
Abstract
Background:
Although postural control deficits have been identified after lateral ankle sprains, objective and subjective comparisons of data before and after injury are limited. The purpose of this project was to prospectively assess and compare the changes in postural control and self-reported functional status in athletes who suffer acute lateral ankle sprains. We evaluated postural control and self-reported functional status before injury and at 1, 7, 14, 21, and 28 days after acute lateral ankle sprain.
Methods:
Postural control in single-limb stance and self-reported functional status were evaluated in 460 collegiate athletes during preseason examinations. Twenty-eight athletes suffered a lateral ankle sprain during the competitive season and participated in testing at 1, 7, 14, 21, and 28 days after injury.
Results:
Significant deficits in postural control were noted in both the injured and the uninjured ankles at 1 day after injury compared to the baseline measurements taken during the preseason examinations. Significant differences (p < .05) also were noted between the uninjured and injured ankles at 1, 7, and 21 days after injury.
Conclusions:
After lateral ankle sprain, postural control deficits occur in the injured and uninjured ankles, suggesting a central impairment in neuromuscular control. Changes in self-reported functional status followed a trend of deficit and improvement that was similar to that shown by the postural control data taken after injury, but the two measures did not strongly correlate.
INTRODUCTION
As a marker of functional ankle instability, deficits in postural control, which is the regulation of balance in an upright stance, have been consistently identified in the injured limb after lateral ankle sprains. 5,6,9 –11,12,20,28,30 These side-to-side deficits, however, have been based almost exclusively on comparisons of injured to uninjured limbs. 29 Postural control deficits after injury support the notion of a neuromuscular component of functional ankle instability, but they do not provide insight into the magnitude of impairments seen after ankle sprains. Although Leanderson et al. 15 reported a prospective study of 53 dancers of whom six had suffered lateral ankle sprains, testing was not done at consistent intervals after injury, and inferential statistics were not used for comparisons of data before and after injury.
Further compounding the interpretation of comparisons made after injury is the potential for bilateral neuromuscular deficits after unilateral lower extremity injury. Several reports have suggested that after lower extremity joint injury, neuromuscular deficits exist in both the injured and the uninjured limbs. 2,6,12,14,31 Altered thigh and hip muscle activation patterns have been reported after severe lateral ankle sprains in the ipsilateral and contralateral limbs. 2 Friden et al. 6 reported bilateral postural control deficits after acute ankle sprains; however, these values were compared to a group of healthy subjects and not to the baseline values of injured subjects before the ankle sprains occurred. Hertel et al. 12 reported bilateral improvements in postural control over the course of 1 month after acute ankle sprains; however, no baseline values were available for comparison. Because of the limited comparisons of data before and after injury, bilateral neuromuscular deficits associated with acute ankle sprains have yet to be conclusively established.
In addition to limited comparisons of objective data, there is limited research regarding changes in self-reported functional status after lateral ankle sprains. 26 Although self-reported functional status commonly is incorporated into the evaluation of outcomes in general orthopaedics, it has yet to be adopted in the daily practice of sports medicine. Furthermore, the relationship between self-reported functional status and specific components of functional instability, such as postural control, has not been established.
The purpose of this project was to prospectively assess and compare the changes in postural control and self-reported functional status in athletes after acute lateral ankle sprains. We compared the baseline healthy measures to those recorded after lateral ankle sprain, assessing postural control and self-reported functional status before injury and at 1, 7, 14, 21, and 28 days after an acute ankle sprain.
