
Abstract

Introduction
Encouraged by intermediate results of second generation ankle implants, many surgeons are expanding their indications for total ankle arthroplasty 1,3,5 As these devices are used in younger and more active patients, it is likely there will be an increasing number of patients with failed implants as is seen with hip and knee replacements. A major concern with ankle replacement surgery is late salvage. With significant bone loss, revision arthroplasty may not be possible, leaving arthrodesis with structural autograft or even amputation as the only options. 4
The New Jersey Low Contact Stress™ (Endotec, South Orange, NJ) (NJLCS) total ankle implant requires relatively little initial bone resection. 2 The implant relies on intact medial and lateral talar walls (medial and lateral ankle gutters) for stability. Unfortunately, subsidence of the talar component is a common mode of failure for any ankle implant, and this results in loss of the ankle gutters, making revision with a similar implant impossible. The Agility™ (DePuy, Warsaw, IN) total ankle does not rely on talar walls for stability. In fact, much of the talar walls are not resected, but the inner medial and lateral malleolar walls are resected during Agility™ ankle arthroplasty, which makes it a potential candidate for revision procedures. The NJLCS tibial component has a stem with a porous surface for bone ingrowth. Removal of this stemmed component has not been well described, but there is reasonable concern that replacement of this may cause major bone loss or even distal tibial fracture during revision procedures with disastrous results. The purpose of this paper was to describe the surgical technique of revising a NJLCS ankle arthroplasty to an Agility™ prosthesis. This technique permits ankle arthroplasty exchange with limited bone damage and may help surgeons with patients in need of revision of a problematic NJLCS arthroplasty. We are not aware of any surgical description of this specific problem nor any surgical guides or instrumentation.
Case report
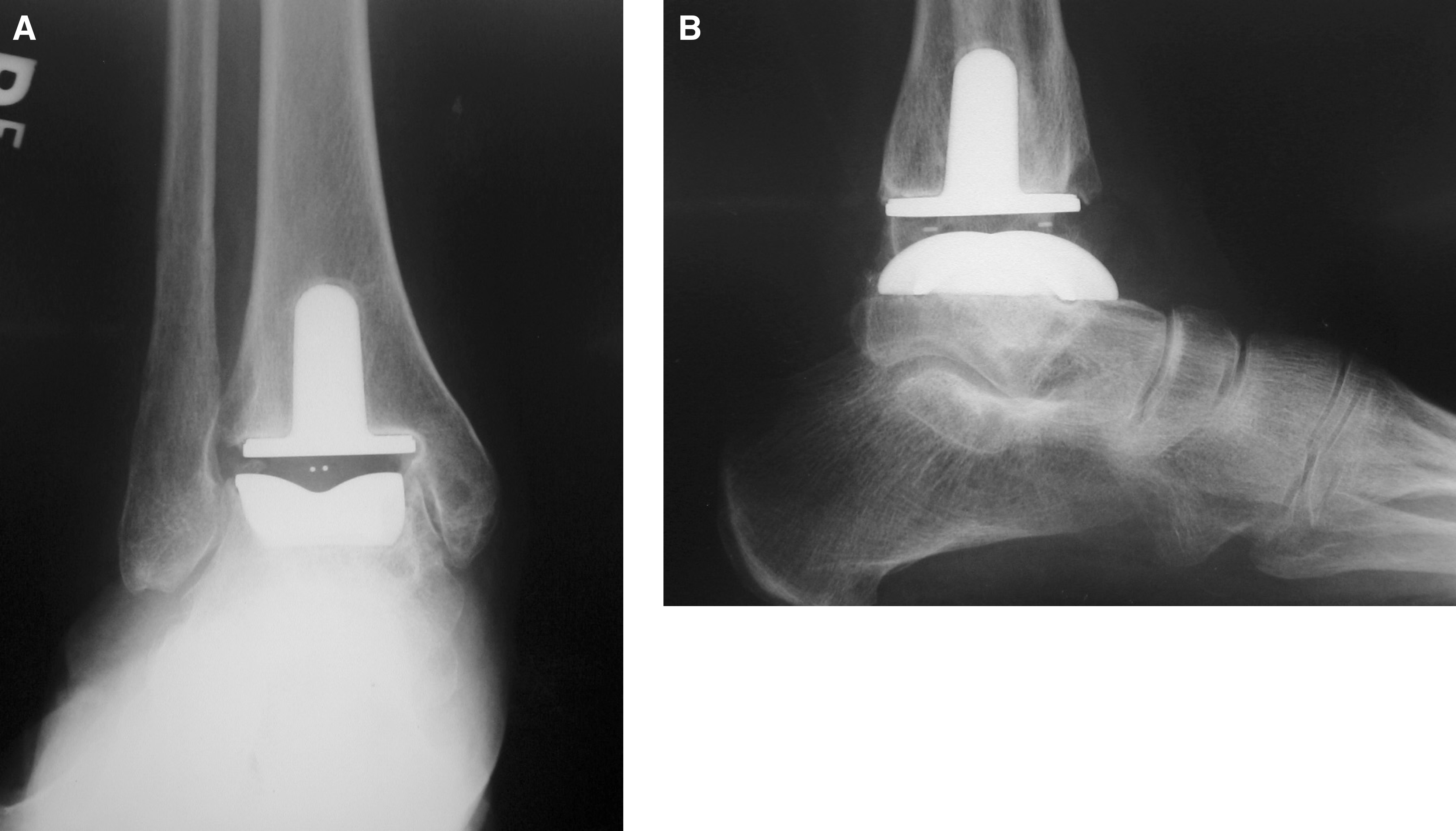
A 52-year-old healthy woman who had a total ankle arthroplasty 6 years earlier was referred to the senior author (STH) for diffuse chronic ankle pain that had been increasing gradually over the past 18 months. Clinical examination of her ankle revealed normal alignment and an active range of motion of 20 degrees of plantarflexion and 5 degrees of dorsiflexion with pain about the medial and lateral malleoli during motion. The soft tissue envelope appeared healthy with no signs of infection. Erythrocyte sedimentation rate and C-reactive protein were within normal range. Anteroposterior and lateral radiographs of her ankle (Figure 1, A and B) revealed subsidence of the tibial component of the NJLCS total ankle arthroplasty with signs of bone resorption and malleolar impingement. Her pain was attributed to impingement of the remaining talar walls against the malleoli. Many months of nonoperative treatment including analgesics and activity modification provided no relief, and revision of the ankle prosthesis was offered to the patient. In view of the marked distal tibial bone loss, the surgical options included ankle arthrodesis with bone block interposition as described by Kitaoka 4 or removal of the NJLCS arthroplasty and implantation of a total ankle arthroplasty better suited to deal with greater bone loss, such as the Agility™. After informed consent, the patient elected to undergo revision total ankle arthroplasty.
