
Abstract
Background: Diabetic foot ulcers, foot infection, Charcot foot arthropathy, and lower extremity amputation have a severe negative effect on the health-related quality of life in individuals with diabetes. The purpose of this study was to determine if there is a relationship between these negative effects and cognitive impairment or clinical depression. Methods: Sixty adults with diabetes completed the Short Form 36 (SF-36) Health Survey questionnaire, two screening examinations for cognitive function (Mini Mental Exam and Clock-Drawing Test), and a screening examination for depression (Zung Self-Rating Depression Scale). The two focus groups were composed of 20 subjects each who were undergoing treatment for (1) diabetic foot ulcers or active Charcot foot arthropathy or (2) lower extremity amputation. Twenty diabetic individuals without foot-related morbidity but with evidence of peripheral neuropathy as measured by insensitivity to the Semmes-Weinstein 5.07 (10 gm) monofilament comprised the control group. Results: The SF-36 Health Survey score was significantly impaired in both the diabetic foot ulcer and Charcot arthropathy group (p < 0.001) and amputee (p < 0.000) group. There was no evidence of cognitive impairment or depression in either group. The negative impact on health-related quality of life was similar in both focus groups (p < 0.314). Conclusion: The results of this preliminary study suggest that the negative impact on health-related quality of life in diabetic patients with foot ulcers or Charcot foot arthropathy may be as severe as in similar patients with lower extremity amputation. The negative effect did not seem to cause cognitive impairment or clinical depression in either focus group.
Introduction
Diabetic foot ulcers precede 85% of diabetes-related lower extremity amputations. Preventive strategies of foot-specific patient education, prophylactic skin and nail care, and therapeutic footwear currently are well-accepted modalities capable of decreasing the risk of diabetic foot ulcers. 19 Once a diabetic patient has a lower extremity amputation the risks of amputation of the contralateral limb 10,11,13 and of death are increased. 12,18
Diabetes-related morbidity negatively affects patients' perceived quality of life, as well as substantially inhibiting the ability to perform daily activities. 6 Peters et al. 17 reported that diabetic patients with transtibial amputations had significantly higher impairment scores on the Sickness Impact Profile than patients without amputations or with forefoot amputations only. There is substantial evidence demonstrating both cognitive dysfunction and clinical depression in individuals with diabetes, 5,7,8,23 and they have been shown to be more likely to develop clinical depression than similar individuals without diabetes. 1,3,14 While many experts think that depression and impaired cognition play an important role in negatively perceived quality of life, we are not aware of any attempts to correlate cognitive or psychological impairment with diabetic foot morbidity. The goal of this pilot project was to develop a simple screening battery for adults with diabetes and attempt to compare health-related quality of life in those with and without foot problems and those who have had lower extremity amputation.
Materials and Methods
The two study focus groups consisted of 20 randomly selected adults with diabetes who were undergoing treatment for diabetic foot ulcers or Charcot foot arthropathy and 20 receiving followup care at least 6 months after lower extremity amputation. Amputation levels ranged from digital amputation to transtibial. The amputee group was not divided based on level of amputation. A control group consisted of 20 diabetic individuals with no evidence of foot morbidity but with evidence of peripheral neuropathy as determined by insensitivity to the Semmes-Weinstein 5.07 (10 gm) monofilament. These individuals participated in the study at the time of receiving routine medical care.