MATERIALS AND METHODS
Subjects
Before the start of their competitive season, we assessed the postural control and the self-reported functional status of 460 NCAA Division I collegiate athletes (234 men and 226 women) from 23 sports. Each subject was free of existing ankle sprains, as well as acute or persistent orthopaedic pathology. Throughout one academic year, 28 of the 460 athletes (11 males, 17 females; age = 19.7 ± 1.4 years; body mass index = 73.5 ± 19.0 kg; height = 175.0 ± 12.5 cm) suffered acute mild to moderate lateral ankle sprain and participated in testing after injury. All injured subjects were initially assessed by either a certified athletic trainer or a team physician. In addition, only those ankle sprains that resulted in limited participation status for at least two consecutive days were included. Twelve of the sprains were considered mild and 16 were moderate. Seventeen sprains occurred in the right ankle and 11 occurred in the left ankle. Mild sprains were classified as ligamentous pain and laxity at either the anterior talofibular ligament or the calcaneofibular ligament. Moderate sprains were classified as pain and laxity of both ligaments. For the anterior talofibular ligament, laxity was assessed with the anterior drawer test, while the talar tilt test was used to assess calcaneofibular ligament laxity. All injured subjects were free of concomitant fractures and syndesmosis injuries. In accordance with the Office of Regulatory Compliance, all subjects provided informed consent.
Protocol
Postural control was measured as the center of pressure (COP) excursion velocity (VEL) while each athlete maintained a unilateral stance for 15 seconds, for both the left leg and right leg, for three trials with the eyes open. Subjects were asked to maintain a single-leg, barefoot stance on a force plate (Advanced Medical Technology Incorporated, [AMTI] Watertown, MA). They were instructed to stand as motionless as possible with their arms folded across the chest. The nonstance leg was held in approximately 30 degrees of hip flexion and 45 degrees of knee flexion and was not allowed to touch the stance leg during testing. If a touchdown (the nonstance leg touching the ground during data acquisition) occurred or the subject touched the nonstance leg to the stance leg, the trial was terminated and repeated. Previous research conducted in our laboratory (unpublished data) indicated that there are no trends in terms of additional repeated trials being necessary with the injured limb stance versus the uninjured limb stance.
Each trial was 15 seconds long and was modeled after Goldie's previously reported methods which have been shown to be reliable and valid. 7 –9 A rest period of 30 seconds was given between trials. The subjects completed three trials on each leg with the eyes open to allow visual feedback during the maintenance of balance. Subjects, therefore, performed a total of six trials. The order of leg testing was counter-balanced among all subjects during the baseline testing. Pilot data from our lab revealed that individuals were typically unable to complete 15 seconds of eyes closed balance trials on the first day after an ankle sprain; therefore, we did not incorporate eyes closed trials in our current study.
The Athletic Training Outcomes Assessment (ATOA) self-report survey 1 and the SF-12 Health Survey 32 were completed before the postural control testing. Athletes were instructed to complete the health surveys based upon their health status at the time. A detailed health interview also was conducted. The preseason assessments were done either during the usual physical examinations or during a scheduled session before the beginning of the competitive season.
In cooperation with the team physicians and certified athletic trainers, athletes who suffered a mild or moderate lateral ankle sprain and missed at least 2 consecutive days of athletic participation without limits were tested within 1 day of return to full weightbearing ambulation. Although specific lateral ankle sprain rehabilitation protocols may have varied among athletic trainers and physicians at our institution, they all followed a functional rehabilitation program that emphasized control of pain and swelling, range of motion, strengthening, and balance exercises, as well as gradual return to functional activities, including weightbearing as tolerated 24 hours after injury, with an emphasis on functional weightbearing exercises. We did not control the treatment intervention or the rehabilitation protocol.
After the initial assessment following injury, postural control and self-reported functional status were measured at 7, 14, 21, and 28 days after the injury. Testing was done in one of five different athletic training rooms or the athletic training research laboratory. The same certified athletic trainer conducted all testing that was done after injury.
Instruments
Postural control was measured with an AMTI Accusway force plate (AMTI Inc., Watertown, MA) interfaced with a laptop computer using SWAYWIN95 software (AMTI Inc., Watertown, MA). Three-dimensional ground reaction forces were collected at 50 Hz. The AMTI force plate measures translational forces (Fx, Fy, Fz) and moments of force (Mx, My, Mz), and the software program calculates COP trajectories. The origin of the COP path was the initial point of COP during each trial. The dependent measure was the COP excursion velocity, defined as the distance or length of the path created by the COP divided by the duration of the trial.