The procedure was done with the patient under general anesthesia. A tourniquet was applied at the level of the thigh. A distractor was not used to facilitate movement of the foot while removing the prosthesis. The previous straight vertical anterior incision was used, passing between the anterior tibial tendon medially and the extensor hallucis longus tendon laterally. The neurovascular bundle was protected laterally, and the ankle joint was opened. Scar tissue was removed with a rongeur, and sharp dissection was used to expose the edges of the failed implants. Bony impingement was present in the medial and lateral gutters. The intervening polyethylene component was removed and macroscopic inspection did not show significant wear. A 3-mm chisel was used to undermine and loosen the talar component, taking care not to remove any underlying talar bone, and the talar component came out without difficulty. Under fluoroscopy, a true anteroposterior view was obtained and the intramedullary stem of the tibial component was identified. To locate the stem, two 1.6 mm Kirschner wires were inserted, one at the proximal medial edge and one at the proximal lateral edge of the stem. From these two Kirschner wires, straight longitudinal lines were drawn distally, representing the medial and lateral sides of the stem. An oscillating saw was used along these lines to arrive precisely on the stem. The anterior block of bone was carefully removed with a 3-mm chisel, with care taken to maintain its maximal thickness. The block of bone removed should be the same size as the stem (15 mm wide, 30 mm high, and at least 10 mm thick). Removal of the block of bone revealed the entire stem of the beaded tibial component (Figure 2). The 3-mm chisel was used to free the portion of the stem protruding into the medullary canal. The prosthesis was then gently tapped from the top and removed without resulting in a fracture of the distal tibia. The talar bone was not damaged during removal of the tibial component. Once all failed implants were removed, a saw was used to create a level surface of the talus. This technique allowed the original bony cuts to remain at the exact levels. Subsidence of the NJLCS implants resulted in a loss of some talar bone, so the “thicker” Agility™ implant could be inserted without any additional bone resection. A revision Agility™ talar component (the “flanged” talus) was used, which is actually 2 mm taller than standard implants (Figure 3). After making the appropriate 20-mm groove for the talar keel, the permanent prosthesis was inserted. To accommodate the fin of the tibial component, a 3-mm wide by 4-mm high cut was made in the lower medial side of the anterior block of bone, and it was replaced into its original location and secured with a 2.7-mm quarter tubular plate and two screws. The syndesmosis was prepared and fused before insertion of the final components. It was stabilized with a one-third tubular plate and two lag screws. No bone graft was used.