After informed consent was obtained, each person completed four surveys and had a lower extremity examination. The SF-36 Health Survey was used to evaluate perceived functional status and health-related quality of life. This survey contains 36 questions divided into eight categories related to physical functioning and role limitations due to physical health, emotional problems, energy or fatigue, emotional well-being, social functioning, physical pain, and general health. All questions were scored on a descending scale with a value of 100 representing the highest level of functioning possible. Scoring was based on standardized methods. 15,16,9
We chose two simple screening tests to evaluate cognitive function. The level of cognitive functioning was determined by the Clock-Drawing Test and the Mini Mental Examination. 2,4,24 The Clock-Drawing Test specifically evaluates frontal lobe function. 20,21 Each subject was asked to draw a clock, with four points being awarded for each of the following completed tasks: producing a full circle, including all twelve numbers, placing the numbers in the correct position, and drawing the hands of the clock to a correct, predetermined time (Figure 1). The Zung Self-Rating Depression Scale was used to evaluate individuals for the presence of clinical depression. The Zung scale is a self-rating depression scale, consisting of 20 questions. It has been used in a variety of mental health settings, including psychiatric analysis, primary care, drug trials, and research. 22,25
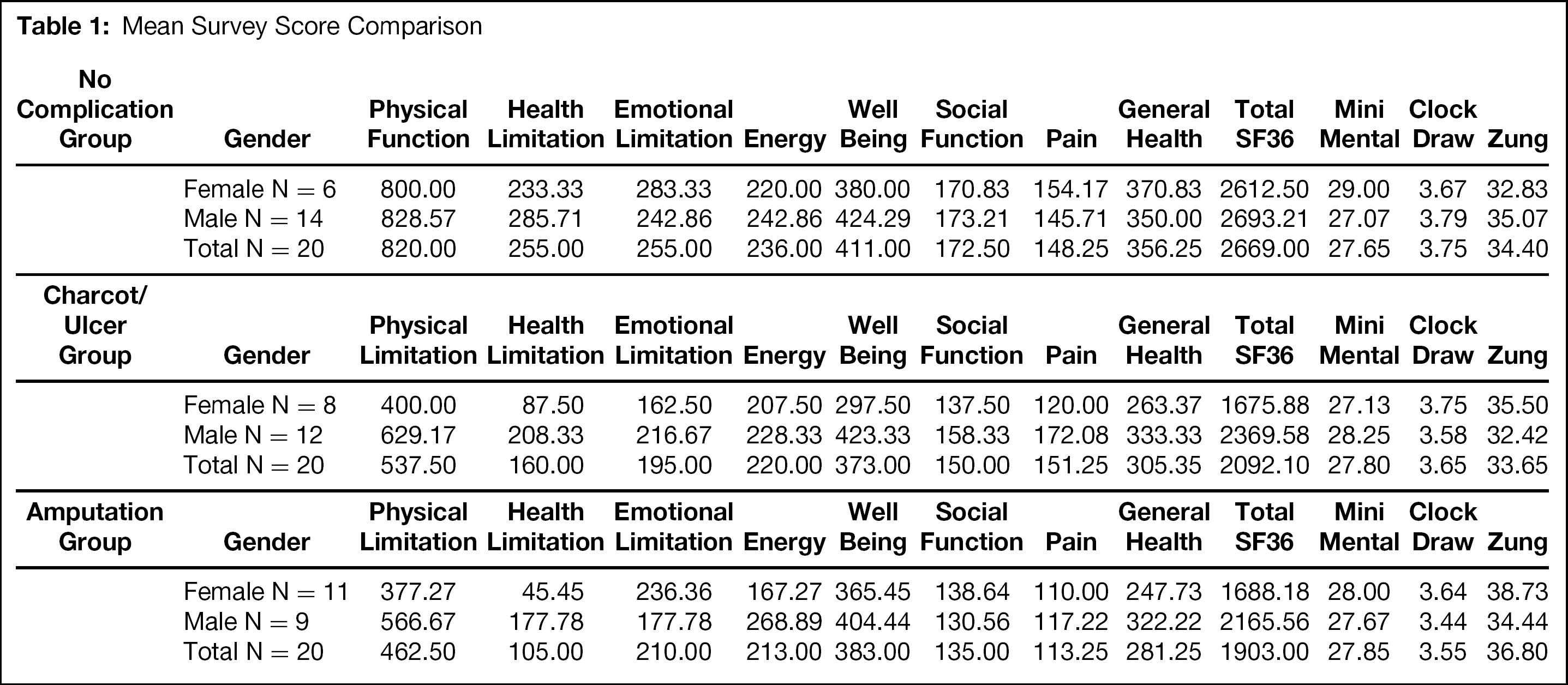
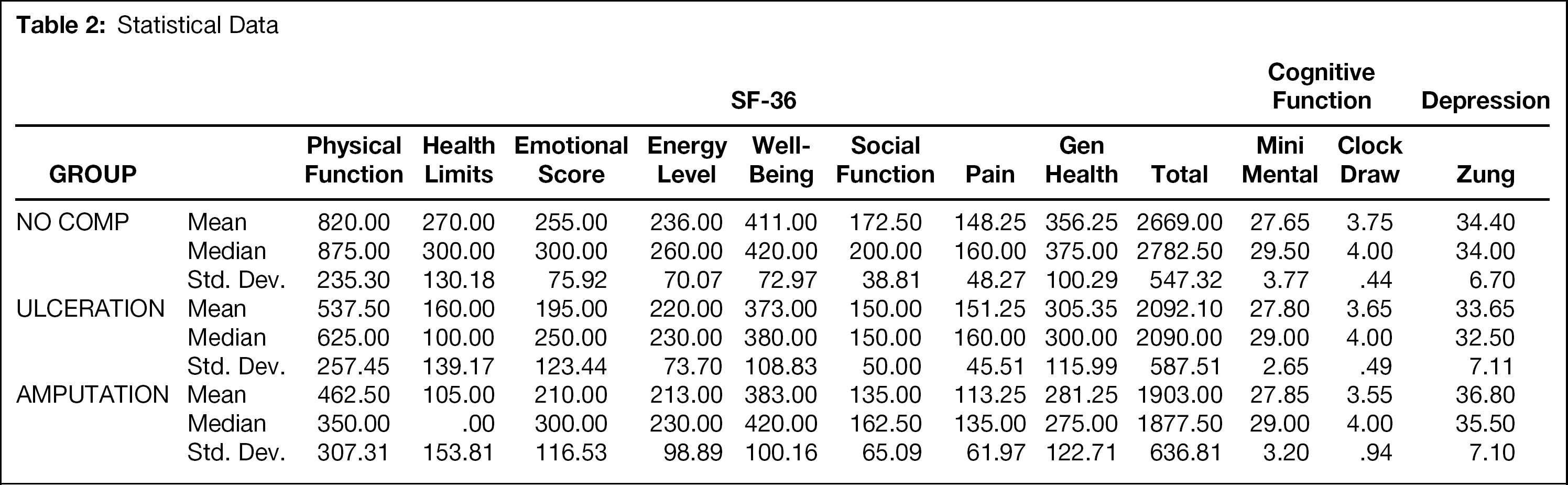
Statistical analysis was performed using SPSS v.10 software (SPSS Inc., Chicago, Il). Medians, means, and standard deviations were computed for each group (Tables 1-2). Differences between groups were tested for statistical significance using the Mann-Whitney test (Table 3). Significance was noted at p <= 0.05.
Results
In this preliminary study, patients in the diabetic foot ulcer and Charcot arthropathy group and the lower extremity amputation group displayed a decrease in perceived functional status and quality of life on the SF-36 Health Survey. Health-related quality of life scores were significantly lower in both the diabetic foot ulcer and Charcot arthropathy group (p < 0.001) and amputee (p < 0.000) group than in the control group (Figure 2). The negative impact on health-related quality of life was not statistically different between the two focus groups (p < 0.314), indicating that there was an equal contribution to the decrease in health-related quality of life in both. Both physical functioning and limitations because of health in both the foot ulcer and Charcot arthropathy group and amputee group were significantly (p < 0.05) different from the control group. There was no statistical difference between the two focus groups in these specific categories, nor was there any evidence of cognitive impairment or depression in either focus group.
