
Abstract
Background: Bone, soft-tissue, and nerve deficits of the weightbearing surface of the foot are frequent sequelae from foot trauma or diabetes mellitus and present challenging treatment issues. Injury to the specialized, shock-absorbing, heel-pad tissue containing spirally arranged fat chambers is particularly difficult to manage. Appropriate footwear modifications and shoe inserts for protection of this skin are essential to the long-term management of bone and soft-tissue defects of the heel. This study evaluated the performance of a new custom total contact foot orthosis (Hindfoot Containment Orthosis, HCO) which was designed to contain the soft tissues of the heel, reduce shear forces, redistribute weightbearing load, and accommodate bone or soft-tissue deformity of the heel. Methods: Twenty-two patients treated with HCO were retrospectively reviewed. Followup averaged 26 months. The effectiveness of the orthosis was assessed by how well the integrity of the soft tissue was maintained (e.g. the number of ulcerations since dispensing the orthosis), the number of refabrications of the orthosis that were required, and whether or not revision surgery was required. Results: Ten patients had superficial ulcerations. No patient required revision surgery. A total of 62 refabrications of the orthoses in 22 patients were required over a 2-year period. Overall results were good in 17 (77%) patients, fair in four (18%), and poor in one. Conclusions: The HCO is effective for preservation of soft-tissue integrity of the heel pad after bony or soft-tissue injury. Important factors in achieving success with the HCO are patient compliance and periodic monitoring for refabrication of the orthosis to accommodate skeletal growth, change in foot size or shape, and compression or wear of insert materials.
INTRODUCTION
Bone, soft-tissue, and nerve deficits of the weightbearing surface of the foot are frequent sequelae from foot trauma or diabetes mellitus and often are difficult to treat. Injuries to the soft tissues of the heel are particularly difficult to manage. 9,12,13
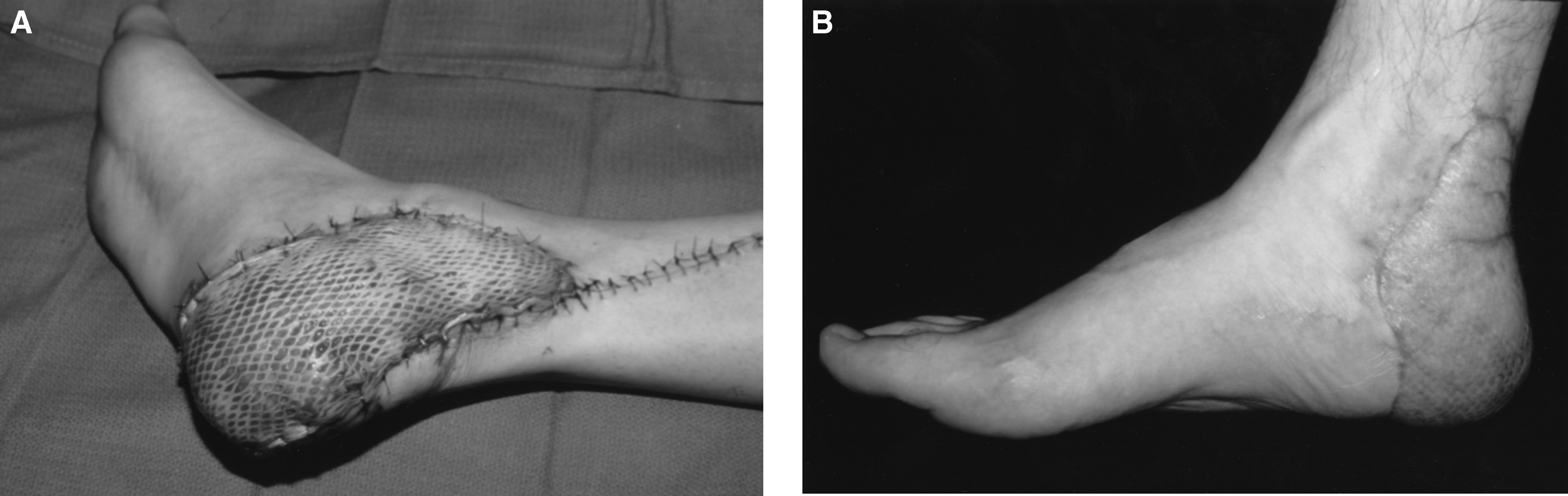
Recent advances in microsurgical vascularized free-tissue transfer have provided a solution for incompetent or absent soft tissue of the heel. 1,3,4,7,8,14,19 However, these flaps have variable sensibility, depending on the type of flap used, and frequently there is concomitant absence of protective sensation (Figure 1). 2,5,10 Soft-tissue defects and bone deformities of the heel covered with local flaps, split-thickness skin grafts, or scar tissue may be at even greater risk of breakdown from the weightbearing loads and the shear forces of ambulation. 2,16 Appropriate footwear modifications and shoe inserts for the protection of this skin are therefore essential to the long-term management of bone and soft-tissue defects of the heel. 2
This study evaluated the performance of a new custom total contact foot orthosis (Hindfoot Containment Orthosis, HCO) which was designed to contain the soft tissues of the heel, reduce shear forces, redistribute weightbearing load, and accommodate bone or soft-tissue deformity for the treatment of bone and soft-tissue deficits of the heel.
