complained of tourniquet pain. In 0.4% of patients tourniquet pain necessitated a conversion to general anesthesia. A significant association was found between tourniquet pain and both age and tourniquet time. We found that for patients younger than 70 years of age, the tourniquet can be applied comfortably for up to 30 minutes in over 97%. For each 11 minutes beyond this, another 1% of patients reported tourniquet pain. However, patients 70 years or older had an average 3.5 times increase in tourniquet pain. In this age group the tourniquet can be applied comfortably for up to 30 min in 91%. For each 3.2 minutes beyond this, another 1% reported tourniquet pain. When questioned, 97.2% of our patients reported that they would have surgery again with an ankle tourniquet.
Conclusions:
Our audit shows that with correct application and the option of sedation the ankle tourniquet is well tolerated by most patients. However, clinicians need to be mindful that patients 70 years of age or older are at greater risk of tourniquet pain and that in all patients the risk of tourniquet pain gradually increases when application times exceed 30 min.
INTRODUCTION
A bloodless field provides increased operative visibility and potentially decreases operative time and risks of complications. The tourniquet is an effective means of obtaining a bloodless field, but its use is not without risk. A number of articles have reviewed the pathophysiologic consequences and complications attributed to the use of a tourniquet, including local damage to nerves and muscles and hematologic changes, such as the development of deep vein thrombosis. 6,11,26,28 However, these complications are regarded as uncommon or manageable through careful patient selection and appropriate use of the tourniquet. Indeed, use of a thigh tourniquet with general anesthesia is widely accepted. Use of an ankle tourniquet in an awake patient is somewhat more controversial. Of particular concern to many clinicians is the problem of tourniquet pain. However, there is little research into the limits of patient tolerance for this device, particularly when used with sedation. Thus, a prospective audit of 1000 patients having midfoot and forefoot surgeries under ankle block was undertaken to determine the degree to which an ankle tourniquet is tolerated by awake patients. Particular emphasis was placed on tourniquet pain, intraoperative difficulties associated with the use of an ankle tourniquet, and patient satisfaction.
MATERIALS AND METHODS
One thousand patients who had elective midfoot and forefoot surgeries by a single surgeon (GD) and single anesthetist (GR) were prospectively studied between July, 1997, and November, 2003. Exclusion criteria included patients with bleeding abnormalities, neurologic or neuromuscular disease, systemic infection or local infection at the proposed site of the ankle block, a history of hypersensitivity to amide local anesthetics, and patients who requested general anesthesia. The audit was conducted at two private hospitals where audit approval was granted and all patients gave informed consent to participate in the study.
Of the 1000 patients who had midfoot or forefoot surgery using an ankle block, 804 (80.4%) were women and 196 (19.5%) were men. The mean age was 57.9 years (range 13 to 98 years; SD 14.1 years). The mean weight was 72.7 kg (range 40 kg to 125 kg; SD 14.5 kg). Four hundred and seventy four patients were American Society of Anesthesiology (ASA) risk grade I, 390 were grade II, 132 were grade III, and 4 were grade IV.
Before the day of surgery, the surgeon provided the patient with written information about the surgery and ankle block with ankle tourniquet. The risks and benefits were further discussed with the patient at the preoperative anesthetic visit. Patients could elect to be awake or drowsy during surgery.