Self-reported health status was measured with a modified version of the ATOA self-report survey 1 and the SF-12 Health Survey. 32 The ATOA self-report survey was developed to measure improvement in function in injured physically active individuals. 1 It consists of 12 items that can produce individual item scores as well as three composite scores. The composite scores include a functional outcomes subgroup (three items), a physical outcomes subgroup (six items), and an overall score (all 12 items). The 12 items include activities of daily living, work activities, sports-recreation-wellness (grouped as functional outcome), movement, strength or power, endurance, motor abilities, body structure, sensory (grouped as physical outcomes), general health status, specific medical condition, and psychosocial status. 1 The survey was modified from its original version to exclude the two items that measured satisfaction with treatment and satisfaction with the certified athletic trainer. In addition, the pretreatment and posttreatment responses were not recorded on the same survey page. Therefore, the subjects did not see their previous responses. This version of the ATOA has been shown to be reliable and sensitive to changes in the health status of physically active individuals. 4
The SF-12 Health Survey, 32 adopted from the Medical Outcomes Study Short Form Health Survey (SF-36), is a 12-item health survey that is an accepted outcomes questionnaire that can be used to evaluate a patient's vitality and general health-related functioning. 32,33 It is considered one of the best generic measures available for use across diverse populations 32 and has been administered to measure the effects of chronic diseases, the effects on general health, and differences in patient populations. 32 It consists of 12 items separated into eight dimensions that measure physical and mental health. The eight dimensions include: 1) physical functioning, 2) role limitations due to physical health problems, 3) role disability due to emotional health problems, 4) general mental health (1 to 4 estimated with two items), 5) vitality, 6) social functioning, 7) bodily pain, and 8) general health perception (estimated with one item each). When totaled the SF-12 produces two scores: the physical component summary scale (PCS) and the mental component summary scale (MCS).
Statistical Analysis
