
Abstract
Background: The proximal crescentic osteotomy is an effective technique for correcting a widened 1–2 intermetatarsal angle associated with moderate to severe hallux valgus deformities. However, postoperative dorsal malunion at the osteotomy site from loss of fixation has been reported. The purpose of this study was to evaluate the biomechanical characteristics of a new custom-designed plate and compare it to the traditional screw and Kirschner wire construct. Methods: Twenty identical Sawbone® (Pacific Research Laboratories, Vashon, WA) models were used for the study. A proximal crescentic osteotomy was done on each specimen, and 10 were secured with a dorsomedial plate (group I). The remaining 10 models were fixed with a screw and Kirschner wire combination (group II). Physiologic cyclical testing was done using a mechanical testing machine to evaluate dorsal displacement of the metatarsal. Load-to-failure testing was then done on each specimen to evaluate ultimate failure and stiffness of the constructs. Groups I and II were statistically compared using paired t-testing. Results: The mean dorsal displacement of the first metatarsal head after 1000 cycles was 0.19 mm (SD = 0.09 mm) for group I and 0.28 mm (SD = 0.15) for group II, and the difference was not statistically significant (p = 0.08). Group I demonstrated statistically superior ultimate failure strength (95.2 N) and stiffness (26.8 N/mm) compared to group II (73.7 N, 19.4 N/mm). Conclusions: Based on Sawbone® models, dorsal plate fixation of proximal crescentic osteotomy provides a stronger construct than the traditional screw and Kirschner wire construct. The clinical use of the specially-designed plate described in this study may lower the incidence of dorsal malunions that occur postoperatively and may decrease the occurrence of transfer metatarsalgia. Its application may be particularly helpful in patients with poor bone quality.
INTRODUCTION
Moderate to severe hallux valgus deformities with wide 1–2 intermetatarsal angles may be treated effectively with a proximal metatarsal osteotomy and distal soft-tissue reconstruction. 2 Many types of osteotomies have been described, and the advantages and disadvantages of each have been reported. 2,14,15 The proximal crescentic osteotomy, first described by Mann, 9 provides reliable correction of metatarsus primus varus, 11 and the reported patient satisfaction rates after this procedure generally are high. 5,9,16,18
Many authors 1,4,7,10,12,14,15,17 have expressed concern about the risk of dorsal malunion and subsequent transfer metatarsalgia after the crescentic osteotomy, and the reported rate of hallux elevatus may be as high as 28% 9 . Using Sawbone® models with three-dimensional tracking, Nyska et al. 11 demonstrated that the proximal crescentic osteotomy does not result in significant elevation of the first metatarsal head when done correctly. Dorsiflexion at the osteotomy site is likely a result of intraoperative technical error 5,8,9 or loss of fixation postoperatively. 1,12,16 Specific problems have been noted with early hardware removal, 18 noncompliant patients, 1 inadequate internal fixation, 16 and osteopenic bone. 15
Cadaver studies and mechanical testing of the crescentic osteotomy have shown that the construct, when fixed with a single screw, is weaker than other commonly used proximal and shaft first metatarsal osteotomies. 1,10,17 Rosenberg and Donley 13 described the use of a 2.7-mm semitubular dorsal plate to augment the strength of fixation of the crescentic osteotomy for selected patients when single-screw fixation was deemed inadequate. To our knowledge, there have not been any published biomechanical reports on the strength of dorsal plate fixation of the proximal crescentic osteotomy.
The purpose of this study was to compare the strength of a specially designed dorsal plate to that of a screw and Kirschner wire construct for fixation of proximal first metatarsal crescentic osteotomies. Our hypothesis was that plate fixation would demonstrate superior mechanical properties.

Custom-designed plate applied across osteotomy along dorsomedial aspect of the base of the first metatarsal.
MATERIALS AND METHODS
Twenty identical Sawbone® models (Pacific Research Laboratories, Vashon, WA) were used for the study. Each model was made of solid foam and consisted of a first and second ray with moderate hallux valgus deformity (hallux valgus angle = 20 degrees) and a widened 1–2 intermetatarsal angle (1–2 IM angle = 11 degrees).
A crescentic osteotomy was done on each Sawbone® specimen using a pneumatic oscillating microsagittal saw (MicroAire Surgical Instruments, Charlottesville, VA) and a curved blade (#5053–176; Zimmer, Warsaw, IN). The saw was attached to a drill press (Ryobi Technologies Inc., Anderson, SC) with a custom-machined coupling device to ensure accurate and reproducible cuts. The saw blade was aligned perpendicular to the long axis of the first metatarsal, and the concavity of the cut was directed proximally at a point 15 mm distal to the first metatarsocuneiform joint. The distal first metatarsal was then displaced laterally across the osteotomy site to correct the 1–2 intermetatarsal angle. Each specimen underwent the same amount of correction, which was ensured by marking and measuring the amount of displacement that occurred at the osteotomy site.