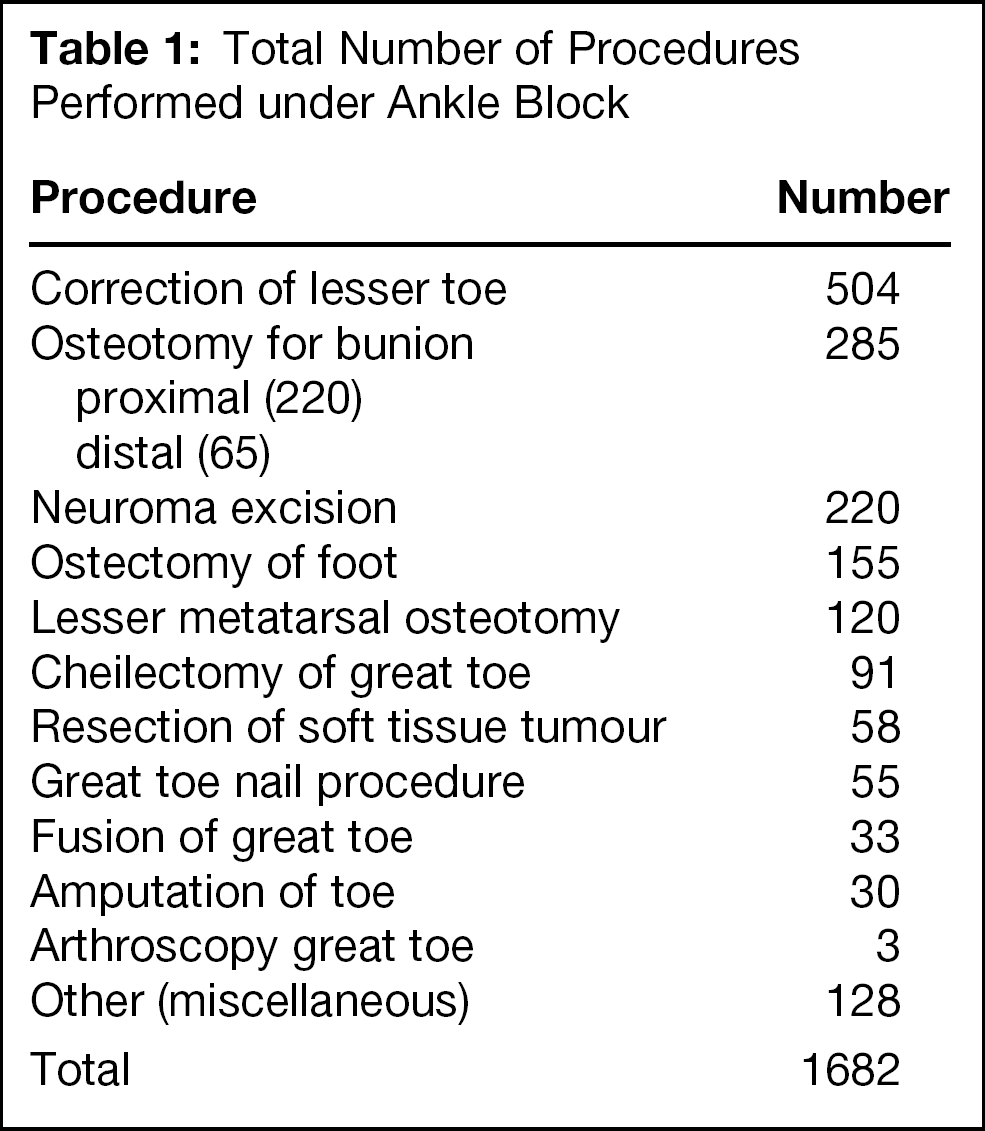
One thousand six hundred and eighty two midfoot or forefoot procedures were done (Table 1). The median operative time was 20 (range 9 to 128) minutes.
The ankle block was done in a standard manner throughout the study, as previously described by Kelly et al. 12 Preoperative intravenous sedation was administered in accordance with patient demand, with particular consideration given to the patient's request for amnesia. Intraoperative intravenous sedation (midazolam or propofol) was titrated to patient effect, and the reason for administration was recorded. Both the surgeon and the anesthetist encouraged patients who wished to be awake during surgery to watch or discuss the operative procedure.
Total Number of Procedures Performed under Ankle Block
In 12 surgical procedures, the surgeon chose not to use a tourniquet. In eight patients there was evidence of severe peripheral vascular disease, and it was not possible to palpate a pulse, and in two patients there was a history of deep vein thrombosis. In one patient mechanical tourniquet malfunction occurred. In one instance the procedure was done in less than two minutes.
Every effort was made to minimize tourniquet time. The lower leg was padded just above the malleoli with a 15-cm roll of Softban dressing. A 15-cm wide conical low-pressure ankle tourniquet was applied over the Softban (Zimmer, Warsaw, Indiana) (Figure 1). The limb was then prepared, draped, elevated, and exsanguinated, and the tourniquet was inflated to 250 mm Hg.
Data collected during the audit included the patient's sex, age, weight, American Society of Anesthesiology (ASA) risk status, blood pressure; the date, type and duration of surgery; duration of tourniquet application; intraoperative sedation details (drug and dose); details of patients converted to general anesthesia; pain specifically related to the application of the tourniquet; mechanical tourniquet problems, and intraoperative hypertensive and breakthrough bleeding episodes.
Postoperative assessment was by telephone survey on the first postoperative day. Patients were asked if they remembered their surgery, if they experienced tourniquet pain during surgery, and whether they would be happy to have a procedure done under an ankle block with an ankle tourniquet again. Independent of the telephone survey, surgical assessment was done two and six weeks postoperatively, at which time neurologic symptoms relating to surgery or anesthesia were recorded.

Placement of the Ankle Tourniquet.