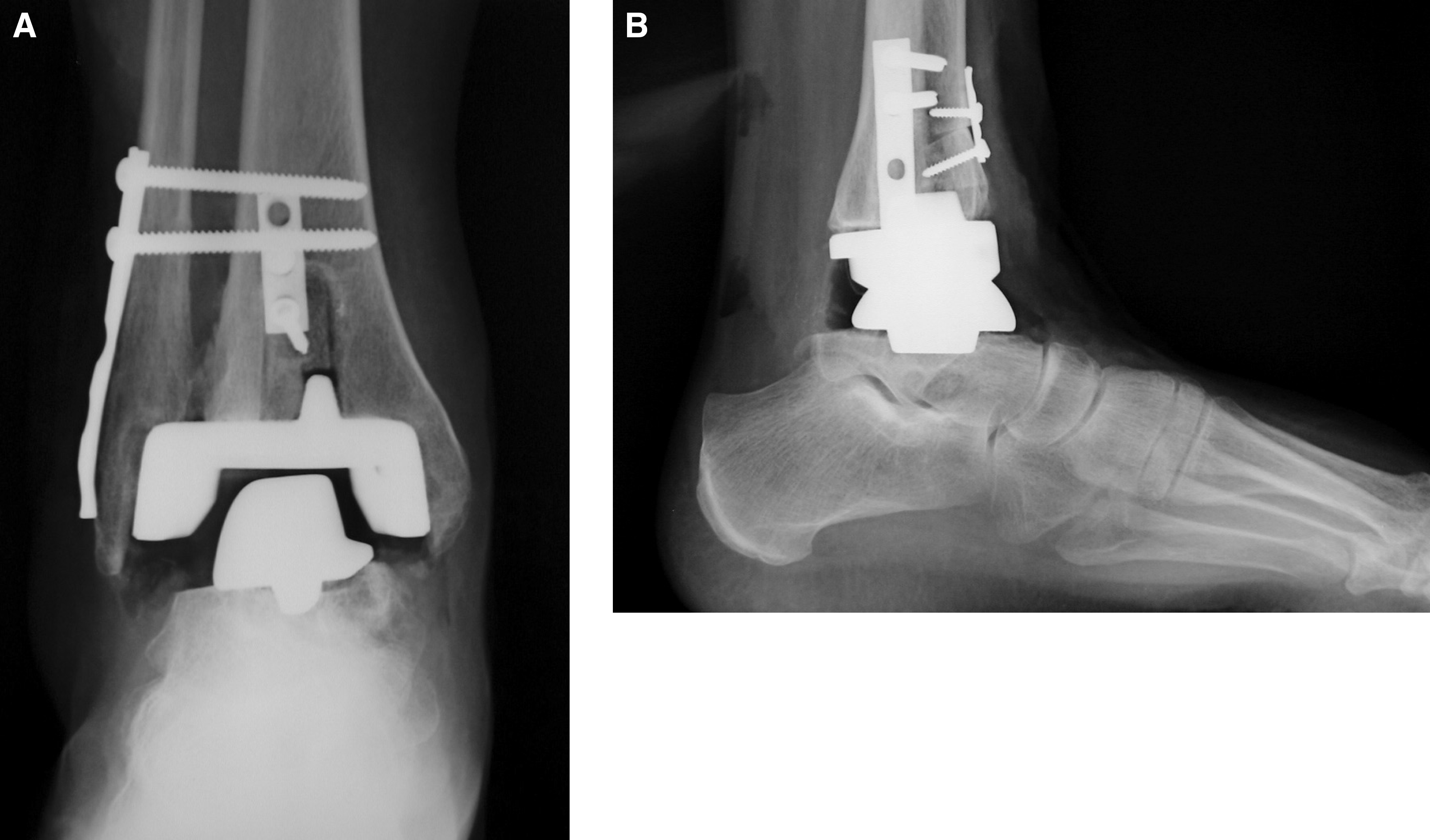
After wound closure and dressing, the ankle was placed in a short-leg padded cast. Postoperative management consisted of touch-down weightbearing for the first 6 weeks. The patient was allowed to perform some static standing on the leg to facilitate compression of the implant to the host bone. The patient progressed to full weightbearing at 6 weeks from the date of surgery, after syndesmotic fusion was sufficient to support the tibial tray. At this time the cast was removed and physical therapy was begun to increase ankle motion. At 5 months, the patient could walk without crutches and was pain free. Active ankle range of motion was 15 degrees of plantar flexion and 5 degrees of dorsiflexion. Radiographs revealed good alignment with no evidence of loosening (Figure 4, A and B).

Intraoperative view after removal of the block of bone revealing the entire stem of the beaded tibial component. The block of bone is shown in the upper part of the picture.

Intraoperative view demonstrating placement of the Agility™ ankle prosthesis. The anterior block of bone was placed back after 3 mm wide by 4 mm high cut was made in its lower medial side to accommodate the fin of the tibial component.
Discussion
There are several models of ankle arthroplasty available, each with its specific design and indications, among them the NJLCS™ and the Agility™. In case of revision, these brands offer a series of revision components that are thicker or larger. However, in some circumstances loosening and bone resorption are such that an alternative prosthesis is required. The Agility™ is better capable of dealing with bone loss by structurally resurfacing a larger portion of the joint. It is more versatile in the sense that it is a semiconstrained ankle whose stability does not rely on the presence of the walls of the talus. Conversely, the NJLCS™ prosthesis is a malleolar preserving type of implant that leaves intact both the talofibular joint and the joint between the medial malleolus and medial wall of the talus. In this latter case, if subsidence and bone loss are significant enough to compromise malleolar function, it may become necessary to exchange the prosthesis. In such a setting the Agility™ can offer a solution. The surgical technique described here provides an option for salvage of a failed NJLCS prosthesis.