The first 10 specimens were designated group I, and fixation of the osteotomy site consisted of a specially-designed titanium plate (Newdeal, Lyon, France) applied on the dorsolateral aspect of the base of the first metatarsal and secured with four 2.7-mm screws (Figure 1). For the remaining 10 specimens (group II) the osteotomy was secured with a 3.5-mm cortical screw and a .062-inch Kirschner wire applied dorsal-distal to plantar-proximal.
Biomechanical testing was done at the Department of Trauma, Hand, and Reconstructive Surgery, University Hospital Munster. The first metatarsocuneiform complex was mounted on a uniaxial testing frame (MTS, Zwick/Roell Z005/TN2A, Ulm, Germany). Each specimen was inclined 15 degrees to the axis of the diaphysis as described by Trnka et al. 17 to simulate anatomic position, and all loads were applied to the plantar aspect of the metatarsal head and directed dorsally in a cantilever-bending mode with a moment arm of 7.5 cm (Figure 2).
Cyclical testing was done with a load of 27 N, equivalent to 70% of the static failure load of the weakest construct. Each specimen underwent 1000 cycles, the frequency of loading for a physiologically normal lower limb per day. Each cycle was recorded and dorsal displacement of the first metatarsal head was measured with the tranverse path sensor of the Zwick Machine.
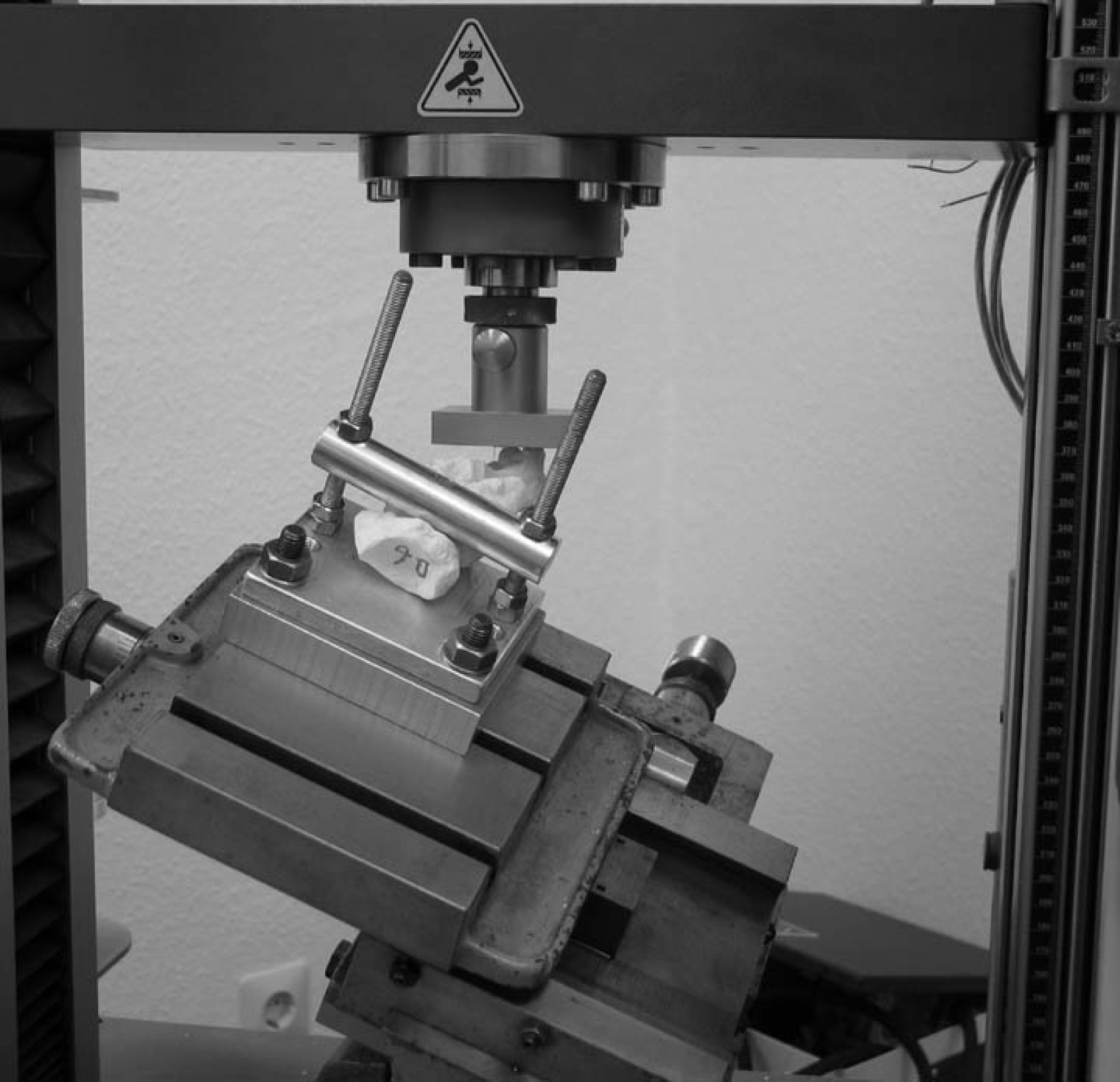
Testing apparatus with dorsally directed force applied to metatarsal head.