Means for COP VEL were calculated for both limbs by averaging the three trials for each testing session. Separate 2 × 6 (side × time) repeated measure analysis of variances (ANOVA) were calculated for postural control data. Separate repeated measures of ANOVA also were calculated for ATOA and SF-12 data. To determine the correlation of balance and self-reported data, delta scores (change scores) were calculated for each measure between each of the testing sessions. Spearman rho coefficients between the postural control delta scores of the injured ankle and the ATOA (total composite score and individual items) and the SF-12 (total composite score only) delta scores were then calculated for the following intervals: baseline–day 1, day 1 to day 7, day 1 to day 28.
RESULTS
Postural Control
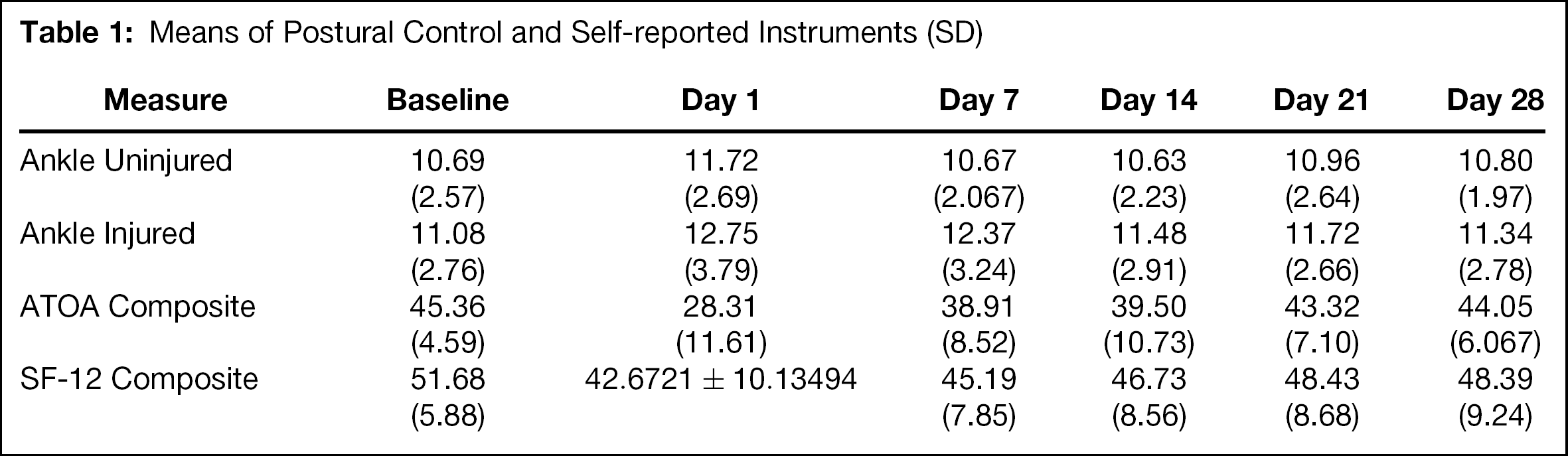
There were significant main effects for both time (F = 3.22, p < .01) and side (F = 8.90, p < .01) for the postural control measure. Analysis revealed that compared to the baseline data, significant deficits in postural control existed for both the injured and the uninjured ankles (p < .05) at day 1 (Figure 1). Significant deficits also were found at day 7 in the injured ankles (p < .05). Furthermore, there were significant differences (p < 0.05) between the healthy and injured ankles at 1, 7, and 21 days. Although the injured ankle values were greater than the uninjured values at days 14 and 28, these differences were not statistically significant. Whereas both the injured and uninjured ankles improved 1 day after injury, the healthy ankle approached baseline values sooner, with the injured ankle showing significant deficits until 14 days after injury. Means for the postural control and the self-reported data are reported in Table 1.
Self-reported Assessment
For both the ATOA (p = .001) and SF-12 data (p = .001), significant time effects existed. Analysis revealed that for both surveys, scores were significantly lower than baseline scores at 1, 7, and 14 days after injury, with scores returning towards baseline beginning at day 7 (Figure 2). Spearman rho coefficients produced only low correlations (r < .49) between ATOA scores and COP VEL, and the SF-12 and COP VEL (Table 2).
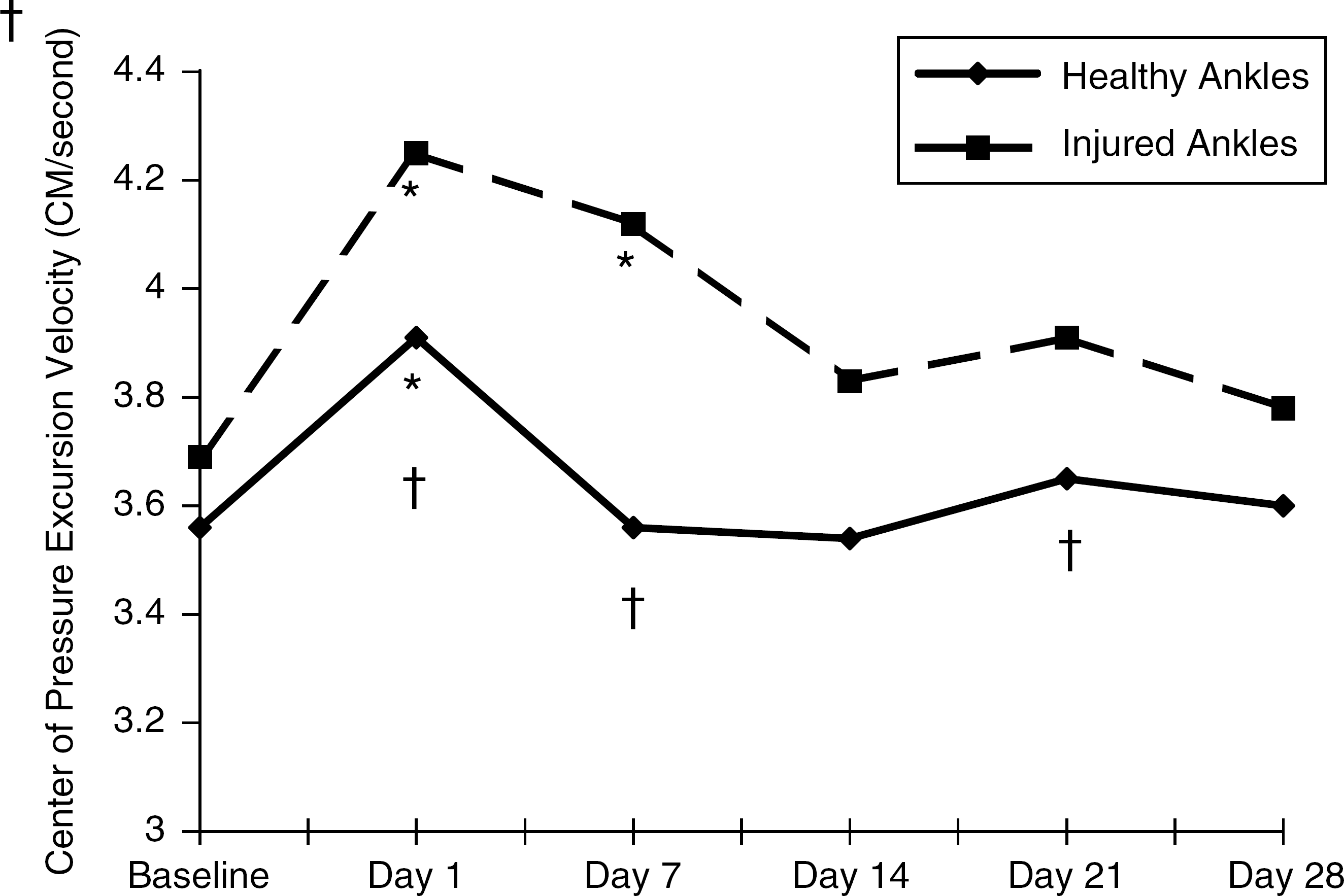
Eyes open postural control data for the injured and healthy ankles illustrates the postural control deficits that occurred immediately after injury and the subsequent return towards baseline values. *Indicates significant difference from baseline (p < .05); †Indicates significant difference between healthy and injured ankle (p < .05).