MATERIALS AND METHODS
Twenty-two (22) patients treated with a hindfoot containment orthosis (HCO) for either bone deformity, soft-tissue defect, or peripheral nerve injury were retrospectively reviewed (Figure 2). There were 14 males and eight females with an average age of 32 (range 5 to 69) years. Followup averaged 26 (range 5 to 54) months. Causes of bone or soft-tissue defects of the heel that required use of the HCO are listed in Table 1. The effectiveness of the orthosis was assessed by how well the integrity of the soft tissue was maintained (e.g. the number of ulcerations since dispensing the orthosis), the number of refabrications of the orthosis that were required, and whether or not revision surgery was required.

Diagnoses requiring use of the Hindfoot Containment Orthosis
HCO Fabrication Technique
The foot of the patient is placed into as near to neutral position as possible and a negative foot impression is taken using a plaster bandage wrap and the “slipper-mold” technique. 6,11,17
The slipper mold incorporates as much of the abnormal heel soft tissue as can be contained by a high-top, in-depth shoe.
A positive model is produced in plaster from the negative mold.
Modifications to the cast are made as necessary to relieve the prominences and insure a total contact fit.
One-quarter inch No. 1 Plastazote® (Zotefoams, Inc; Croydon, England) sheet stock is cut large enough to sufficiently cover the entire surface area of the positive model and extend around the entire heel to cover all free tissue flaps or skin grafted areas.
The Plastazote® is heated until moldable and then vacuum-formed over the model. Care must be taken to eliminate any wrinkling of the Plastazote® in the skin contact areas (Figure 3, A).
Viscoelastic polymer is added to the underside of the Plastazote® lining to fill any void caused by deformity or where maximal shock absorption is needed (Figure 3, B).
A small dam is placed around the perimeter of the heel of the cast to contain the liquid form of the viscoelastic polymer.
The polymer is mixed to a consistently soft density, and the heel is covered in the liquid polymer. After setting, the polymer is trimmed to a uniform thickness of approximately 3/8 of an inch.
Stabilization of the Plastazote® lining and viscoelastic polymer filler is provided by layering fiberglass on the underside of the orthosis proximal to the metatarsal heads.
The fiberglass is extended over the heel posteriorly, medially, and laterally creating a high-walled, heel-cupping effect. Excess fiberglass is removed with a cast saw, and the edges are smoothed with a grinder or sander.
The edge of the fiberglass is trimmed 1/4 inch lower than the trim line of the Plastazote® to prevent abrasion of the skin by the edge of the fiberglass. A facemask is used when grinding fiberglass to prevent airborne inhalation of fiberglass particles.
A 1/2-inch thermal cork is used to post the heel for medial and lateral stability and to flatten the bottom of the heel for proper shoe fit. As the final trimming is done, care is taken to contain as much of the abnormal heel soft tissue, free flap, or skin grafted area as possible within the orthosis and shoe (Figure 3, C).