Data analysis consisted largely of calculation of descriptive statistics, tabulation, and graphical examination of the data, and was carried out using R. 23 Logistic regression was used for the initial assessment of the effects of age, tourniquet application time, weight, and gender on tourniquet pain. Subsequent investigation of these effects used linear regression on grouped data. Comparison of means used the Welsh two-sample t-test at the 5% significance level.
RESULTS
Thirty-one of 988 (3.1%) patients complained at the time of surgery of intraoperative pain from the tourniquet. In eight patients tourniquet pain resulted in an interruption in surgery. The reasons are outlined as follows: in one patient tourniquet pressure was reduced to 200 mm Hg to limit pain but resulted in breakthrough bleeding; two patients moved their limbs excessively from tourniquet pain; and in one patient, the anesthetist, in an attempt to compensate for tourniquet pain, over-sedated the patient; four patients were converted from an ankle block to general anesthesia because of tourniquet pain.
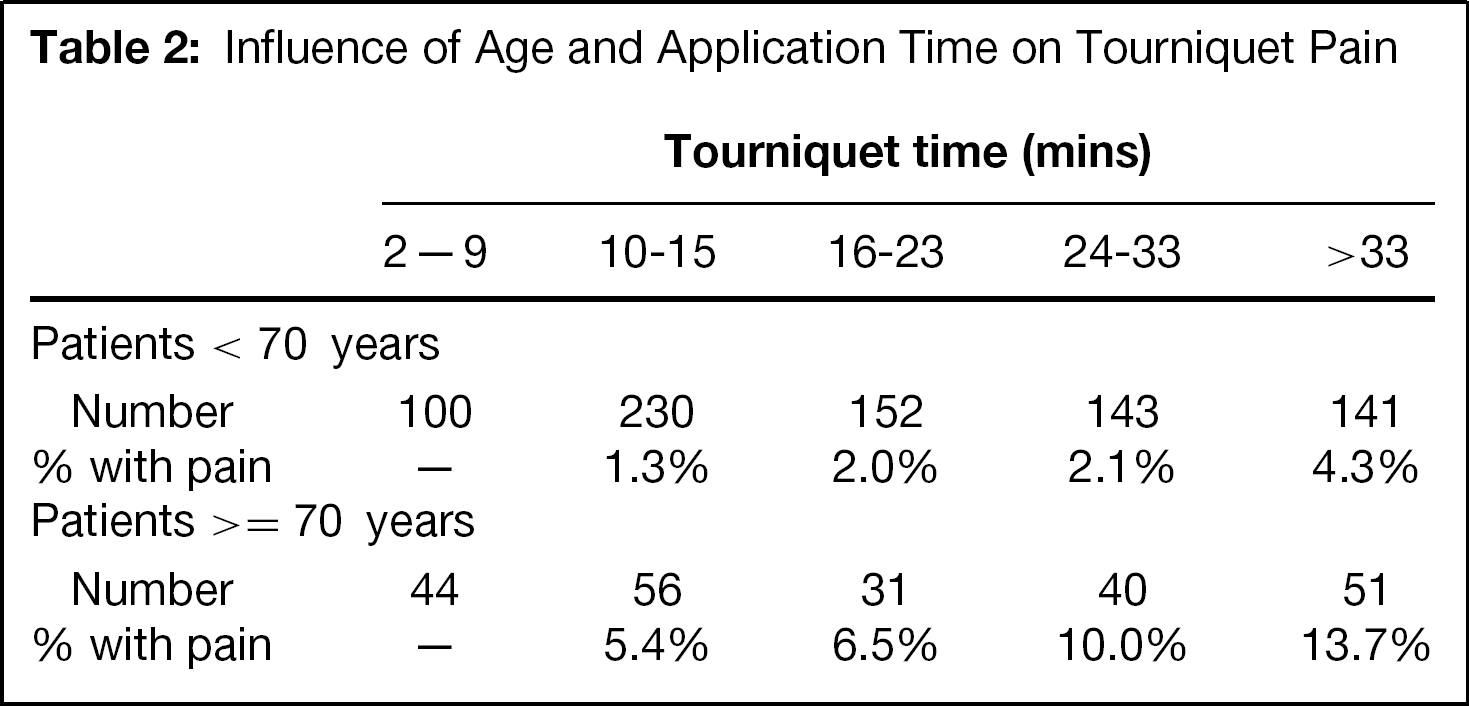
Tourniquet times ranged from 2 to 90 min, with the median time being 18 min, mean time 22.4 min and standard deviation 14.7 min. Logistic regression analysis confirmed significant effects of age (p < .01) and tourniquet application time (p < .001) on tourniquet pain. This model assessed the probability of tourniquet pain with increasing levels of age and tourniquet time, without assuming any particular groupings of age or tourniquet time. Subsequent investigation showed that the age effect was largely a contrast between those younger than 70 years and those older than 70 years, and thus the two groups were treated separately. Grouped data is shown below in Figure 2.