Means of Postural Control and Self-reported Instruments (SD)
DISCUSSION
Our results indicate a significant deficit in COP VEL in both the injured and uninjured limbs 1 day after injury, as well as at seven days in the injured limbs when compared to baseline measures. The COP VEL is the distance or length of the path created by the COP divided by the duration of the trial. Side-to-side differences in COP VEL were present at 1, 7 and 21 days as well. Significant changes in self-reported functional status occurred after injury, and although these data followed a similar trend, the objective and subjective measures were not strongly correlated.
Our primary finding was that bilateral impairments in postural control during single-limb stance occurred after unilateral ankle sprains. Injured subjects demonstrated inferior postural control on both their injured and their uninjured limb after acute ankle sprain compared to baseline values. Our comparison of measures of postural control after injury to baseline measures taken before injury allowed us to definitively demonstrate bilateral deficits after a unilateral acute ankle sprain The existence of bilateral impairment after an ankle sprain does not support the seminal hypothesis by Freeman et al. of ligament mechanoreceptor damage causing neuromuscular control deficits after injury. 5 The existence of deficits in the uninjured contralateral limb indicates that a centrally mediated mechanism is contributing to the neuromuscular deficits associated with acute joint injury.
Previous researchers have offered evidence of bilateral neuromuscular control deficits after unilateral ankle sprain; 2,6,12 however, the lack of preinjury data made definitive interpretation of these results impossible. Friden et al. 6 demonstrated impaired postural control in both the involved and uninvolved limbs 3 and 8 days after an ankle sprain compared to healthy subjects. Hertel et al. 12 reported bilateral improvements in postural control measures on injured and uninjured limbs over the course of four weeks after an ankle sprain. It must be noted that in these studies, as in our current study, there were more pronounced postural control impairments in the injured limbs than in the uninjured limbs.