After cyclical testing, a load-to-failure test was done. Load was applied at a rate of 120 mm/min until failure was noted. Ultimate strength was defined as the peak load preceding a sharp decrease in the load-displacement curve. Load-deflection curves were continuously recorded, and the ultimate failure was measured as units of force (N). Stiffness was determined from the linear region of the load-displacement curves and recorded as N/mm.
Data collection during mechanical testing was done using testXpert V10.11 (Zwick/Roell, Ulm, Germany). Statistical analysis was completed using Microsoft Excel (Microsoft, Bellevue, WA). A two-tailed student's t-test was used to compare results from groups I and II, and p values less than 0.05 were considered significant.
RESULTS
All of the specimens in group II (screw and Kirschner wire fixation) failed the same way. In every case a fracture occurred through the screw hole adjacent to the screw head. The specimens in group I (plate fixation) broke in different ways, but all of them broke with a fragment between the screws and the osteotomy site. In one case it was a distal fragment, and in all the other cases the broken fragment was proximal (Figure 3). One specimen in group II was excluded for technical difficulties involving the testing machine.
The average load-displacement curves for the two groups were determined (Table 1). The mean dorsal displacement of the first metatarsal head after 1000 cycles was 0.19 mm (SD = 0.09 mm) for group I and 0.28 mm (SD = 0.15) for group II. The osteotomies fixed with the plate tended to have less displacement, but it was not quite statistically significant (p = 0.08). The mean load-to-failure for group I was 95.2 N (SD = 12.2) and 73.7 N (SD = 24.6) for group II. The difference in the means was statistically significant (p = 0.03). The average stiffness for group I (26.8 N/mm, SD = 4.9 N/mm) was significantly (p = 0.01) greater than the stiffness for group II (19.4 N/mm, SD = 6.6 N/mm).

Typical mode of failure of plate construct with fracture proximal to osteotomy.
DISCUSSION
Although first metatarsal proximal crescentic osteotomy is capable of providing significant correction of a widened 1–2 intermetatarsal angle, the reported rates of dorsal malunion are a cause of concern. Lippert and McDermott 8 and Jones et al. 6 demonstrated the importance of sawblade orientation and noted a positive correlation between hallux elevatus and medial-to-lateral coronal tilt of the osteotomy using foam metatarsal models. Nyska et al., 11 using a three-dimensional digitized tracker and Sawbone® models, confirmed that no significant elevation of the first metatarsal occurs when the proper osteotomy technique is used.