Tourniquet application times of less than 10 minutes produced no reports of pain for either group. For both age groups, the rate of reported intraoperative tourniquet pain increased approximately linearly with tourniquet time. Regressing (through the origin) the percentage of patients with pain within a tourniquet time class interval showed highly significant regressions for each age class. The slopes of the regressions were significantly different (all p < .001). The slope of the fitted regression was 3.5 times greater for patients 70 years and older than for those 70 years or younger. Thus, on average, there were 3.5 times more patients over 70 years of age reporting pain after any particular tourniquet time than there were patients younger than 70 years. Tourniquet pain was unrelated to gender, weight, or intraoperative sedation dosage (Table 2).
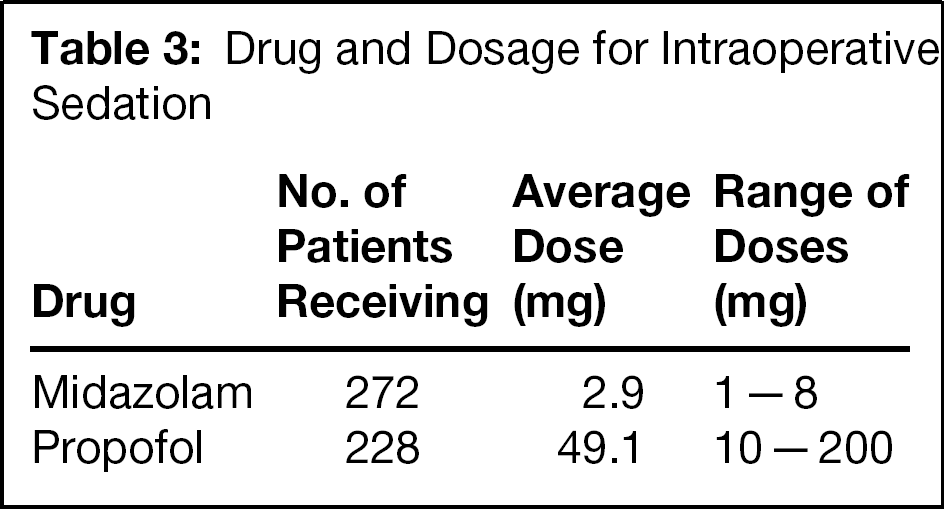
Nine patients were converted to general anesthesia. Intraoperative sedation was administered to 50.5% of patients who were not converted to general anesthesia (500 of 991 patients) (Table 3). The reasons, often multiple, for administering intraoperative sedation are presented in Figure 3.
Of the 31 patients who experienced tourniquet pain, four resulted in conversion to general anesthesia. In three no sedation was required. In 23 instances tourniquet pain was satisfactorily dealt with by intravenous sedation. In one instance the patient was oversedated. Average dosage given to patients experiencing pain did not differ significantly from the dosage of the same drug given to those with no pain.
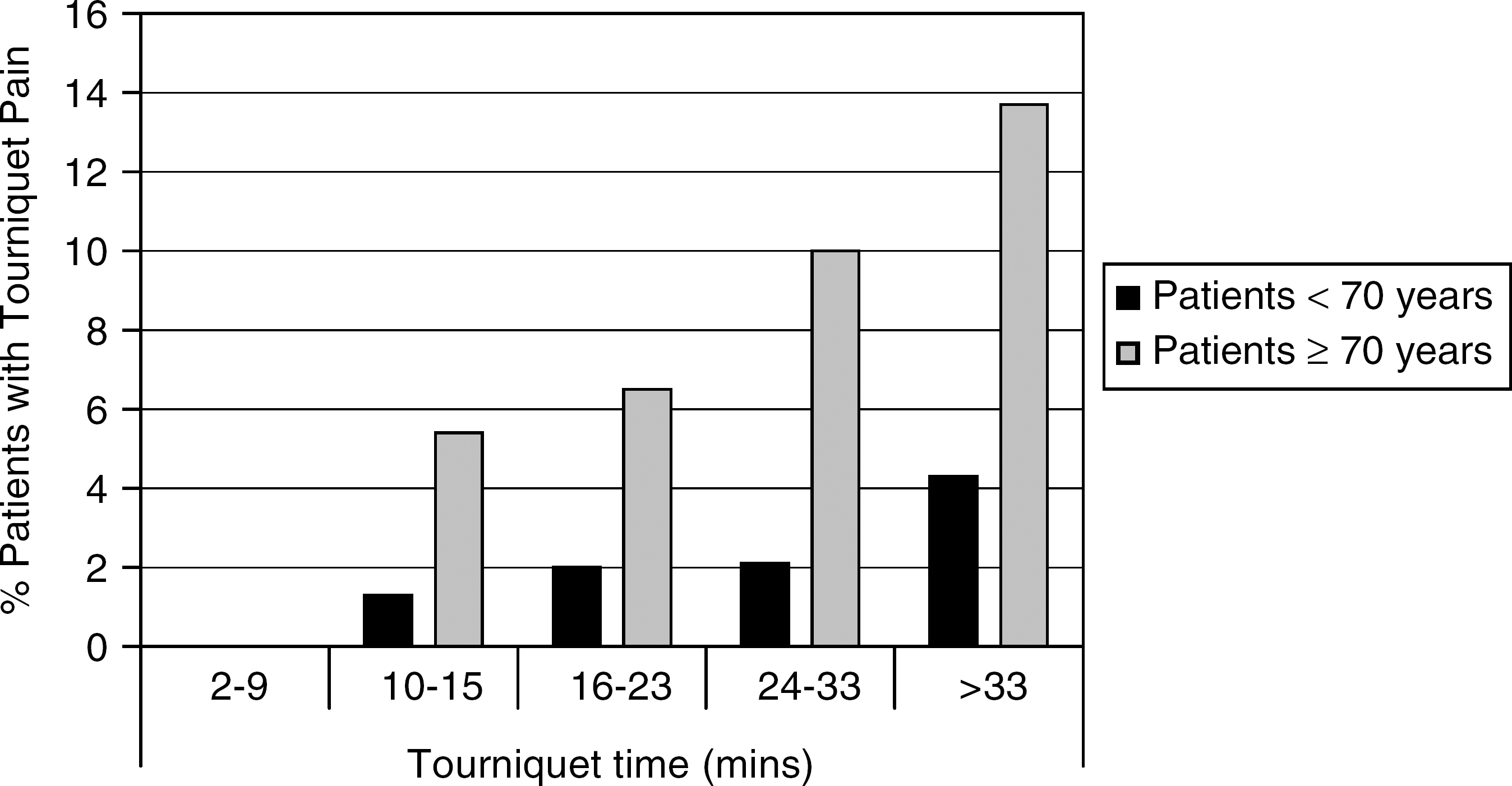
Effect of tourniquet time and age on tourniquet pain (grouped data).
Intraoperative hypertension occurred in 27 of 988 patients (2.7%). In 20 of these the patients had preoperative hypertension. In four patients, high blood pressure resulted in breakthrough bleeding. Tourniquet pressure was raised to control bleeding in three of these patients, while in the fourth bleeding was minimal and tolerated by the surgeon. In the other patients the anesthetist managed elevated intraoperative blood pressure with sedation. This strategy was successful in all but one patient in whom the anesthetist reduced blood pressure and calmed the anxious patient by increasing the dose of sedative agent, but in the process oversedated the patient.