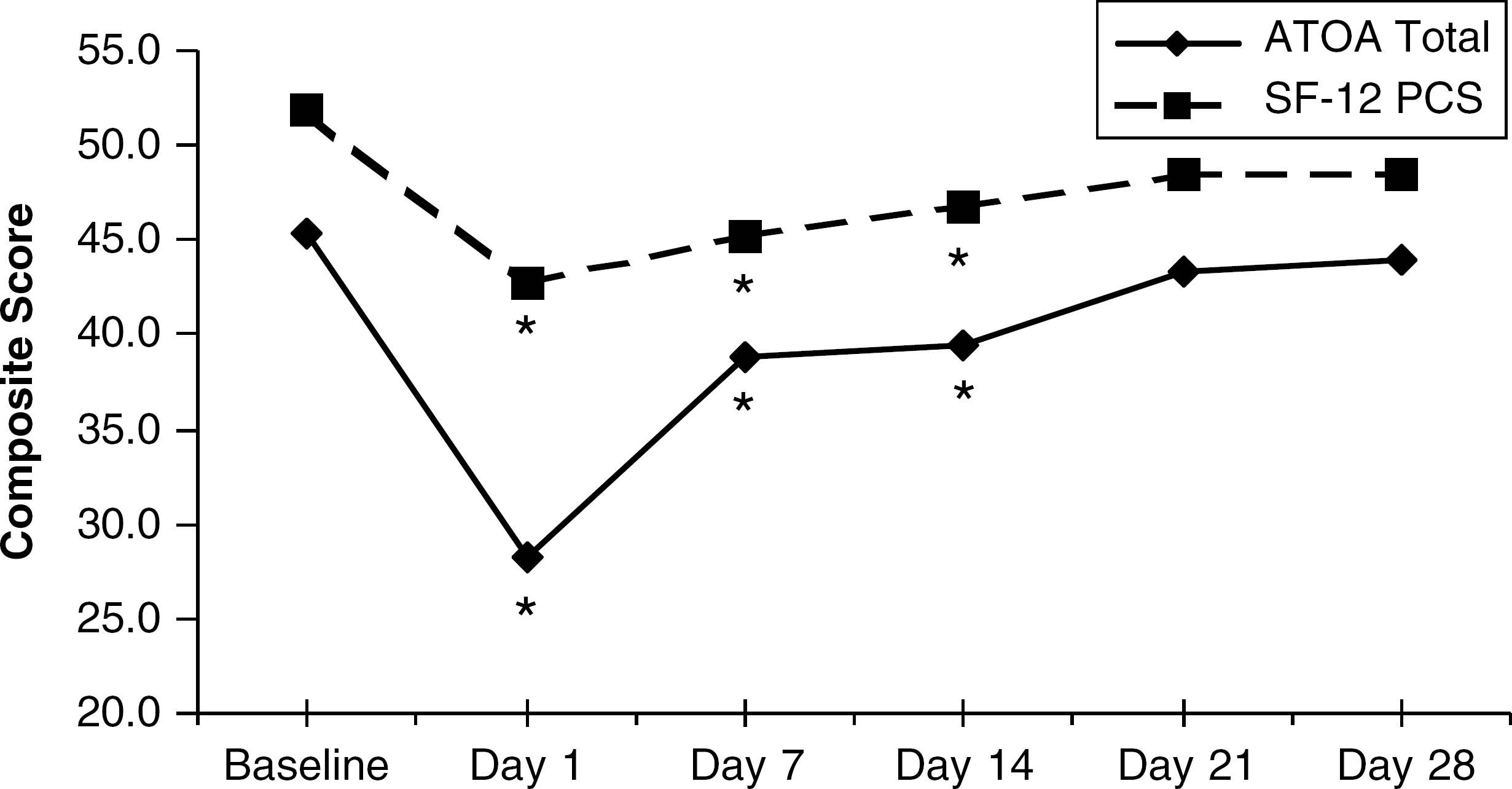
ATOA and SF-12 composite scores. Changes in self-reported assessment after injury and the subsequent return towards baseline values. *Indicate significant difference from baseline (p < .001).