Biomechanical comparison between plate (group I) and screw and Kirschner wire (group II) constructs
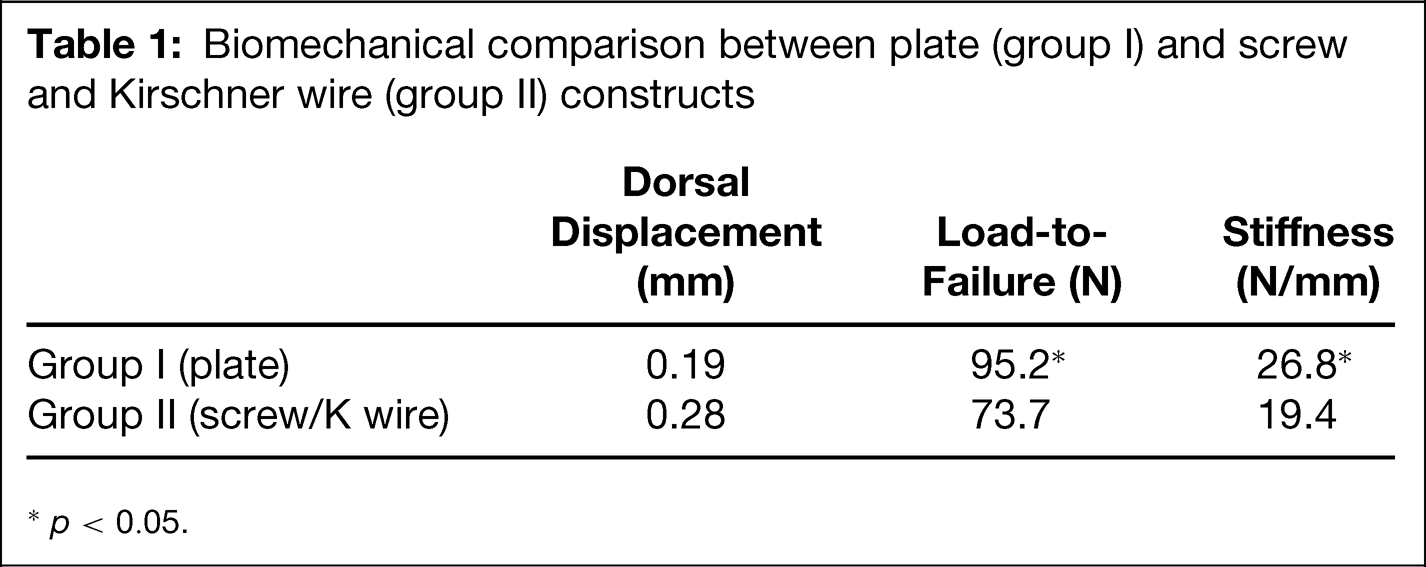
p < 0.05.
Even in the absence of intraoperative technical error, dorsal malunion may occur postoperatively from a loss of fixation related to poor bone quality, 15 inadequate internal fixation, 16 or patient noncompliance. 1 The geometry of the crescentic bone cut is relatively unstable. The proximal location of the first metatarsal osteotomy results in a long lever arm, and less dorsiflexion force is required to generate a significant moment at the osteotomy. The osteotomy is typically secured with a single 3.5-mm cortical or 4.0-mm cancellous screw applied dorsal-distal to proximal-plantar. 5,9,12,16,18 Mechanical testing of this construct has confirmed that it is weaker than most other described proximal and shaft metatarsal osteotomies. 1,10,17 Trnka et al. 17 compared the strength of the crescentic osteotomy fixed with a single screw in a cadaver model to the normal pressures under the first metatarsal head during ambulation in healthy volunteers. Based on their analysis, the construct was not strong enough to withstand early weightbearing postoperatively. 17
To provide stronger fixation and obtain better rotational control, a Kirschner wire can be used in addition to a screw for fixation of a crescentic osteotomy. 3,5 Alternatively, Rosenberg and Donley 13 described the use of a dorsal 2.7-mm semitubular plate with a single lag screw across the osteotomy and suggested that this provides stronger fixation than the screw and Kirschner wire construct. They further theorized that this might help prevent intraoperative dorsiflexion of the osteotomy by better aligning the dorsal surfaces of the proximal metatarsal. 13 To our knowledge, mechanical testing of dorsal plate fixation has not been previously published.
The results of this study demonstrate that dorsal plate fixation of a proximal first metatarsal crescentic osteotomy in a Sawbone® model is a stronger and stiffer construct than a screw and Kirschner wire combination. Foam models were used to ensure consistency in shape, size, and length of the metatarsal. To simulate proper anatomic position and physiologic conditions, the metatarsal models were inclined 15 degrees, and cyclical loading was done before load-to-failure. The results of group II are similar to those reported by Earll et al. 4 who also used a Sawbone® model.
Comparing our results to other published mechanical studies is difficult because previous investigators have used cadaver specimens and different loading techniques. We did not use cadavers to avoid differences in bone quality and morphology among specimens, which may influence the results. Further mechanical testing of the constructs described in this study using matched pairs of cadaveric specimens may help control these inconsistencies 1,7 and provide more clinically relevant information. However, Sawbone® models are useful for demonstrating relative differences between types of fixation.
Extrapolating the results of this study to the clinical scenario must be undertaken with some caution. However, we do believe that dorsal plate fixation of a proximal metatarsal crescentic osteotomy may decrease the incidence of dorsal malunion related to loss of fixation. We also agree with Rosenberg and Donley 13 that the plate may aid the surgeon intraoperatively by controlling sagittal plane alignment, although proper coronal plane orientation of the sawblade is equally important. 6,8 Clinical studies of the dorsal plate are necessary to confirm our notions, in addition to evaluating differences in operative time, surgical exposure, and costs.