Discussion
The results of this preliminary pilot study suggest that diabetic individuals who develop foot ulcers or Charcot arthropathy or have lower extremity amputation may perceive their quality of life to be equally impaired by their health conditions. This data supports earlier studies that have indicated that lower extremity amputation may be correlated with decreased physical and psychosocial functioning. 17 Using these simple screening tools, we found that impairment in cognitive function was no worse in the two focus groups than in the control group with no foot morbidity but with evidence of peripheral neuropathy. Clinical depression did not appear to play a substantial role. This was surprising because individuals with diabetes have been shown to have a predisposition to both depression and cognitive impairment. 5,8
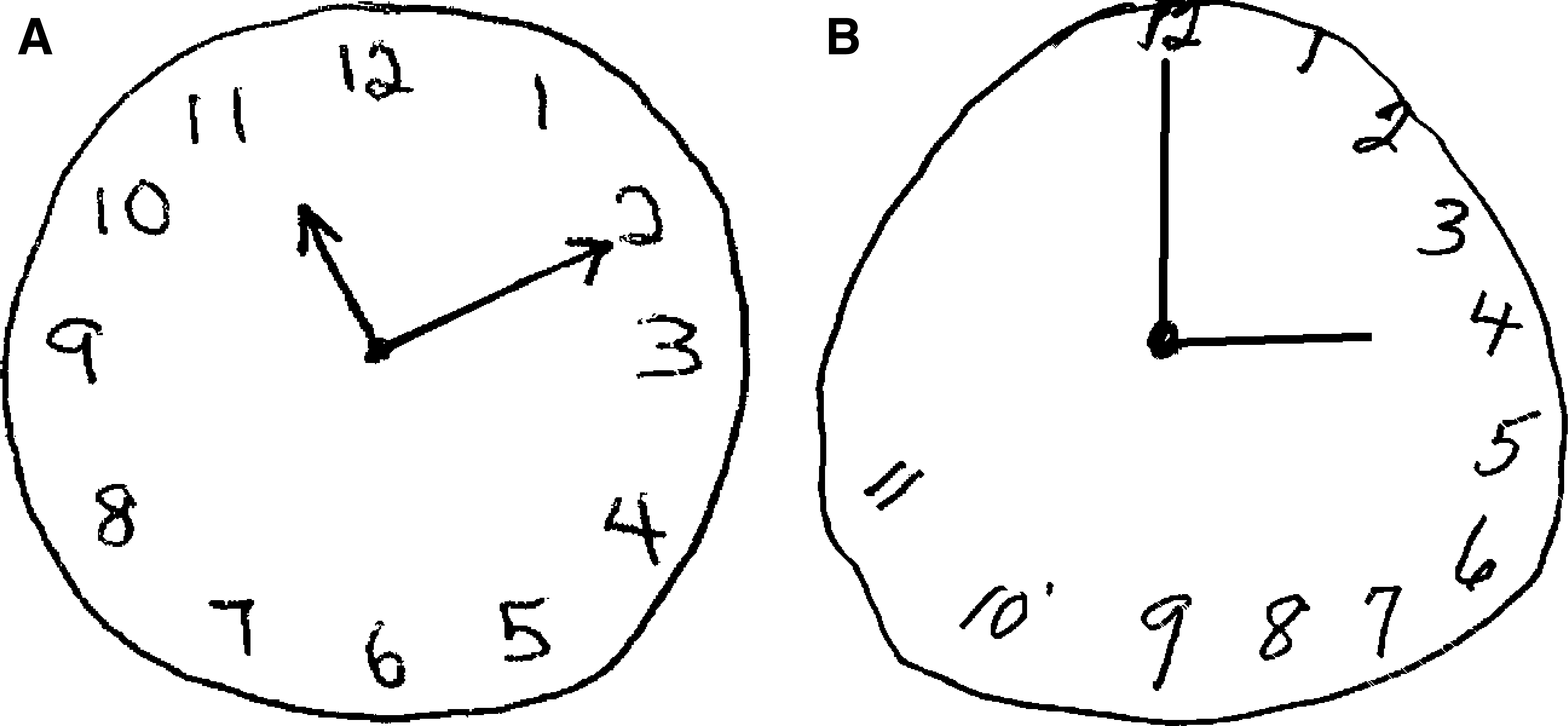
The Clock-Drawing Test was one of the two screening tests used to evaluate cognitive function (see text). The subject who drew the clock on the left (A) received all four points. The clock on the right (B) exhibits significant cognitive impairment