Spearman Coefficients Between Change Scores of ATOA, SF-12, and COP VEL
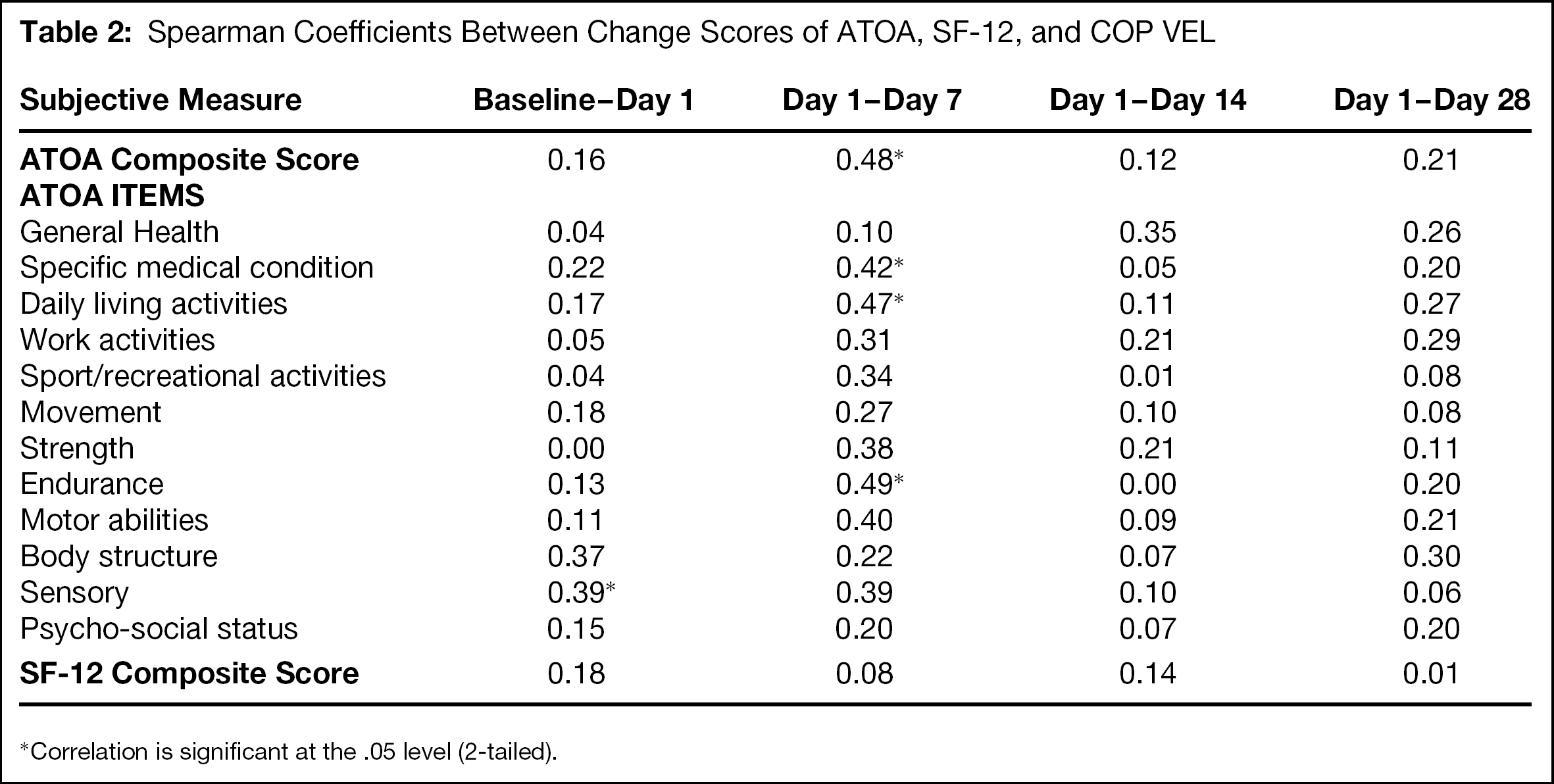
Correlation is significant at the .05 level (2-tailed).
The clinical implications of our current postural control findings must be considered. Acute inflammation associated with ankle sprains likely led to neuromuscular inhibition, and, thus, impaired postural control in both the injured and uninjured limbs. As inflammation subsided, the contralateral deficits were negated. This is evidenced by the uninvolved limb only being significantly worse than baseline at 1 day after injury. The ability of antiinflammatory modalities and medications to lessen the neuromuscular effects associated with acute joint injury is an area that warrants future research. The consequences of impaired postural control bilaterally also deserve consideration; poor postural control has been shown to increase the risk of ankle sprains. 16,28 However, this has not been studied in athletes with impaired postural control after a recent ankle sprain. Returning athletes to play too quickly after an ankle sprain (i.e., before return of preinjury postural control) may predispose them to further injuries.