Mechanical problems with the tourniquet were encountered three times during the study, twice due to connector problems, once due to a faulty inflator seal. In one instance mechanical problems resulted in the procedure being done without a tourniquet.
Of 899 (89.9%) patients who were followed, 611 (68.0%) remembered surgery, and of these patients, only 17 (2.8%) complained at the postoperative interview of feeling tourniquet pain during surgery. Only two of the patients who remembered the surgery complained of tourniquet pain at the time of surgery. Thus, 15 complained of tourniquet pain upon reflection. However, all patients who complained of tourniquet pain postoperatively reported that they would have surgery using an ankle block with ankle tourniquet again. There was one report of paresthesia at 6 weeks followup, but despite attempts no further contact could be made with this patient.
Influence of Age and Application Time on Tourniquet Pain
Drug and Dosage for Intraoperative Sedation
DISCUSSION
The techniques used by orthopaedic surgeons in midfoot and forefoot surgeries vary greatly. In a survey of foot and ankle surgeons across Canada and the United States, most respondents used a tourniquet for foot and ankle surgery (96.6%). 10 However practices varied substantially among surgeons, and although most (92%) used ankle tourniquets, only 27% used ankle tourniquets exclusively. 10 The first major study of regional anesthesia for foot and ankle surgery led by Mark Myerson (1992) was done without routine use of a tourniquet. 20 The advantage of Myersons's technique was that he usually could operate without the presence of an anaesthetist, without risk of complications associated with the tourniquet, and arguably with a lower rate of wound infection. 3 The potential disadvantage of this technique is that the surgeon may be working in a comparatively bloody field with reduced operative visibility and possible increased operative times. Myerson's technique, while not popular, certainly is not without merit. Nevertheless, the prospect of shorter operative times is attractive to many surgeons and patients, and in this audit the surgeon elected to use an ankle tourniquet whenever possible.