As our experience grows with revision total ankle arthroplasty, we have noted several key principles that are relevant to this case. The first is to preserve as much bone as possible during revision. By using very thin chisels, minimal bone is destroyed during implant removal. In the case of revision of a NJLCS ankle, a controlled osteotomy of the distal tibia is necessary to fully expose and free up the stem. With a porous ingrowth surface, there is the potential for catastrophic bone loss during implant removal. It is necessary to have revision components available. There is a thicker polyethylene liner and also wide-based talar components that can take up space in the case of bone loss. The full spectrum of implant sizes should be available, as well as small and mini-fragment reconstruction sets in case of fracture. Finally, the surgeon must adhere to the principles of primary total ankle arthroplasty. With revision arthroplasty, the cause of failure must be identified. Often, it will be subsidence of the components into bone, in which case revision with wider components (which decrease contact pressures at bone-implant interfaces) may be necessary. Both static and dynamic muscle and ligament balance must be neutral. Muscle lengthenings, tendon transfers, corrective osteotomies or fusions may be required. When these principles are rigidly adhered to, our early experience has shown revision total ankle arthroplasty to be a viable option after failed arthroplasty.
Other diagnostic and therapeutic interventions could have been considered for this patient. Not all patients with subsidence of an ankle arthroplasty need revision. The work-up of the painful total ankle arthroplasty can be complex and is beyond the scope of this discussion. In this patient who had more than 1 year of pain and failure of long-term nonoperative treatment, the senior surgeon thought revision arthroplasty was the most appropriate plan of management.