As an adjunct to objective measurements, self-reported functional status has become a valuable tool in orthopaedic rehabilitation. 1,13 Whereas assessing self-reported outcomes has been implemented to some degree in most health care settings, it has yet to become standard in most sports medicine settings. Survey instruments are used to assess general, condition-specific, or patient-specific outcomes 22,34 and typically assess clinical indicators, such as activities of daily living, general health, work activities, and psychosocial status. The instruments used in this study, the ATOA and SF-12, are considered generic instruments, although the ATOA was designed for assessing the health status of physically active patients. 1
Our results suggest that changes in self-reported functional status, as reported with generic instruments, follow a trend similar to that of postural control after lateral ankle sprain. Comparable to the injured ankle COP VEL scores, self-reported functional status scores were significantly worse immediately and 7 days after injury. Unlike the self-reported functional status scores, however, COP VEL scores were not significantly worse 14 days after injury than baseline measures. Thus, at 14 days after injury, subjects continued to subjectively report deficits even though postural control had returned to close to baseline values. Furthermore, the COP VEL and self-reported functional status scores were not highly correlated at any interval.
One explanation for the low correlations is that although linked to such anomalies as pain, inflammation, and muscle weakness, self-reported function instruments are not sensitive to improvements and deficits in neuromuscular performance. Through a retrospective study, Rose et al. 26 assessed both balance and self-reported functional status using the Olerud and Molander questionnaire after noncontact ankle sprains at 3, 7, and 14 days after injury. Similar to our findings, they reported significant improvements in questionnaire scores. They did not, however, find significant differences in balance scores between the injured subjects and the controls, although they reported that the injured subjects appeared to be less stable than the controls. As in our study, other authors have compared subjective and objective measures after lower extremity injury. Rozzi et al. 27 compared the effects of balance training on balance parameters and self-reported functional status in subjects with functional ankle instability. Although significant improvements were found for balance and functional assessment, a relationship between functional and subjective assessment status was not established. 27 Munn et al. 17 reported that although self-reported functional status scores can indicate impairment in subjects with ankle instability, agility scores were not highly correlated. Comparable studies by Wilson and Gansneder 35 and Cross et al. 3 seem to indicate that self-reported limitations alone have limited value in predicting variance in disability duration after acute ankle sprains. In a series of studies on patients with anterior cruciate ligament problems, Risbert et al., 23 –25 reported that subjective scales can be sensitive to change over time; however, they vary in their relationship to neuromuscular impairments and disability. Pfeifer and Banzer, 21 Neeb et al., 19 and Wojtys and Hutson 36 also suggested that self-reported measures are not consistently related to objective measures.
A second explanation for the lack of high correlation values between COP VEL scores and self-reported functional status scores is that the generic self-reporting tools used in this study are not sensitive enough to detect changes in neuromuscular control. No items on either the ATOA or the SF-12 exclusively address balance or other parameters of neuromuscular control.
To clinically interpret our subjective results, it appears that changes in neuromuscular markers of functional instability, in this case postural control, are not strongly correlated with self-reported functional changes. This notion supports the clinical practice of implementing both subjective and objective assessment strategies when evaluating status after lateral ankle sprains.
In conclusion, our results suggest that immediately after a lateral ankle sprain, bilateral postural control deficits exist. Although previous research has demonstrated deficits in postural control in the injured limb, deficits in the uninjured limb have not been compared to preinjury measures. These bilateral deficits suggest alterations in centrally-mediated neuromuscular control processes after acute joint injury. Furthermore, although changes in self-reported health status follow a trend similar to changes in postural control after lateral ankle sprains, changes in these two measures were not highly correlated. These findings support the use of both subjective and objective measures, as they may reflect distinctly different components of impairment and recovery.