There is no rule as to how long a tourniquet may safely be inflated, and it depends greatly upon the patient. Clinically, the outer limit of uninterrupted tourniquet use under general anesthesia usually is placed at 2 hours. 5,29 In an awake patient the threshold is lower and depends on the patient. For instance, Fuselier et al. 8 established that an awake patient could tolerate a thigh tourniquet for an average of 32 minutes without sedation and 45 minutes with sedation. Finsen and Kasseth 7 showed that an ankle tourniquet is better tolerated than a calf tourniquet, but did not offer a guide for its use.
Some conclusions may be drawn from this audit; however, the notion of an empirical threshold for ankle tourniquet use is probably neither accurate nor clinically useful. First, we have shown that tourniquet pain is a relatively minor problem in midfoot and forefoot surgery when used in conjunction with an ankle block and limited levels of intraoperative sedation. In only 0.4% of patients in whom a tourniquet was used (988) was tourniquet pain severe enough to require conversion to general anesthesia. Second, rather than a time threshold, we have demonstrated a relatively linear relationship between application time and pain. So, for patients younger than 70 years of age, the tourniquet can be applied comfortably for up to 30 minutes in over 97%. For each 11 minutes beyond this, another 1% of patients report tourniquet pain.
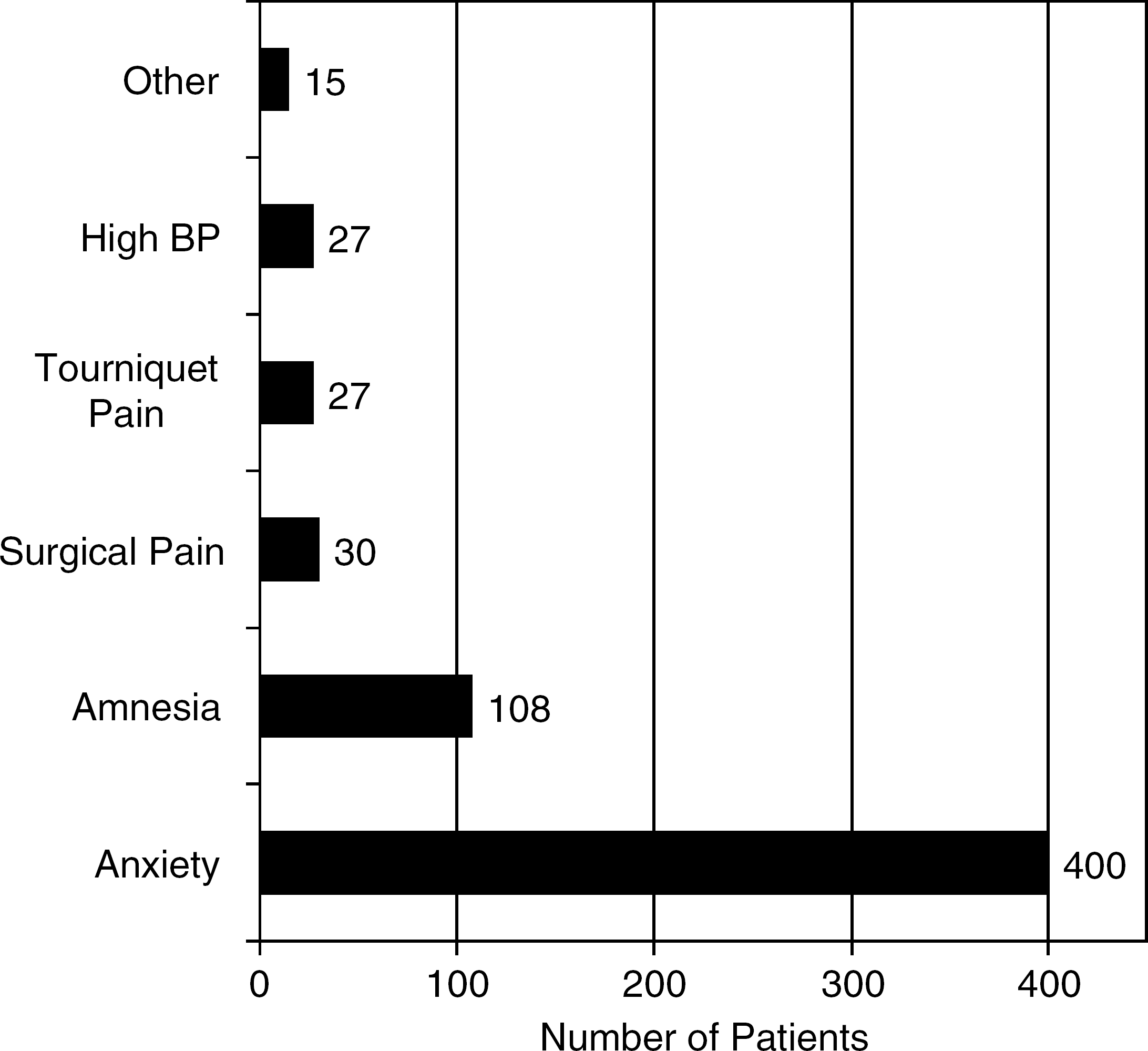
Reasons for sedation. The most commonly cited “other” reason was patient distress at hearing the sound of surgical tools.