Mean Survey Score Comparison
Statistical Data
Statistical Comparison Of Scores (p values)
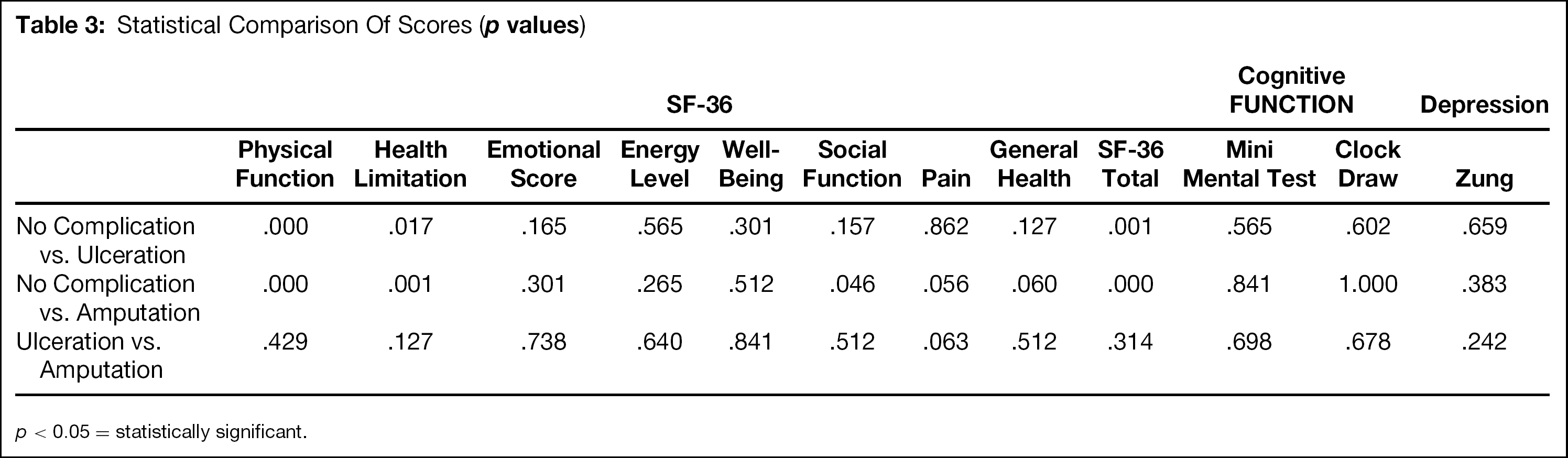
p < 0.05 = statistically significant.
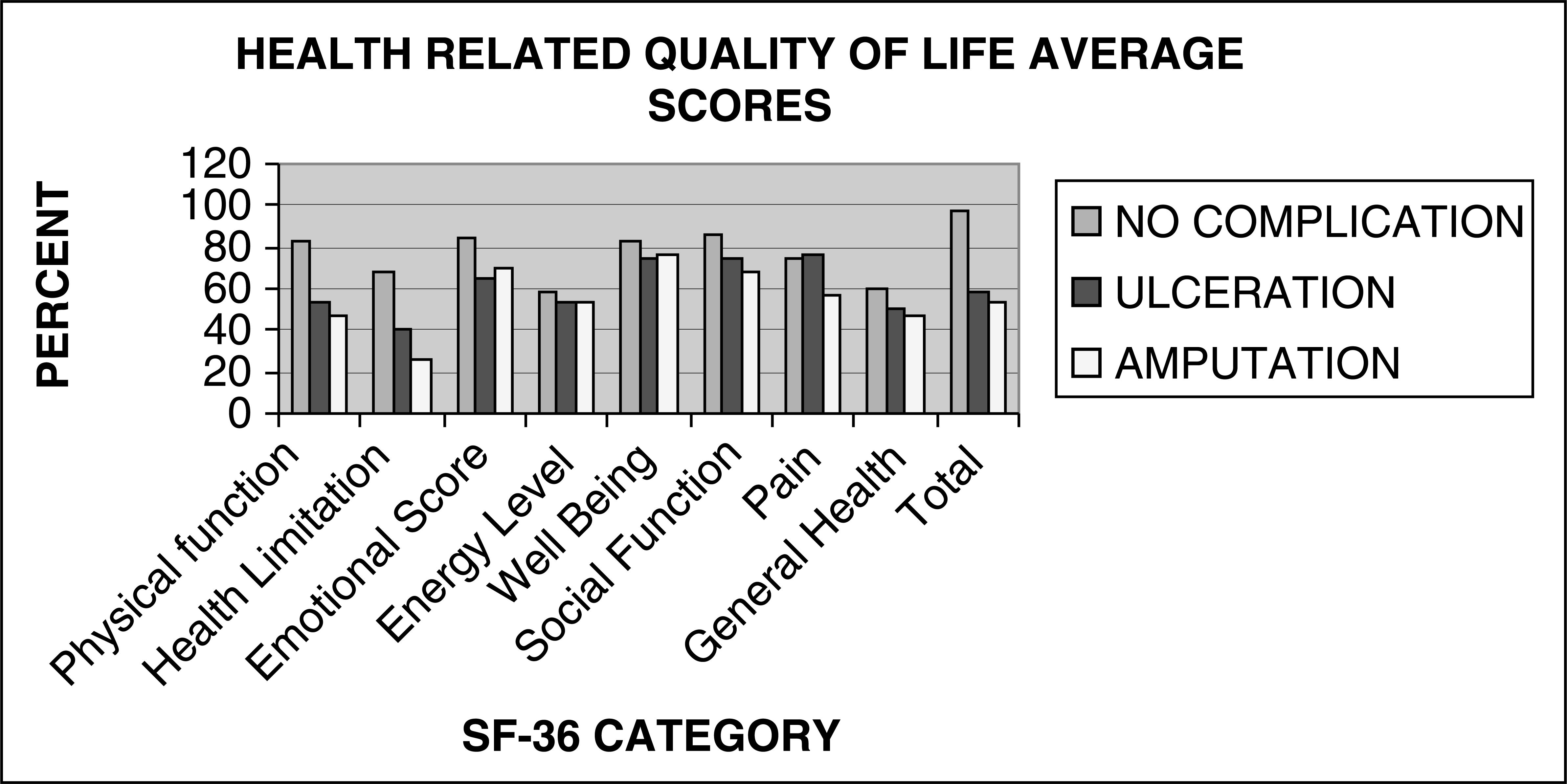
Significant impairment shown in both the diabetic foot ulcer and Charcot arthropathy group and amputee group compared to the control group
The limitations of this study include the small population size, lack of knowledge concerning length and control of diabetes, and lack of segregation regarding level of amputation or duration of ulceration. This investigation was used as a pilot to determine if the study instruments were discriminative. The next step in this project will be to improve the power of the study by narrowing the inclusion and exclusion criteria for study participants in the focus groups and increasing the number of study participants.
While not providing clear answers, the results of this pilot study raise several interesting questions. The information obtained from this investigation did not agree with the currently held belief that there is an increased incidence of depression in individuals with diabetes. This will require further study with a larger number of participants. The similar magnitude of effect on health-related quality of life for both patients with diabetic foot ulcers and lower extremity amputations can be interpreted from two perspectives. The most obvious is the under-appreciation of the effect that diabetic foot ulcers have on patients' perception of health-related quality of life. An alternative explanation would suggest that individuals with diabetic foot ulcers are actually the same population as diabetic individuals who have had amputations, differing only by being at different locations on the time-line of their disease. The appreciation that diabetic foot ulcers may have a similar negative effect on health-related quality of life as lower extremity amputation should provide a new perspective on the disease process and its associated complications.