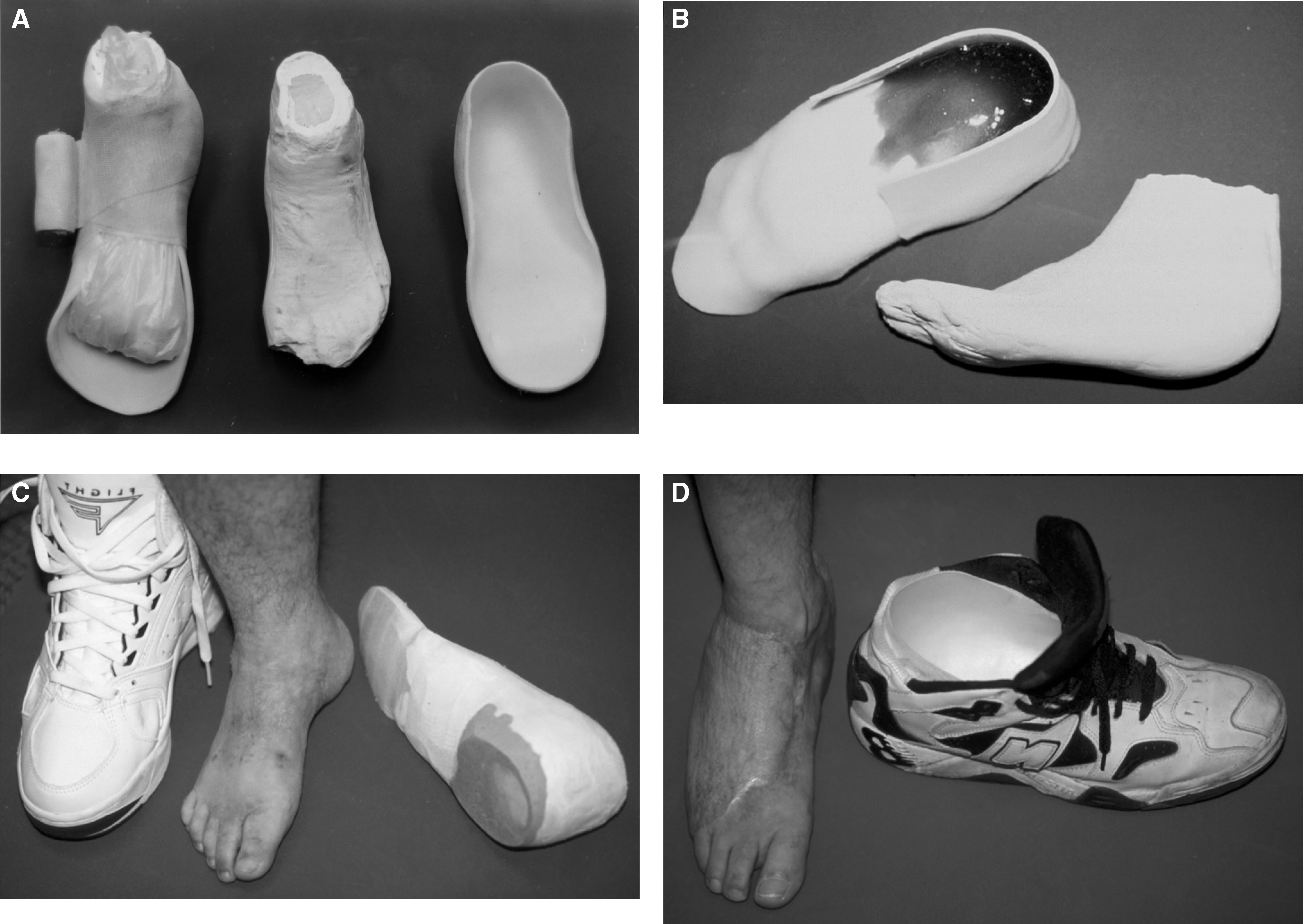
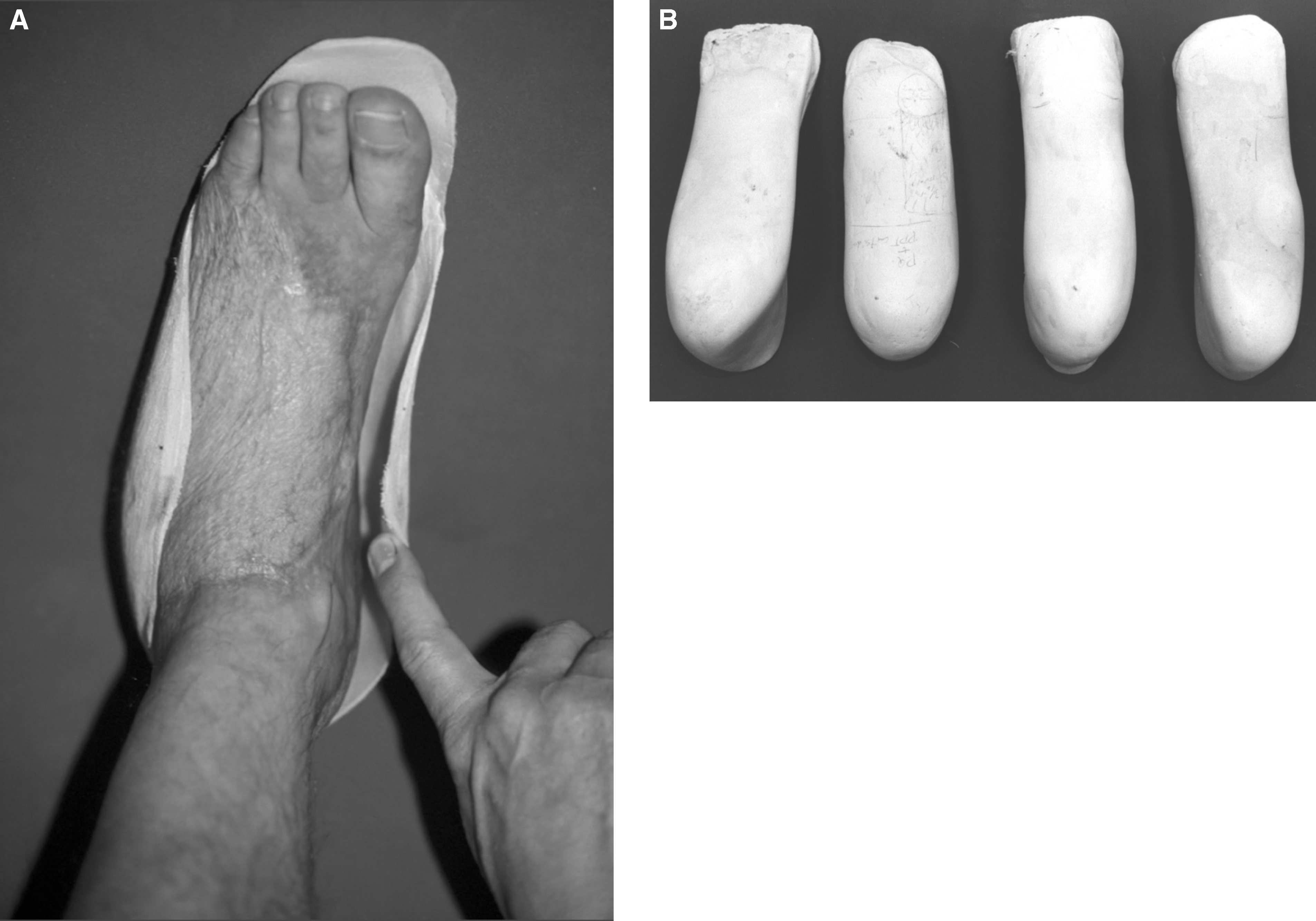
Once the soft tissues of the heel healed adequately for weightbearing, a well-conforming, short-leg, total contact cast was applied and worn for 2 to 4 weeks while the patient became fully ambulatory. Then the patient was transitioned to a removable walker boot, and the first HCO was fabricated and placed inside the footplate. As the patient improved, an appropriate in-depth shoe was used that accommodated the foot and the HCO. High-top athletic shoes with removable insoles were popular choices by the younger patients in our study group (Figure 3, D). During the initial 6 months of treatment, a few patients required mismated shoes to accommodate the bulk of the soft tissues as well as the orthosis. However, at the time of followup, no patients required mismated in-depth shoes because of the bulk of the orthosis. External shoe modifications including rocker soles, sole flares, and extended steel shanks were applied on an individual basis but were not routinely required. Refabrication of the orthosis over the original, or a new mold of the foot, was recommended periodically because of the limited lifespan of the soft Plastazote® and the gradual change in shape and size of the foot after major injury or free-tissue transfer (Figure 4, A and B).
RESULTS
Skin Ulceration
Twelve patients (55%) had no ulceration or skin breakdown with their chosen level of activity over the followup period, which averaged 28 months for this group. The remaining 10 patients (45%) developed at least one superficial ulceration during the followup period that averaged 24 months in this subset. No deep ulcers below the level of the dermis occurred. The 10 patients in the reulceration group had a total of 21 ulcerations (range 1 to 4) over the followup period with an average of one ulceration per patient per year of followup. All of the ulcerations were superficial and did not extend to bone or tendon.
The major contributing factor causing reulceration was noncompliance in wearing the HCO or not replacing it when anticipated wear occurred.