This audit showed a profound increase in tourniquet pain in patients 70 years of age or older. On average there was a 3.5 times increase in reported tourniquet pain in this age group for a given application time. The tourniquet can be applied comfortably in this age group for up to 30 min in only 91%. For each 3.2 minutes beyond this, another 1% of patients will report tourniquet pain. The exact reason for this trend is unclear. We speculate that it may be a consequence of physiologic changes in the elderly, such as reduction in subcutaneous tissue or their diminished ability to tolerate stress, such as tourniquet pain. Recent literature has argued that with the administration of sedatives, delirium is a common complication in the elderly, and sedation requirements in this age group are dramatically reduced. 15,16 Furthermore, McGoldrick 16 stated that “Pain control is further complicated (in the elderly) by the fact that the patient's perception and expression of pain are affected by changes in mental status.” It is conceivable that midazolam administered to the elderly altered their expression and perception of pain to a greater extent than the younger age group.
Postoperatively, tourniquet pain in midfoot and forefoot surgery is a relatively minor concern for patients. In this study only 1.9% of patients followed (17 of 899) complained of tourniquet pain at postoperative interview, yet each of these patients would be happy to have the procedure performed again under ankle block with an ankle tourniquet.
Managing Tourniquet Pain
Intraoperative tourniquet pain poses difficulties to both surgeons and anesthetist. The surgeon can respond to pain caused by an ankle tourniquet by reducing tourniquet pressure but does so at the risk of breakthrough bleeding. Alternatively, the anesthetist can manage ankle tourniquet pain by sedating the patient, but does so at the risk of over-sedating the patient. Published data has recognized the importance of sedation, and its ability to prolong patient tolerance of a tourniquet. 8 Yet sedation must be administered with caution, for over-sedation is troublesome because the patient often is unable to follow commands and may move the limb excessively during surgery. This may necessitate a conversion to general anesthesia (Figure 4).
Extended tourniquet times have been noted to lead to progressive hypertension; the mechanism is thought to be a humoral response to the pain. 9,27 Clinically, most hypertensive episodes in this study were anticipated because of preoperative hypertension and accompanying tourniquet pain. Intraoperative episodes can result in breakthrough bleeding and delays in surgery as illustrated in Figure 4, yet most hypertension can be managed adequately by intravenous sedation.
Tourniquet Choice and Application
Some of the problems associated with the use of a tourniquet can be ameliorated by careful application of an appropriate tourniquet. Most surgeons choose to work with a pneumatic rather than Esmarch tourniquet, and the literature supports this popular practice. 10 The pneumatic ankle tourniquet allows more accurate and reproducible control of circumferential compression than the standard Esmarch bandage when used in conjunction with an ankle block. 7,14 It has been shown that Esmarch bandages produce variable tourniquet pressures, which increase linearly with each successive turn of the bandage. It has thus been contended that the Esmarch bandage has an increased risk of nerve damage and complications. 17,18,24
There are still some misconceptions about the placement of a tourniquet. Wakai et al. 28 wrote that “adequate muscle [in the upper arm or thigh] envelopes to protect invested nerves from compression.” This assertion is based on a theoretical argument that has never been clinically proven. 13,25 Rather, recent literature has shown that placement of the tourniquet just proximal to the malleoli leads to significantly less pain than a more proximal site and that the risk of neurologic damage is not increased. 2,5,7,14 It has been established that a wide ankle cuff (15 cm) can create a bloodless field in the limb with less pressure than a narrow cuff. 7,19,21 A wide cuff also minimizes the shear force on the tissue and distributes the force more evenly at all tissue depths. 4 There has been some level of consensus that the pressure of the ankle tourniquet should be maintained at around 200 to 250 mm Hg, allowing for some variation for patient age, blood pressure, and limb circumference and tourniquet design. 4,22 Thus, in this audit, a 15 cm wide conical low-pressure ankle tourniquet (Zimmer) was applied to the supramalleolar region. Inflation pressure usually was maintained at 250 mm Hg.
