
Abstract

Introduction
Detection of an ankle syndesmosis injury is important because it can cause a longer recovery time and more disabling symptoms than the more frequent lateral ligament sprain. 1,5 Syndesmosis injuries have been reported to be more common than previously suspected. 4,6
Four tests have been described for detecting syndesmosis injury: the squeeze test, the external rotation test, syndesmosis ligament palpation, and the passive dorsiflexion test. 1,2,4,5 We describe another test for examination of the syndesmosis injury.
The crossed-leg test mimics the mechanism of the squeeze test, but avoids some of its disadvantages: the pivot point where the leg is squeezed may be inconsistent among different examiners and the test is difficult and requires more power for pressure in large legs. Alonso et al. 1 reported that the interrater reliability of the squeeze test is moderate (Kappa = 0.50) and that the external rotation test was the most reliable of the four tests. We have found, however, that the external rotation test is difficult to use in patients with acute injuries because of excessive swelling and tenderness. In these patients, manipulation of the ankle joint caused pain and the results of the test did not indicate the true pathology. Variations in the way the external test is done also compromise its reliability.
Major advantages of the crossed-leg test (Figure 1) are (1) the test is natural and requires no manipulation, (2) because the test is self-administered by the patient, inter- and intra-observer differences are avoided, (3) the test uses gravity and the pair-force of gravity (forces exist in pairs — action and reaction), and (4) the size of the leg has no effect on the result. Since the test is difficult in patients with knee or hip pathology, it should not be used in these patients.
The crossed-leg test has been used in our clinics since 2001, and nine patients with syndesmosis injuries without fractures have been evaluated. Radiographically, the integrity of the syndesmosis was evaluated in external rotation by measuring the space between the tibia and fibula 1 cm proximal to the plafond. 3 Seven of the nine patients had abnormal radiographs, and two had no abnormality on stress radiographs but had positive crossed-leg tests. The squeeze test and external rotation test also were done, 2,4 and all three tests were repeated weekly until recovery as defined by Alonso et al. 1
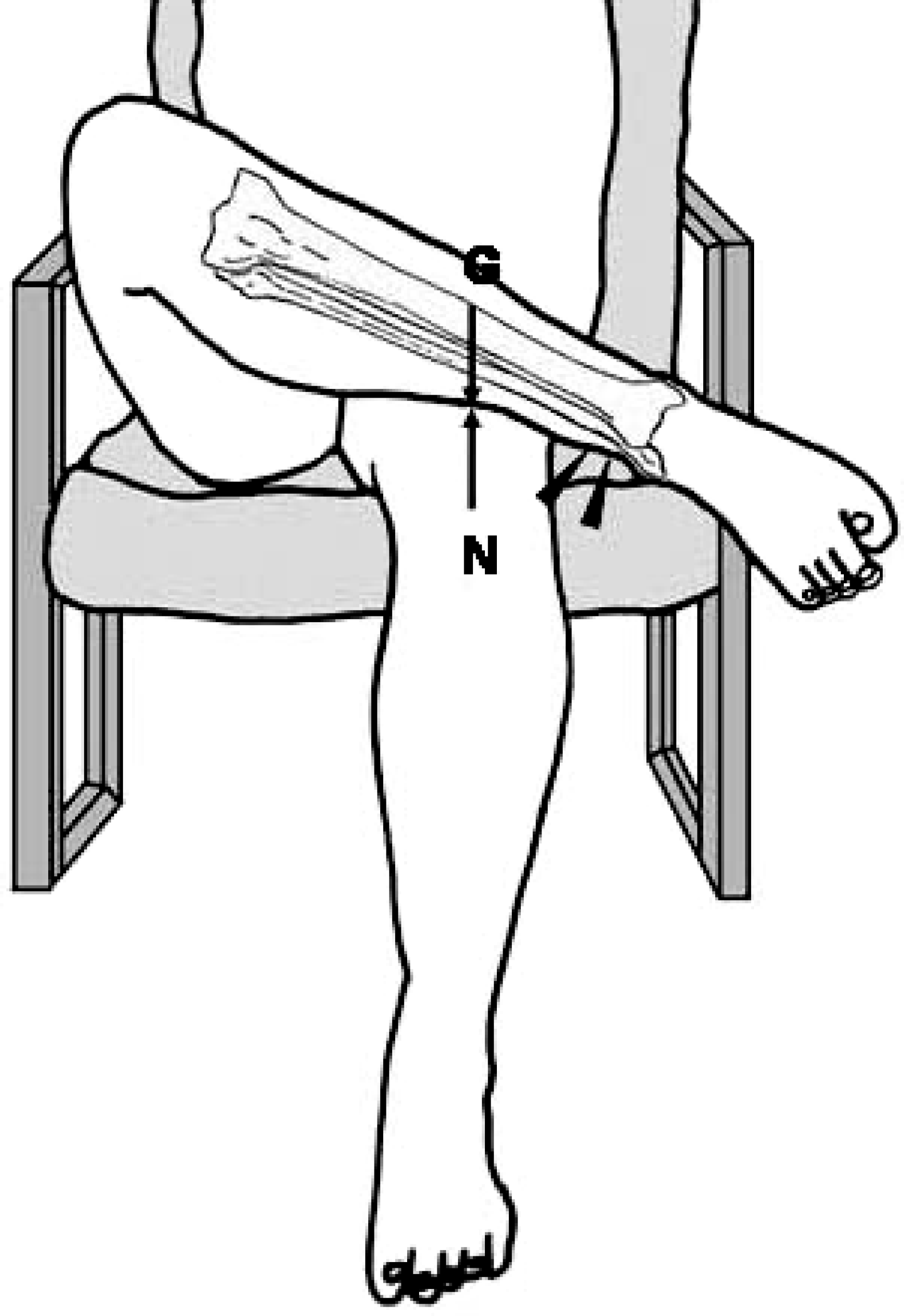
Crossed-leg test position. The test is positive if pain is produced in syndesmosis area (arrow heads) when pressure is applied to the medial side of the knee. G = gravity, N = pair force of the gravity.
The crossed-leg test was positive in all patients at both the first examination immediately after injury and the control examination 1 week later. The external rotation test was unclear at first examination of two patients because of excessive swelling and tenderness at the lateral area of the ankle and pain produced by any ankle movement. The external rotation test was positive in the other seven patients at the first examination, and it was positive in all patients at the control examination 1 week later. The squeeze test was negative in two patients at the first examination. At the repeat examination, it was negative in the same two patients plus an additional one. Recovery was prolonged in all patients, with an average time to return to full activity without functional restriction of 31.7 days.
Technique
The patient is seated in a chair, and the physician demonstrates the correct position. The patient places the leg to be tested across the kneecap of the other leg, with the pivot point at the junction of the middle and distal thirds of the tibia (Figure 1). When the patient applies a gentle force with his or her hand on the medial side of the knee, pain in the syndesmosis area is a positive result, indicating syndesmosis injury.