Frequency of Revision Surgery
No revision surgeries for reulceration were required except for planned flap debulking in some patients with redundant soft-tissue flaps.
Orthosis Refabrications
A total of 62 HCO refabrications were required during the average 2-year followup period in the 22 patients studied. Thirty-two (52%) were refabricated over a new mold of the foot because of a change in size or shape of the heel that adversely altered the total contact fit. Thirty (48%) were refabricated over the previous mold of the foot because the insert materials had worn out or compressed to significantly reduce the effectiveness and comfort of the orthosis. All patients who had worn the HCO for 1 year or more required at least one refabrication. Variability between patients in the number of remakes was dependent upon skeletal growth, activity level, and phase of treatment. Growing children, physically active patients, and those with significant postinjury or postoperative swelling required additional refabrications to accommodate the continued changes in the shape of the heel deformity.
Overall Satisfaction
Seventeen (77%) patients were determined to have good results based on return to a moderate or unlimited level of activity. A moderate activity level was defined subjectively by the patient and treating physician as the ability to participate in most desired activities of daily living but with limitations. This clearly is a potential flaw in the study because of the opportunity for detection bias. Four patients (18%) had fair results and one (5%) patient had a poor overall result. However, the latter was complicated by a comorbid lumbosacral-level paraplegia with insensitivity of the plantar foot causing a neurotrophic painful heel ulcer. In addition, this patient was noncompliant with wearing the orthosis or appropriate accommodative footwear.
DISCUSSION
After injury to the heel pad or free-flap coverage of the calcaneus, the resulting tissue lacks the shock-absorbing and shear accommodating qualities of the normal heel pad. Free muscle transfers atrophy over time, which reduces the thickness of the tissue and creates a redundant, hypermobile tissue envelope over the calcaneus. 17 During the gait cycle, this tissue is susceptible to ulceration from localized pressure over areas of bony prominence or from excessive shear forces due to hypermobility.
A standard solution to the problem of an insensate or deficient heel pad or bony deformity of the heel is the use of cushion-soled shoes, with some type of heat-moldable material for the insole. 6,11,15,18 The concept of the HCO differs from these types of inserts in two ways. The HCO has a high heel cup built into the insole, similar to the University of California Berkeley Laboratory (UCBL) orthosis, but extends higher around the sides and back of the heel to cover a larger area of compromised soft tissue than the UCBL. The second unique feature is a trilayer construction with moldable foam and viscoelastic polymer reinforced with a shell of fiberglass. The soft, heat-moldable, closed-cell polyethylene foam (Plastazote®) provides a “total contact” fit over the entire deformity or compromised area of the heel and sole. The viscoelastic polymer is considered to have superior shock-absorbing and shear force-relieving properties. 16 This material is placed underneath the plantar aspect of the Plastazote®liner to protect areas of bony prominence or potential skin breakdown. This composite is covered with a stiff shell of fiberglass to prevent excessive deformation or bottoming out of the viscoelastic polymer and to contain the soft tissues of the heel by holding the bulk of the soft tissue centered beneath the weightbearing area of the calcaneus.
Determining how this design of orthosis affects the soft-tissue biomechanics or the distribution of load-bearing forces on the plantar aspect of the foot was not the purpose of this study. However, despite a lack of understanding of the mechanism by which this orthosis functions, the results of this study suggest that the HCO is an effective device to relieve pain and prevent or reduce skin breakdown in patients with soft tissue or bony deformity of the heel. The use of the HCO is especially helpful when the heel deformity is associated with diminished or absent sensation.
In the first 6 to 12 months after a severe injury to the hindfoot or after a free vascularized tissue transfer to the heel or sole, the volume and shape of the foot change significantly as the posttraumatic edema resolves and the denervated, transferred muscle flap undergoes atrophy. During this time, it is important to remake the HCO over a new mold of the foot to preserve the total contact fit because significant changes in size or volume of the foot occur. Growing children also need periodic remakes to accommodate the changes in foot size. Active or overweight patients tend to compress the moldable materials quickly and require more frequent monitoring by the certified pedorthotist or surgeon to prevent skin breakdown over high-pressure areas. Recognition by the clinician of the need for these periodic refabrications represents not only an important technical point with regard to HCO maintenance but reflects the clinical issues involved with the dynamic changes in the heel size and shape over time in this patient population.
Based on the results of this study, we recommend remaking the orthosis at least yearly in all patients and more frequently in patients who are very active or within 1 year of surgery or injury.