With correct application of the tourniquet and the option of sedation, our audit has demonstrated that an ankle tourniquet is well tolerated in an awake patient and that a high level of patient satisfaction can be achieved. Both age and tourniquet time were shown to be significant risk factors for tourniquet pain. For patients younger than 70 years of age an ankle tourniquet can be applied comfortably for up to 30 minutes in over 97% and for each 11 minutes beyond this 1% of patients will report pain. The clinician also should be wary of tourniquet pain in patients older than 70 years, particularly when operative times are extended beyond 30 minutes.
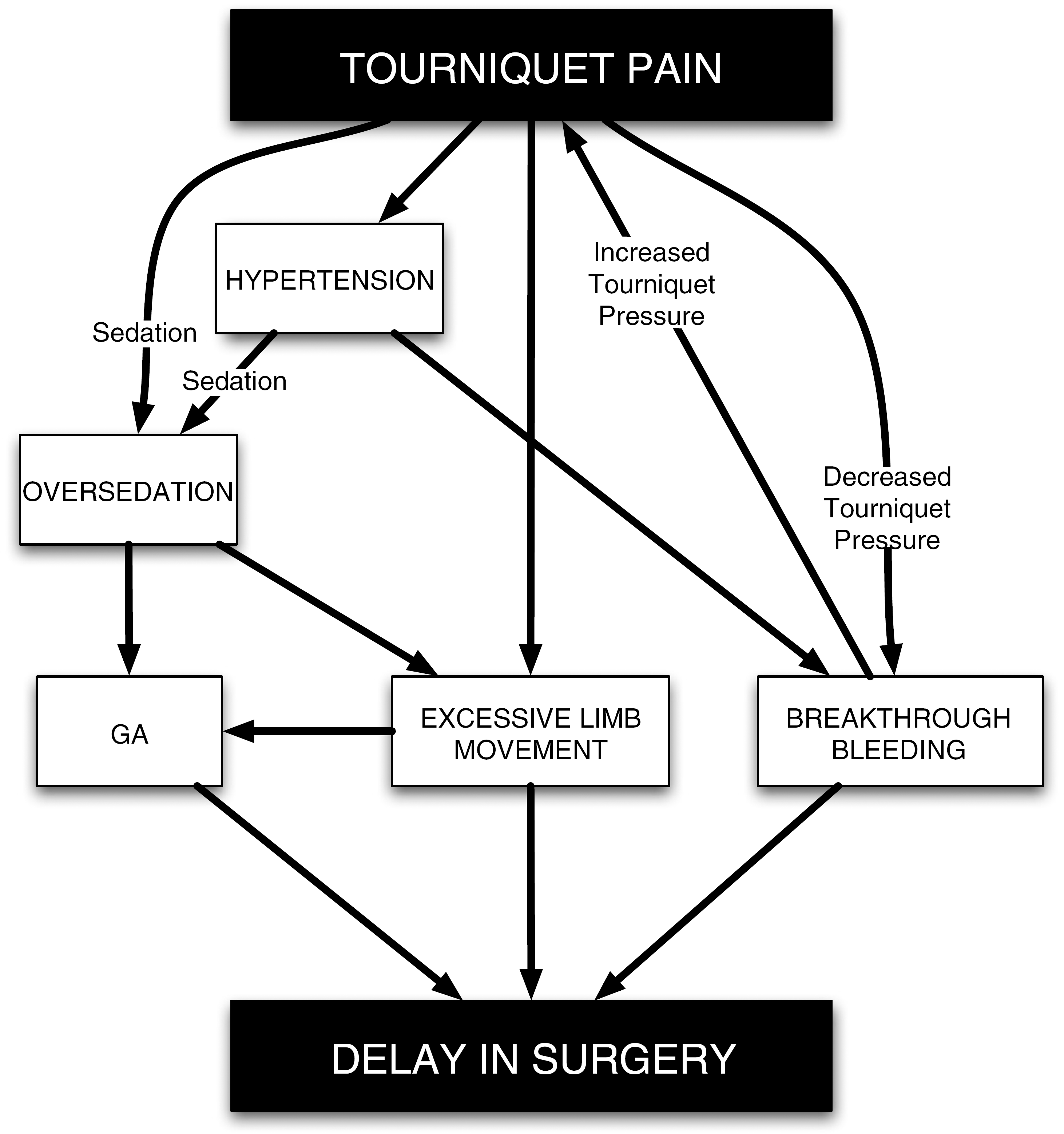
Relationship between tourniquet pain and intraoperative complications.